Breaking Research News from sources other than Breastcancer.org

I watch for research news on breast cancer, treatments, etc., and frequently see interesting articles. There is a topic on BCO called "Breaking Research News from Breastcancer.org." One of the moderators suggested that another topic might be appropriate for posting links and synopses of reports on research found elsewhere. So here it is! Please post links to reports on research form reliable sources. Thanks for sharing!
Comments
-
Elucent Medical Receives FDA Clearance for Innovation for Breast Tumor Removal Procedures
EnVisio Surgical Navigation System and SmartClip Soft Tissue Marker provide alternative for painful and costly localization procedures
Elucent Medical announced that it has received U.S. Food and Drug Administration (FDA) 510(k) clearance for the clinical use of the company's EnVisio™ Surgical Navigation System. Elucent Medical's permanently implantable wireless SmartClip™ Soft Tissue Marker provides an alternative localization procedure. The SmartClip™ is used by surgeons with the company's EnVisio™ Navigation System to identify the location of the malignancy and to wirelessly navigate to it in real-time 3-D. The system can uniquely identify three different SmartClip™ Soft Tissue Markers – allowing physicians to effectively mark difficult lesions and navigate distances, depths, and directions... Elucent Medical is offering a ...solution that addresses a key challenge for breast surgeons: how to easily find the location of a malignant biopsy during surgery, especially in tissue that lacks anatomical landmarks.
-
Lumpie- I heard a talk with a panel of MOs who said that they can't get authorization for the genetic testing for many patients especially if they are under 60 years old. The prices have come way down so maybe if the insurance refuses- patients could pay for it themselves.
-
Nkb, my genetic testing was billed at about $4500 from the lab (independent of my hospital) and about $300 from my hospital for the counselor and the blood draw. I don't know how much it is other places, but it would be a stretch to cover that by myself.
-
mountain Mia- that sounds like the prices for when I had the tests also- tho my insurance covered it- these MOs are saying that it is getting closer to $250-750 for the 11 or 13 tests that are the most important. Hope it is true.
-
Effect of Radiotherapy After Breast-Conserving Surgery Depending on the Presence of TILs
- The purpose of this study was to analyze the association of tumor-infiltrating lymphocytes (TILs) with the effect of postoperative radiotherapy (RT) on ipsilateral breast tumor recurrence (IBTR) in a large randomized trial of 936 patients with stage I/II breast cancer. The authors found that high TIL values were associated with a reduced risk of IBTR (HR, 0.61; P=.033). The interaction between RT and TILs was not found to be statistically significant (P=.317).
- High TIL values within the primary tumor may be associated with a reduced risk for IBTR. The authors further conclude that patients with low TIL values may experience a greater benefit from RT with regard to reduced risk of IBTR.
DOI: 10.1200/JCO.18.02157 Journal of Clinical OncologyPublished online April 02, 2019. -
My insurer would not pay for genetic testing either. We found a lab that would do it for around $400 "cash" paid by me/the patient without doing the insurer's paperwork. Some labs offer "patient assistance programs" for those who either do not have insurance or whose insurance will not cover the testing. It is worthwhile to ask. Sometimes these programs depend on your household income. You will still have to have an order from your physician and you they may want you to agree ahead of time that you will pay a fixed price and that they will not file insurance paperwork. It is interesting that they seem to be discussing this testing as "standard of care" but that insurers are not paying for it. Unfortunately, it seems like it often takes a while before the insurers catch up to actually paying for standard of care.
-
What genetic testing are you referring too, like BRACA and other mutations or something more specific?
-
illimae, Basically, yes. There are a lot of labs that offer testing. And your physician will recommend the testing that seems most appropriate. Some labs offer a breast cancer specific panel that screens for risk for hereditary breast cancer risk only. A lab may also offer a multi-cancer panel that screens for elevated risk for multiple types of cancer. BRCA genes would almost certainly be included in either of those but it's always wise to double check. Of course, our knowledge of genetics and causality continues to evolve, so these tests may change over time as researchers learn more. As that knowledge evolves, you may be able to get updated results or you may need to be retested. Keeping in mind that this is just one lab/just one example, if you want to read up on the tests available by looking at a lab's website, here are a couple of links to a lab I know some practitioners to use:
Breast cancer panel {interestingly, this indicates that it is for ER+, HER2− early-stage breast cancer patients only}
https://myriad.com/products-services/breast-cancer/endopredict/
Multiple hereditary cancers:
https://myriad.com/products-services/hereditary-cancers/myrisk-hereditary-cancer/
Some of the web pages have videos. It can actually be quite educational if you are interested in genetics.
