Should I do chest wall rads?

I am perplexed as to why my MO is wanting to radiate my chest wall. I have a <1cm. Lump right by my nipple and 1 affected lymph node. Lump is now gone and node very much smaller after chemo. I will have box and node removal surgery. I understand radiating nodes, but the chest wall? Her only reasoning is that if you get a reoccurrence it is 50% of the time in chest wall. After all of my treatments I just have a 12-14% chance of cancer returning. I am thinking of refusing the chest wall chemo due yo all the damage it can cause. I have had the most a aggressive chemo and surgery for a not so aggressive diagnosis, I just think this is overkill. Thoughts
Comments
-
My experience is that there are protocols for treatment that must be followed, and if you get radiation, you get the standard treatment. If they radiate the axilla, they radiate the chest wall. I had a 3 cm margin between my tumour and my chest wall, but because I was having radiation to the axilla (instead of an ALND following a micromet), chest wall radiation was still part of the treatment. Personally, I had no objection to additional treatment, so I didn't push back on the issue.
-
This may be helpful in understanding the guidelines:
The guidelines are guidelines, you need to be comfortable with the treatment plan.
-
I thought with mastectomy they don't usually do radiation unless margins are too close or something. Hopefully others can help explain but I do know must find radiation to be doabl
-
chemo is to prevent distant recurrence; rads reduces risk of local recurrence. It is ultimately up to you. Perhaps you can get a couple opinions. It is ultimately up to you. Ask them what percentage it lowers your risk. Ask what the risk of rads are. If they do not specifically describe risks, find a different RO. You need to decide if percentage benefit is worth the risks
-
Jiffrig, as Cubbie said, that is standard protocol. I just had the concern as you did. I understand also that full irradiation must be given when the tumor is inside the body but protocols just load you with the same amount even when there is no tumor inside. I still do not understand how can they treat some single cells as if they were organized as a tumorous body of 1 cm or greater. As I said before, they are seeing giants where there are only windmills.
OK, I understand their premise: where there was a tumor, there are still cells that can become a tumor in the future. However, a cancer cell needs the radiation a compact tumor body needs to break and shrink? It is a question of logic. Maybe if physicians evaluate their protocols, there would not be so many post-radiation cancers, fibrosis or necrosis of the breasts, as well as many other severe side effects.
I said in another forum that I objected to my RO so I won't be receiving RT now. I asked her if she could use the partial breast RT with 40 Gy and 16 tx sessions. She said she didn't give PBRT. The other thing I dealt with was axilla irradiation. Due to lymphedema risk, I said I won't let anyone touch my axilla. She didn't like the project but she complied to my request. Anyway, I have physicians I can talk to but I change them if they ignore my concerns, worries or requests. Is my body they are treating, not theirs. I will live with the consequences of my decisions, not theirs. I will live with my own risks, not theirs. And, I once said, I do not go to MDs to make them happy and be compliant. I go to them because I need a health service and they are entitled by the state to do that kind of service. If I don't like the service or the risks are too great to be acceptable, I retract and move away.
The MO stood by my side and told me he would watch my health closely. I accepted gratefully cause I am scared of cancer, any cancer, the one I had and was removed or the one which can grow back as recurrence or due to RT or chemo or whatever thing MDs give me. I am paying them to get well, not to get sick with their treatment.
The best thing is communication with your doctors, your family, your friends. My cards are clear with MDs. My friends know where they stand; they were also stopped from arguing and fighting me because I was too difficult. That I have to comply to MDs. I do when doctors convince me. Otherwise, no. I told my friends all the things I wrote earlier. Besides, I told them that I am the one who makes decisions with my body, not them, and that I want their friendship and companionship, not their critics, in this moment. If they want to stand by me, they are welcome. If they don't, I will understand. They are also free to go. I don't let anyone, not even my brother to decide for me because I am not mentally incapacitated. When I am confused, I ask opinions, look for information; when I decide, the problem with my conscience is solved. I rest my case. Have a good afternoon.
-
Did you have lympho vascular invasion? That seems to get you radiation even after mastectomy. Ask questions specifically why do you need radiation. The benefit from radiation after mastectomy is questionable but the studies do agree that radiation to nodes rather than ALND is better.