-
Thanks for clarifying. I was tested almost immediately at MDA since I was stage IV de novo at 41 with strong family history (mom and maternal aunt). Results were negative but the genetic counselor believed there’s something in a combination of genes not currently known. It was covered by my insurance since I was under 45, I only paid the $100 copay. Interesting stuff, thanks!
-
On the TRAIL of a Solution to Trastuzumab Resistance in HER2+ Breast Cancer
A genomic and proteomic analysis of HER2-positive breast cancer cell lines that are resistant to trastuzumab found a deregulation of the cell death pathway known as TRAIL (tumor necrosis factor–related apoptosis-inducing ligand). The finding presents the possibility of targeting this pathway as a way to lessen the impact of trastuzumab resistance in HER2-positive breast cancer.
https://www.sciencedirect.com/science/article/pii/S0304383519301983
-
Organ Transplant Disability Bias Gets Second Look Under Trump
The Office for Civil Rights (OCR) in the U.S. Department of Health and Human Services (HHS) is reportedly considering written guidance warning health care providers that denying organ transplants based solely on disability violates the ADA.
{This would seem to raise some interesting questions about the possibility of transplant for oligo-metastatic disease.}
-
as I recall, my genetic tests covered about 15 variables. Even with a strong family history (mom and both her sisters, who each had recurrences), the tests did not find any links. My insurer- Aetna- covered the tests. I think the hospital told me they will check results again in 5 years if new tests are available.
I find it unconscionable that some insurers won’t cover genetic testing and/or that the standard of care depends on where you live.
Lanne
-
When I was diagnosed in 2012 I was tested for BRAC through Myriad which was negative. At the time, insurance didn't cover it so I paid $4000 for the testing. Took me forever to pay it off!! Well, now I've just gotten my mammogram results letter (all good!) and the letter says genetic testing is now strongly recommended for anyone having had BC. I called the breast center where I had my testing done because I wasn't sure if my original testing was all that was needed or if there was more. The counselor there said Myriad is now offering additional testing to anyone who only had BRAC done. It covers about 30 more genes that are looked at for other ties to BC and insurance should cover it. Apparently guidelines recommend the latest testing be done for all BC patients. So I've called my BS and they are supposed to be sending a referral to the breast center so I can go in for a blood draw to get the extra tests done.
-
lala1, I am really impressed that you received a letter saying that testing is recommended. I would venture to say that most of us do not get such proactive notification. That is great that Myriad is offering additional testing. (I hope it is at a palatable-to-patient fee structure.) Sounds like most of us probably need to check in with our docs to be sure that we have had suitable testing. There is so much more to learn in the field of genetics. I venture to guess that this is something we each probably need to revisit with our providers every 5 years or so if we want to keep up with the latest findings. I sort of feel like that is something I can do for my family... to give them a heads up if there is a chance of increased risk. Right now, only about 10% of breast cancer can be associated with inherited risk.... which leaves so many of us wondering what the heck happened!
-
Lumpie, what does Myriad test for? Is it similar to Oncotype? Thank you!
-
lala1, the insurance should reimburse you the 4k!
-
April1964: Oncotype and similar tests (like MammaPrint) test the genetics of a tumor. This is sometimes also referred to as "genomics." Myriad tests the genetics of your body/your person. You may also hear the term "germ line" in reference to genetics. That means things that are hereditary... which can be passed along within a genetically related family (parent to child). One of the best genetics references if you want to read more about genetics is the Genetics Home Reference. It is part of the NIH U.S. National Library of Medicine. Professionals use it, too! They used to have a really excellent glossary of terms which, lamentably, I can no longer find, but there is still lots of good descriptive/educational info. Here's the link:
-
thank you so much Lumpie!!!!
-
I initially had genetic testing for 6 variants which were all negative. Once my mom had BC for the second time, they did full panel on her and found VUS in CHEK2. They tested me for that same thing, but only that and found I had it too. I could not get full panel testing done "since I already had BMX, it would not alter my treatment". I had full panel testing done by COLOR Genomics for $250. It found the same VUS, but thankfully nothing more. It was very efficient and easy.