-
Yes, I do have one node that they know of. Since writing the first post, I have decided to do a first surgery where the BS takes out all breast tissue and affected nodes. They will put in te's as place holders for DIEP after rads, if necessary. We wlll then evaluate after path on nodes as to necessity of rads. I do notice on this board many of the reoccurrences after mastectomy are on gals who did not have radiation the first time. Evidently 50% of reoccuramces are to chest wall
-
LVI is different from nodal involvement . It means that cancer cells are found in blood vessels and lymph channels in the breast. I just now realize that usually you have that information after the surgery. You could wait for you pathology after surgery and then get 2 opinions. I saw 2 radiation oncologists and they both gave me the same explanation. But the benefit from radiation after mastectomy may be less than 5%.
-
Hello, I am too debating whether I should or shouldn't do radiation. No one seems to give clear cut answer. Sam2u, I read the NCCR guidelines and I just realized that it applies only when the patient had surgery BEFORE chemo or rads. What happened when you had neoadjuvant chemo? The lymph nodes may be cleared but that's because they were blasted by chemo.
Here is my situation: I got dx April 2016 with stage 2b, left breast, 3.3 cm, 1/3 biopsied axillary lymph node, March 26, 2016. Received chemo AC+Taxol (April thru September 01), UMX on 10/5 but margin positive (one single cell on the edge) reexcision was done 10/24 and the pathology came back showing nothing. BS said it sometime happened with a mastectomy. PATH also showed 3 lymph nodes taken out after surgery 10/5 were negative, no tissue left because they were blasted by the chemo. OC said initially I don't need chemo after MX since my tumor was smaller than 5 cm, but she is not sure about the armpit cause the lymph nodes were negative due to (chemo prior to surgery). RO just said I need to do rads but did not say what he based on. The nurse came in talked to me said there is standard reduction of 30% but why don't give me percentage based on my specific situation? OC said I have about 15% recurrence. I went to a second OC for second opinion and after reviewing my history, surgery, and pathology, she said I don't need radiation😯.
So I'm seeking a second opinion from another RO from MD Anderson. However, I'm suspecting all RO encourage people to get radiation so they can get paid. Sorry that's my impression about the cancer treatment system. The reason for that is I have to research in the beginning about almost everything under the sun to help me decide what's good for my body. Drs just want to give you drugs on of drugs and want you to go through the standard of care. Any suggestions?
-
Houston, I agree with you. People are continuously irradiated even though they should develop protocols for post-mx patients. As someone mentioned before the increase on survival for post mx is only 4%. If one weighs the risks versus the gains, and the risks are larger and more serious that we are informed, then we can make a very well informed decision. I have been reading in this site as well as others, about radiation damage and I don't like what I see. I know that not everyone will get serious side effects, but those who get it, their life become more complicated than for those that don't. For a person with necrosis, she could loss her breast or her life if she does not get medical attention on time; for a person who have fibrosis, there is continuous pain and hardness; both, to get better, will need to get hyperbaric oxygenation tx for two to three years to get back to "normality."
I got a second opinion and the second RO just listed me with a full lifetime dosage of 50.40 Gy. The first one wanted to give me 60 Gy (50.4 on regular rads and the remaining in boosts). I considered it to be high. If I get the recurrence, she can irradiate me with the tumor inside. I will keep believing that a cancer cell does not need the same amount of radiation as a well differentiated tumor.
Yes, ROs and MOs need to eat so they will always promote their line of job. Ask your MO about the RO's suggestion of full RT. And ask about lymphedema; it is not mentioned by any oncologist but it is a problem when it flares up and makes one's life miserable. A full dissection, a full rad to armpits, and even a biopsy can provoke a swelling. So ask, ask, ask. And if the MD gets mad then get another who can answer and clarify information.
-
OK. I went to see a second R.O from MD Anderson today and she takes time to explain why she thinks I need radiation. The first R.O didn't tell me these things, but he said I will get 30% benefit from recurrence. After speaking with the second R.O that I see it made sense to me I have lymph vascular invasion. Now for me to decide which Dr. I should use for radiation.
My current Dr..is Kelsey Seybold and the R.O said he does CT scan if my heart is not in the radiation field, no breath hold is needed. The second R.O said I wear a gogle and I can see how far my heart goes when I hold my breath. If I start breathing, the machine will stop. When I relate that to R.O at Kelsey he said that can create an error. What do you all think? Thanks.
-
Thanks for sharing, Houston, I may have LVI, won't know until surgery. I am having bmx next month before rads. I was trying to decide to do chest wall and my first RO did not explain things well either. My second was much clearer and I had a better feeling about her. I have a similar dx to yours. If it has gotten through my lymph node I will be doing chest wall in addition to nodes. Did you already have surgery? How big was your tumor in breast?
-
Hi Jiffrig, I guess each RO has his or her own way of approach. The second RO understood the reason I came to her so therefore she gave me more reasons to do rads. She read the PATH report from my first surgery on 10/5, which said I have LVN but prior to coming to her, I didn't know what that is. She also said I was premenopause at dx and I have greater than 2 cm residual cancer after chemo. If you have at least one positive lymph node at dx then it is no brainer to do rads under armpit. For me I was hesitant about the chest wall until the second RO kinda laid it out. I guess I could escape rads on the chest wall if I have complete PCR to chemo then no residual cancer left. So you may want to see the PATH after surgery and decide further from there. Hope that helps.
-
I want to add that my original tumor was 3.3 cm and the chemo AC+Taxol didn't reduce much, so my tumor after chemo was 2.8. The chemo did cause me to have menopause after AC though. If you have a PCR from chemo then you may not need rads on the chest wall. As your RO said your benefit from rads is 5%. In my case RO said 30%.
-
Houston, in your case you have a greater benefit than the risk involved in the procedure. And if I were you I would stay with the second RO because she seems to be a person who would be careful, considerate, and she is not detached with the patient.
As for the type of procedure, breath holding or not, each RO must be careful as to the measures to avoid radiation to critical organs and tissues. My first RO use the same procedure as your first RO but she doesn't talk. She has the attitude that she has the ultimate truth and one has to follow her silently. The second one use molds in conventional RT to fix me to the table and to avoid movement. She is quite nice but I would feel anxiety to be attached to a table even for 10 minutes. I am claustrophobic and I hate CT and MRIs if they are not open machines. I think she uses X rays to check position in the table but the guy that prepared the list of what-to-do didn't give me the list. Anyway, each type of procedures has its own advantages and disadvantages. Ask to each doctor, if you have the chance, what is the risks of pneumonitis, lung cancer and heart damage using the CT procedure or the breath holding procedure.Both procedures may have the same side effects but not the same probability of developing them.
-
MariangeI43, thank you for your inputs. Like you said, the second RO is a little more thorough, but she said standard surgery the BS has to take out 10 lymph nodes so she's kinda surprised that I had only 2-3 SNL from my PATH report. I went back to talk further with the first RO he's nice to explain to me about the new high tech machine they just had for a year. He showed videos that show a small heart is already out of the radiation field that breath hold is not necessary. He said if the person's heart is enlarged touching the rads field then breath holding would be used case by case. He looked at a CT I did in April and it shows my heart is small within the circumference. So that gives me some peace of mind. However he also let me know the dose of rads I would need is 4860CGY plus 1200 CGY for scar boosts in 27 fractions. I'm no chemist so IDK if that is alot. What is everyone dose of rads given by your RO?. Thanks.
-
Houston, the amount of radiation he is giving to you is a standard 60 grays (60 Gy), divided in 27 fractions (sessions) of 1.8 Gy and the added fractions of the boosts. Since I don't know the # of boosts (usually five) I cannot say how many Gy in boosts. With respect to the lymph nodes, I think that ten are too much. The risk of lymphedema increases with the amount of nodes taken out. Besides, they irradiate the armpit with chest wall; that is also standard procedure.And irradiation also increases lymphedema risk. Do what is best for you. I can't tell you what is the best for you but you know it. We will be here for you.
Dosage will depend on the RO's school, invasion to lymph nodes and to vascular tissues, the stage and degree of the tumor and the aggresiveness of the tumor, and lastly but not less important, the characteristics of the patient. Some people have 50 Gy, other less. AS I said, first RO I saw gave me 60 Gy (28 sessions of 1.8 and the five boosts with remainder Gy). and the other 50.4 Gy (no boosts).
-
Thanks Mariange, the first RO told me it the dosage is 48.6 CGY and 1.2 CGY for boosts. I asked the second RO but she hasn't responded.
OK, here some bad news, I posted earlier that I went to see drs at MD Anderson, well, the RO at Anderson looked at my PATH report (2SNL removed with no tissues left blasted by chemo). She called my OC at Kelsey requested them to having me for surgery for more lymph nodes. The OC said Anderson is the experts so she had to oblige the request. I was furious having just recovered from two surgeries (over 8 weeks now), now they want to open me back up again all because that BS from Kelsey didn't do it right? I'm scheduled to go see him to discuss it.