-
Need advice from you wise woman or anyone reading this post with knowledge and experience. I found out this week I have a positive mutation for ATM. It's very rare and only 1% of the population are carriers. It's considered a moderate risk for BC however in general it's about 50%. risk for recurrence. I received very little information from my genetic counselor and will be meeting with the Genetic Oncologist next week. I have lots of questions to ask her.
In the meantime my BS office called yesterday to schedule an MRI. My PA asked if it was too soon to discuss surgery. I said I would meet with the BS next week after my appointment with the Genetic Oncologist. I suspect the BS is going to recommend a BMX or increased surveillance. The thing is with this mutation, radiation may be a problem though everything I read said these findings are not conclusive. I've already had a lumpectomy and radiation on my left breast. So just add that to my stress level as well as the implications for my daughter
So these are my questions.
1. Does the location of the mutation on the gene determine the percentage of your risk factor?
2. How would I get a second opinion re surgery options from another BS?
3. Should I also schedule an appointment with my MO?
As you can relate, I'm a nervous wreck. I'm anxious and oh by the way I am claustrophobic although with an anti anxiety medicine I can tolerate the breast MRI because it's face down. I'm not sleeping. I have to make peace with the decision to move forward with the BMX. I know reconstruction is not an option for me. I don't want implants and the radiated breast would be a problem,
Any words of wisdom would be helpful. I know that I'm fortunate that at this moment my cancer has been contained and I offer a prayer of gratitude for that and all the positive things in my life. I think once I have a plan things will settle down and I won't be as overwhelmed.
-
Lumpie--I just received notice from my insurance that my testing has been approved. My BS has sent a referral to the breast center and I'm just waiting for them to call to get an appointment. I do plan to confirm what, if anything, I will need to pay.
And Laughing Gull, the insurance won't reimburse me since it was 6 years ago and I was with a different insurance company. At the time, many insurance companies didn't cover this.
-
Low-Dose Tamoxifen to Prevent Local and Contralateral Recurrence in Breast Intraepithelial Neoplasia
Tamoxifen administered for 5 years at 20 mg/d is effective in breast cancer treatment and prevention, but toxicity has limited its broad use. Biomarker trials showed that 5 mg/d is not inferior to 20 mg/d in decreasing breast cancer proliferation. We hypothesized that a lower dose given for a shorter period could be as effective in preventing recurrence from breast intraepithelial neoplasia but have a lower toxicity than the standard dose.
We conducted a multicenter randomized trial of tamoxifen, 5 mg/d or placebo administered for 3 years after surgery in women with hormone-sensitive or unknown breast intraepithelial neoplasia, including atypical ductal hyperplasia and lobular or ductal carcinoma in situ. The primary end point was the incidence of invasive breast cancer or ductal carcinoma in situ.
Tamoxifen at 5 mg/d for 3 years can halve the recurrence of breast intraepithelial neoplasia with a limited toxicity, which provides a new treatment option in these disorders.
https://www.practiceupdate.com/C/82315/56?elsca1=emc_enews_topic-alert
https://ascopubs.org/doi/full/10.1200/JCO.18.01779
DOI: 10.1200/JCO.18.01779 Journal of Clinical Oncology
-
I suspect that's probably the case with a lot of drugs. Why they have to drag us through the mud first I will never understand.
-
Butterfly1234:
So sorry that this is a distressing time - but we understand!
You have a Genetic Oncologist? Interesting! I have not run across one of those. That sounds good because a Genetic Oncologist should be able to counsel you on both the implications of the genetic findings and the relative risks and benefits of available therapies including radiation. Genetic counselors are great. but their expertise is often limited to the implications of the genetics. Their knowledge about medical interventions and how those mesh with your genetic risk profile may or may not be extensive. If your situation is unique, that just adds complexity.
Mutations are generally categorized as creating increased risk, of unknown significance or not associated with increased risk. (Sort of small-medium-large buckets.) Your GO (or genetic counselor) should be able to counsel you on the risk associated with a particular mutation.