On the same token, I don't see the need for more lymph nodes taken out if they will be irradiated. Whether they took five or six lymph nodes or 2-3 there's always some possibilities remaining. The only thing is the BS took out 2 sentinel and no axillary. The RO at Anderson told me standard is they take out 10 nodes. Isn't that an overkill? So what are my options now, what can I do if I don't want another surgery? Thank you all.
-
I also want to ask you all if I have remaining positive lymph nodes not taken out. What is the status or possibilities they are spreading?
-
Houston, this is a personal matter between you and the RO. I can only say that I didn't let the BS do the dissection of lymph nodes on me. I am still working and I need my arm in functioning order. I cannot develop lymphedema, and if I have to, it must be a slight one. Since he operated on me I set the limits. The BS is the expert but it was my body and I didn't let him have more than three nodes. I said him NO DISSECTION. I knew and accepted my risk. Anyway, if the BS knows his job and only one node was positive, he doesn't have to cut out the 10 or 20 just because is protocol. Our lives are more important than protocols.
I won't tell you what to do. I will tell you that you investigate what evidence they have to justify the cutting of more and more lymph nodes. If you decide to irradiate, you can decide whether or not you want to let them remove your nodes or not. It is a personal decision that depends on how active you are, your kind of work, if you live alone or not, if you have other family members that will take care of you, etc.
Spreading, I don't know. I need more information. However, neither chemo nor RT can guarantee you that you will not have a recurrence. Some people have recurrence even undergoing both of the treatments. Others don't. There are so many variables. The only thing I can tell you is DON'T PANIC. Relax, ask questions, do you have a friend that can go with you? And if you undergo the surgery, please ask them to send you to a specialist in lymphedema at the slightest swelling. It is difficult to live with that condition.
Can you tell me what was written on you PATH report? Whom did you decide will be your RO, the first or the second? If the second RO obliges you to have a lymph dissection, you don't need to comply. If the first RO do not need the removal of lymph nodes, well, let him do RT. Look what is best for you now and in the near and far future.
I was reading an article that says many ROs and MOs over-treat patients. It is true. They play safe but we pay a high price for it. Take care
 . We are all in the same boat.
. We are all in the same boat. -
Thank you Mariange. I am not opposed to taking lymph nodes, just what is needed. What made me upset was the fact that BS did not take enough to be tested, perhaps, he was in a hurry? I was already lost time energy, had hard time with two surgeries, and now a mistake was done. When I have a talk with BS, I will ask about what's the justification of having more lymph nodes taken out. I'm scheduled to do rads on 12/05. My RO from Kelsey never talked about the PATH, just radiation. When I went to see RO at MD Anderson for second opinion to do rads or not, she reviewed the PATH report and questioned about the lymph nodes removal. She then called my OC at Kelsey, unknown to me, and said I should have more lymph nodes removed. This just happened This past Monday. BTW, I went to MD Anderson a couple of times but never got treatment there. All treatment up to this point was from Kelsey Seybold. What also bothered me was my OC response to me: MD Anderson is the expert so she had to obliged to their request, decision is still ultimately mine. I kept thinking OK so my OC is not confidence in her training, expertise, she didn't tell me what will be my benefits, except go talk to my BS.😓
-
What do you plan to do? I don't think it was an error from BS to remove only two. Do you plan to continue with your OC? What is her specialty? She must have some medical criteria to treat you. Be difficult, question; you, among everybody, are the most interested in your well being.And, NO, you don't have to submit to another surgery just because a second opinion, who is not treating you, just called your OC and asked her to refer you again to BS.
Just in case, Happy Thanksgiving to you and family.
-
Mariange, yes, the decision is ultimately mine. I guess my dilemma was I want to make the right decision, so that it doesn't lead to spreading of the cancer cells. I don't understand the benefits if any, of removing more lymph nodes, whether positive or negative, would that change the course of my treatment? Or am I just gonna still having radiation? I need to talk to the BS this coming Tuesday and I want to ask him if he thinks what he did was optimal in his opinion. If he is satisfied with his performance, then I won't need to go for more surgeries if it is not needed.
Ironically, all the people I talk to, ask opinion, including my family members during thanksgiving, and the ladies on this discussion board. No one has said the BS did anything wrong by removing only two lymph nodes although one of my brothers said there is nothing wrong with wanting to find out if I have positive lymph nodes (having more surgeries) neither. Well, at least that's a good sign, right? Hope you have a Happy Thanksgiving everyone
-
Houston, even though I was not in that dilemma before, I can say the following. 1) Losing more lymph nodes can lead you to an attack on lymphedema in the very near future. (Even the removal of two can rise the statistics on lymphedema on any of us); 2) Your armpit area will be radiated because is standard protocol (whether you have removed two, 10 or 20); also your chest wall and other areas that had stained in the SNB. It will include standard dose and some boosts. That'll result in an additional 40 percent of developing arm and trunk lymphedema. Please, see the photos of persons living with lymphedema. That is not a condition to be taken lightly.
I don't think the BS did wrong when he did the surgery. I think he was thinking what was better for you in the long run. You will be living with the consequences. The action of the second radio oncologist of pushing you into a protocol just for the sake of it was wrong. It has created doubts on you and that is not good. Remember surgeons stain the area and then remove the nodes who absorbed the dye. The ones who see stained nodes are the BSs not the ROs. That RO just wants the nodes out, no matter this will damage your arm, your life, your work, etc. Since it is not happening to him or her, the RO doesn't care. There is a controversy between over-treatment and what is really necessary. If removal of two will do the good, why extract ten or 20?
I believe radiation will do the local cleanse that is expected. That is a regional method of clearing cancer cells from the zone. It is not 100% certain (no method is). Whether we have three, four or five surgeries, two or three complete rounds of chemo, or 20 or 40 fractions of RT, no one can guarantee that we will be cancer free or that we will not have recurrence. The first RO I saw told me the following: "You will followed up during the rest of your life by RT staff because of the long and short side effects of the RT, that can be necrosis, fibrosis, including cancer." I asked the second RO I saw if I were 100% completely cleared of cancer if I accepted the 28 sessions (fractions) of RT. She could not guarantee that either.
In one of the discussion rooms there is a lady who had a recurrence and she complained of having had surgery and a complete round of RT even when she had a very small tumor and the doctor had guaranteed her that she was going to be cancer free after the treatment. Only God knows and time will tell us. So when you go to the BS, ask him or her to tell you in plain English how many nodes were involved and stained in SNB. Ask if he or she thinks that the nodes not staining are a real source of possible cancer in the future and what are of the probability of developing the disease after radiating the area (if you don't remove the lymph nodes). Do not go out from the office with doubts. And if you are still in doubt, ask for an MRI or a PET/Scan; the second is better in detecting cancer activity in other areas of the body. You don't have to undergo surgery if the area is neutral. I think your brother doesn't know the risks of surgery when he makes the comment.
Last thing, cancer cells are resistant to treatment when they are hypoxic, and some or many of them are dormant in our bodies So the better way to assure yourself that you continue cancer free is to change life habits. If you smoke, stop it; if you eat carbon-smoked meats and food, reduce or stop it; eat more vegetables and fruits; do yoga, exercise or walk. And read or see comedies; the best way to heal our body is laughter (especially for long term chronic disorders). There is a book I recommend: Anatomy of an illness. Also what Patch Addams did is unique and real. You will see. Bye, dear, I need to sleep.
-
Hi Mariange, thank you for your thoughtful comments. I agreed no treatment can irradiated all cancer cells. I did speak to the BS he said off all the cases he worked on, mine was one he felt good about, he took only two SNL because those were the only one lit up. BS said he doesn't think another surgery is necessary. So I went on with radiation, things are good so far. The only problem is I'm also taking Amiridex and the SE like joint pain is driving me crazy. I'm staying away from meat, eating lots of fruits and vegetables, herbal supplements to reduce these inflammation. Happy holidays.
-
Houston, Sorry to hear you are already having the joint pain. Keep the changes in eating and you will feel better. I told my MO about it and he said that my arthritis was due to age and not to Arimidex. I looked at him and I didn't believe him, of course. I have two 500 Tylenol pills every day. If not enough, I take two more at night. Since my life without cancer depends on it, I will keep on this small yet deadly pill for as long as I need it. I am also taking anti-oxidants: turmeric for inflammation, Vit C, graviola oil, echinacea and goldeanseal, and last but not least, resveratrol. They are anti-carcinogenic agents and they help me to control the cancer cells that are free-moving.