As far as a second opinion, first, you will need to identify where you want to get that second opinion. People often go to a major cancer center for a second opinion. You might pick one not too far away from where you live. Often their websites will tell you how to get in touch about getting a second opinion. Otherwise you can call. They will need a copy of your medical records. Some will provide a second opinion based on your records only. Some will want you to come for a visit. You may have a preference as far as which would better suit your needs. If you do not want to go to a major medical center, you can see another oncologist near you. Many of us think it is valuable to be sure that this opinion is independent so we go to an oncologist that is not in the same practice as the physician we saw originally. Whichever option you choose, you should check with your insurance about coverage for the second opinion. {My personal input: if what you are hearing just doesn't sound right to you, consider talking with another doctor. Sometimes docs are make mistakes and many of us have had to visit multiple docs to address our concerns.}
You definitely want to keep your MO in the picture. Do you have a sense of the extent to which your docs work as a team routinely - vs being a team built ad hoc for your care? If your docs work together routinely, they are probably good at working together. If not, it may take a little more effort to be sure everyone is working off the same game plan. I would suggest being sure your MO knows what you are working on (i.e.: going to the GO), what the time line is (when you are going), and be sure s/he gets the report from your visit and has access to copies of all test results. In an ideal world, your care team would be sharing these documents and records via an electronic health records system but that does not always happen. Let your MO know if you are getting a second opinion, too. After you have completed these tasks, you will have more complete information and that is probably when your MO will want to sit down with you and finalize a plan for care. This sort of assumes that the MO is the "point person" for your oncology care. That is most often the case but not always so it is helpful to verify that with all involved.
I hope that this puts some structure around things that may be helpful. I think that most of us would agree that you are in the toughest phase - trying to gather information, make sense of a great deal of information and make a plan. A lot of us feel like once we have a plan and can focus on executing the plan, we feel much more like empowered agents of our own well-being.
[Gratuitous tips: sometimes I tell myself to turn into Mr. Spock from Star Trek and only think about things logically. Similar but slightly different: if it all feels like too much, try to mentally think that it is happening to someone else and how would you guide her through it. For me, I have to put structure around what;s happening and look at the facts. Incorporate how you feel about things but if you know that you are informed and methodical, this may help you feel more comfortable about your actions and decisions .]
This post strays from research news and we may need to move it to a different forum but I wanted to provide Butterfly with a response. All the best, Butterfly1234! I have found helpful counsel at BC.org and hope you will, too!
-
Regarding genetic testing: Color Genomics (https://www.color.com/learn/color-genes#cancer) is a highly reputable company offering a variety of genetic testing services. Their hereditary cancer test panel is $249. This includes the opportunity to speak by phone with a genetic counselor to discuss your results. If you are found to have an issue of concern, family members may opt to be tested for about $25.00. Your MD's referral is not required although I think they provide the opportunity to consult with one on their staff prior to testing (this could have changed).
I'm not shilling for Color but I think it's important that women know their options. I don't consider companies such as 23 and Me to be a good choice - their data privacy policy isn't sufficient and they don't test for more than a few mutations on the BRCA 1/2 genes much less test for more recently identified problems in other genes.
Mary Clare King (google her) is affiliated with Color, which says a lot about the company. (I think they may also help support BCO).
If I hadn't already been through the genetic testing wrangle with my insurer, I'd go to Color. As it is, my sister did use Color when her PCP and OB/GYN dragged their feet (despite my genetic counselor's strong recommendation). She found it easy, very helpful and a lot faster than going through any more hoops.
I also believe it's vital to thoroughly understand all the implications of seeing genetic testing. Regardless of results it can impact your ability to obtain life insurance and the price you pay for it. Should GINA protections be removed or weakened it could be a problem. So do your homework first.
-
I don’t want to get off topic on this thread so I’ll quickly respond to Lumpie. I respect and thank you for your insights and wisdom. I’ve read every word and appreciate the time you took for your thoughtful response. You help me gain some levity in my decision making process. Just in case anyone is wondering the Genetic Oncologist is part of the genetic testing process at my treatment center. She will be reviewing my test results with me.