I am really glad you don't have to undergo a new surgery. The RO was wrong when she wanted to push you into a new surgery. I hope RT continues being fine with you. Let's celebrate when you finish RT.
Bye, see you soon. God bless you and happy holidays.
Maria
-
Mariangel.;I want to update you with my rads. With be, there's always something going on. Well, I'm taking Amiridex which I mentioned give me joint pain on my hands the most, and the back of my left and right arm, when I wake up in the morning I feel like 65 even though I'm 52. Then I started to move around, stretch, put hot towel on back of my neck, it gets better. I'm not a drug person, I like to use home remedy if I can, so I don't take Tylenol. The discomfort is there but it doesn't amount to the pain that needs medication. I will take more herbals, and curcumin for anti-inflammatory once I finish with radiation. RO forbid taking a list of herbs, vitamins, supplement during radiation😞Meanwhile I can take vitamin D and multivitamin.
The twist is I've done four rads so far, the RO has not discussed with me about CT plan. But now the technician is saying they added another step to radiate the middle part of my chest, between the two breasts. They said there are lymph nodes there. Have you heard of this before? Thanks
.
-
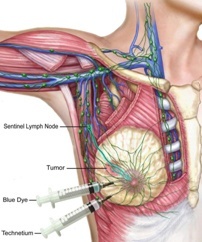
Hi, Houston2016, I hope you are not feeling side effects with RT. If you look after a diagram of the lymphatic system, you will find that around the breast there are several sites with lymph nodes. The intramammary lymph nodes are located near the center between the breasts. In the figure below you see the small white parts (ribs) and running down fine small blue threads. Those are the intramammary lymph nodes. They are irradiated with the chest wall. Since they belong to the lymphatic system and can, in theory, transport cancer cells to other parts of the body, ROs and staff irradiate everything, armpits, supraclavicular, intramammary and chest wall. Since this region is near the heart, they must be quite careful not to damage the heart muscle.
ROs oppose patients using antioxidants because they believe antioxidants interfere with RT. RT produces "healthy" free radicals and antioxidants remove them. If you need further information, you can contact me.
-
Hi Mariangel, it's been awhile I've been struggled with Anastrozole, the generic of Arimidex. Went on other posts and a lady said she switch the name and it has less side effects. So I started yesterday but insurance refused to pay until Jan.8. Meanwhile I still have joints pain on hands, mostly, then back neck tense that now radiated to shoulder and arm, Lower pressure extremity, the RO denied any come from rads. Now, the left underarm pit is fluffy after second week of treatment and RO said that may be seroma and not lymphedema. He said just keep an eye on it but I'm pretty sure it's lymphedema.
-
Houston, Happy New Year 2017. Many health plan go after generics because brand medications are more expensive. They will only cover brand meds if there are no generic equivalents. I used to pay around $60 dollars with Synthroid and now I pay around $12 just because it's a generic. To help you with muscular pains you can have cold or hot pads therapy. Besides, if you are not allergic to aspirin, you can use NSAIDs; they will help a lot. There is also ointments and creams based on arnica (arnica gel or Arniflora, arnicare gel) and menthol (Bengay, mentholatum ointment) that you can use; they are anti-inflammatory meds that are not anti-oxidants. I use them for pain in my hands and feet. I apply it in the area, if in the feet, I use socks to avoid slipping.
What do you mean with lower pressure extremity? As for the fluffy underarm, I think is lymphedema too. Can you locate a physician specialized in perivascular disorders? They are the ones who treat vascular problems in extremities. My orthopedist sent me to one and I still had not had the chance due to so many doctors' appointments. Or ask your MO to send you to one before it worsens. There are accesories to deal with lymphedema of the trunk and of the arm.
I don't think that the RO would admit about the lymphedema. They are worried about not being sued for malpractice so they would say anything to avoid a confrontation. They should be less evasive and more sincere. There is a lot of things they keep silent about and they avoid the topics. Better get a specialist in vascular diseases.
Can I ask you about your CT? How long did it take the RO to take the measures? Did the simulation take more than an hour?
Hoping to hear from you.
Maria







Categories
- All Categories
- 679 Advocacy and Fund-Raising
- 289 Advocacy
- 68 I've Donated to Breastcancer.org in honor of....