Blessings all
-
MSH6 and PMS2 germ-line pathogenic variants implicated in Lynch syndrome are associated with breast cancer
Genetics in Medicinevolume 20, pages1167–1174 (2018)
There is a BCO page that references this article. But having read the recent discussion of testing on this thread, what I want y'all to know is that despite the growing evidence, not all oncologists or genetic testing companies consider these genes as “breast cancer genes" yet. (They are particularly associated with colon and endometrial cancers, but there is a long list.) Myriad's chart on their web site is missing a dot in the breast cancer column for these genes. Yet I saw a chart in a paper that showed a 30% lifetime breast cancer risk for MSH6. So bc patients who have Lynch cancers in their family history may want to specifically inquire about a panel that includes these genes. A “breast cancer panel" may not yet include it.
-
Thanks, ShetlandPony. The genetic counselor I worked with also thought Lynch Syndrome was significant for breast cancer.
-
Locoregional Surgical Treatment Improves the Prognosis in Primary Metastatic Breast Cancer
TAKE-HOME MESSAGE
- In this population-based retrospective study of patients with primary metastatic breast cancer, those who underwent surgery exhibited breast cancer–specific survival and overall survival almost double that seen in patients who did not undergo surgery. A survival advantage was reported for patients with single metastases to the bone, liver, or lung. A significant survival advantage was reported when surgery was combined with radiotherapy and/or chemotherapy, regardless of molecular subtype and tumor size. Overall, surgery led to a 40% reduced mortality risk.
- These findings support the consideration of locoregional breast surgery in patients with primary metastatic breast cancer.
- Written byLillie D Shockney RN, BS, MAS
Patients with stage IV breast cancer chronically and repeatedly ask about having breast cancer surgery to rid their body of the source of this disease. The analogy of a dandelion going to seed is used to describe how the cancer — the dandelion — has gone to seed and the seeds — the metastases —have landed elsewhere in the yard. So, patients naturally ask, "Why wouldn't the original dandelion that caused this to happen be dug up too? Why just treat the seeds that blew away?"
This study provides information demonstrating that there may be benefit in treating the primary breast cancer with surgery to remove the source of the disease. Hopefully, the cancer will have only spread to one organ, such as the most common metastatic site—the bone.
There is also a potential psychological benefit to having the surgery done. The cancer is in the breast — right under a patient's face. Some women have been requesting lumpectomy or mastectomy surgery not because they think it will clinically help them, but because they don't need the reminder constantly that they have cancer lying within their chest.
Abstract
This abstract is available on the publisher's site.
BACKGROUND
We aimed to validate the clinical significance of locoregional surgery in improving the prognosis of primary metastatic breast cancer (pMBC).
METHODS
We conducted a population-based retrospective study by analyzing clinical data obtained from the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) database. Stratification analysis was employed to assess the effect of breast surgery on breast cancer-specific survival and overall survival. Then propensity score matching and COX regression models were employed to evaluate the survival advantages of breast surgery, if any in patients with pMBC.
RESULTS
The median BCSS and OS in the surgery group were almost twice of that in the group without surgery. Breast surgery provided a survival advantage for patients with a single metastasis in the bone, liver or lung, but not in the brain. We found that axillary lymph node dissection performed in combination with specific breast surgical procedures did not result in a significant improvement in survival. Additionally, when combined with radiotherapy and/or chemotherapy, surgery significantly improved the survival and was not influenced by the molecular subtype and tumor size. Finally, using COX regression models before and after propensity score matching, breast surgery was found to reduce the risk of mortality in patients with MBC by more than 40%.
CONCLUSIONS
The effect of locoregional surgery has been underestimated in pMBC patients. Surgical procedures should be seriously considered when planning combination treatments for pMBC patients with a single metastasis except for brain metastasis.
-
Hopeful, is there a website that publicly posted this study? I’m having this conversation with my oncologist and he is firmly against surgery. Thank you.
-
Hopeful I saw this study somewhere. I'm glad this question is resolved for our MBC friends. But I feel bad for the ones that didn't get the surgery.
Here's the website wanderingneedle. You will need to sign up but it's free. I hope your doctor agrees!
http://www.practiceupdate.com/content/locoregional... -
Wanderingneedle, put this in google for the original publication (the insert link function isn't cooperating today):
Locoregional Surgical Treatment Improves the Prognosis in Primary Metastatic Breast Cancer Patients With a Single Distant Metastasis Except for Brain Metastasis
Breast 2019 Jun 01;45(xx)104-112, X Li, R Huang, L Ma, S Liu, X Zong
I hope this helps you in your discussions with your oncologist.