- Test
- 322 Walks, Runs and Fundraising Events for Breastcancer.org
- 5.6K Community Connections
- 282 Middle Age 40-60(ish) Years Old With Breast Cancer
- 53 Australians and New Zealanders Affected by Breast Cancer
- 208 Black Women or Men With Breast Cancer
- 684 Canadians Affected by Breast Cancer
- 1.5K Caring for Someone with Breast cancer
- 455 Caring for Someone with Stage IV or Mets
- 260 High Risk of Recurrence or Second Breast Cancer
- 22 International, Non-English Speakers With Breast Cancer
- 16 Latinas/Hispanics With Breast Cancer
- 189 LGBTQA+ With Breast Cancer
- 152 May Their Memory Live On
- 85 Member Matchup & Virtual Support Meetups
- 375 Members by Location
- 291 Older Than 60 Years Old With Breast Cancer
- 177 Singles With Breast Cancer
- 869 Young With Breast Cancer
- 50.4K Connecting With Others Who Have a Similar Diagnosis
- 204 Breast Cancer with Another Diagnosis or Comorbidity
- 4K DCIS (Ductal Carcinoma In Situ)
- 79 DCIS plus HER2-positive Microinvasion
- 529 Genetic Testing
- 2.2K HER2+ (Positive) Breast Cancer
- 1.5K IBC (Inflammatory Breast Cancer)
- 3.4K IDC (Invasive Ductal Carcinoma)
- 1.5K ILC (Invasive Lobular Carcinoma)
- 999 Just Diagnosed With a Recurrence or Metastasis
- 652 LCIS (Lobular Carcinoma In Situ)
- 193 Less Common Types of Breast Cancer
- 252 Male Breast Cancer
- 86 Mixed Type Breast Cancer
- 3.1K Not Diagnosed With a Recurrence or Metastases but Concerned
- 189 Palliative Therapy/Hospice Care
- 488 Second or Third Breast Cancer
- 1.2K Stage I Breast Cancer
- 313 Stage II Breast Cancer
- 3.8K Stage III Breast Cancer
- 2.5K Triple-Negative Breast Cancer
- 13.1K Day-to-Day Matters
- 132 All things COVID-19 or coronavirus
- 87 BCO Free-Cycle: Give or Trade Items Related to Breast Cancer
- 5.9K Clinical Trials, Research News, Podcasts, and Study Results
- 86 Coping with Holidays, Special Days and Anniversaries
- 828 Employment, Insurance, and Other Financial Issues
- 101 Family and Family Planning Matters
- Family Issues for Those Who Have Breast Cancer
- 26 Furry friends
- 1.8K Humor and Games
- 1.6K Mental Health: Because Cancer Doesn't Just Affect Your Breasts
- 706 Recipe Swap for Healthy Living
- 704 Recommend Your Resources
- 171 Sex & Relationship Matters
- 9 The Political Corner
- 874 Working on Your Fitness
- 4.5K Moving On & Finding Inspiration After Breast Cancer
- 394 Bonded by Breast Cancer
- 3.1K Life After Breast Cancer
- 806 Prayers and Spiritual Support
- 285 Who or What Inspires You?
- 28.7K Not Diagnosed But Concerned
- 1K Benign Breast Conditions
- 2.3K High Risk for Breast Cancer
- 18K Not Diagnosed But Worried
- 7.4K Waiting for Test Results
- 603 Site News and Announcements
- 560 Comments, Suggestions, Feature Requests
- 39 Mod Announcements, Breastcancer.org News, Blog Entries, Podcasts
- 4 Survey, Interview and Participant Requests: Need your Help!
- 61.9K Tests, Treatments & Side Effects
- 586 Alternative Medicine
- 255 Bone Health and Bone Loss
- 11.4K Breast Reconstruction
- 7.9K Chemotherapy - Before, During, and After
- 2.7K Complementary and Holistic Medicine and Treatment
- 775 Diagnosed and Waiting for Test Results
- 7.8K Hormonal Therapy - Before, During, and After
- 50 Immunotherapy - Before, During, and After
- 7.4K Just Diagnosed
- 1.4K Living Without Reconstruction After a Mastectomy
- 5.2K Lymphedema
- 3.6K Managing Side Effects of Breast Cancer and Its Treatment
- 591 Pain
- 3.9K Radiation Therapy - Before, During, and After
- 8.4K Surgery - Before, During, and After
- 109 Welcome to Breastcancer.org
- 98 Acknowledging and honoring our Community
- 11 Info & Resources for New Patients & Members From the Team