Marijen, yes, I feel badly for those who missed out, also. That's one of the many very frustrating aspects of cancer - we all know that treatments and knowledge will be so much improved in the near future but most of the time we won't be in a position to benefit from it.
-
{This is an opinion piece on Medicare Part D vs scientific research but some may be interested...}
Medicare Part D must evolve to help people fight cancer
In recent years, there have been incredible advancements in cancer treatments. But these innovations are only valuable if patients have access to them and Medicare Part D has remained relatively unchanged in the last 13 years.
This article explores what the gaps are and what can be done to fix them. -
FDA Pipeline: Designations for Myelodysplastic Syndromes, Triple-Negative Breast Cancer, AML, and EBV-Associated Cancers
Fast Track Designation for INT230-6 in Relapsed or Metastatic Triple-Negative Breast Cancer
The FDA granted Fast Track designation to a development program evaluating INT230-6 for the treatment of patients with relapsed or metastatic triple-negative breast cancer who have failed at least two prior lines of therapy. INT230-6, designed for direct intratumoral injection, comprises two proven, potent anticancer agents and a penetration enhancer molecule that helps disperse the drugs throughout tumors and diffuse into cancer cells.
INT230-6 is being evaluated in a phase I/II clinical study in patients with various advanced solid tumors. In preclinical studies, INT230-6 eradicated tumors by a combination of direct tumor kill and recruitment of dendritic cells to the tumor microenvironment that induced anticancer T-cell activation.
-
Wonderingneedle - May I ask what your oncologist reason is for strongly rejects surgery of the metastatic site?
-
AMP, he says it’s already spread and there is no medical benefit. On my last appointment I asked again and he just kind of chuckled and said sure if you really want to I’ll stop your treatment and you can have it done. I would like his support and not feeling like maybe he won’t pay as much attention if I’m not doing what he says. I would really like a second opinion from a surgeon who is familiar with the research and who has worked with metastatic patients at a cancer center. The surgeon I went to when I was diagnosed only deals with early stage and she’s kind of brutal. My oncologist doesn’t care for her so it adds to the problem. I go to a private community clinic, not a comprehensive canter center so I don’t think they’re on top of everything. I get frustrated when I read these articles and the treatments seem so unreachable
-
Can you go outside the clinic you currently go to?
-
Sara, I had a second opinion in January when my treatment was changing and they mentioned surgery but because I wasn’t looking for surgery then I didn’t pursue it. I’m on my fourth line since I started in January last year and I’m frustrated that my original tumor will respond to treatment then quickly start growing again.
-
Surgery Tied to Improved Survival in Stage IV Breast Cancer
Women with human epidermal receptor 2–positive (HER2+) stage IV breast cancer who received surgery after systemic therapy were at a 44% reduced relative risk for death compared with women who did not undergo surgery. The finding comes from a retrospective analysis reported on April 3 at the American Association for Cancer Research (AACR) 2019.
https://www.abstractsonline.com/pp8/#!/6812/presentation/6349
{Even though it relates to HER2+ only, this seems timely, given the discussion. I thought the evidence in favor of surgery was fairly clear at this point. The abstract and article are about an Apr 3, 2019 presentation. I know that there have been links to other articles on this topic posted. I wish there were a better way of indexing those links. If I locate others soon, I will post them.}
-
Associations Between Dietary Patterns and the Risk of Breast Cancer
Background: Epidemiologic evidence suggests that certain dietary patterns were associated with breast cancer risk, but the results have been inconclusive. We assessed the associations between different dietary patterns and the risk of breast cancer by conducting a meta-analysis of observational studies.
...sub-group analyses showed that the positive association between a Western dietary pattern and breast cancer risk was significant among postmenopausal, but not premenopausal women, and significant for hormone receptor-positive tumors, but not receptor-negative tumors. In contrast, the inverse association between a prudent dietary pattern and breast cancer was significant in premenopausal, but not postmenopausal women, and significant for both hormone receptor-positive and receptor-negative tumors.
Conclusions: The results of the current meta-analysis suggest a possible increased risk of breast cancer associated with a Western dietary pattern and a reduced risk with a prudent dietary pattern. Large-scale cohort studies with a high quality need to be conducted to further confirm the findings of the current meta-analysis. As dietary patterns are modifiable, these findings may provide viable strategies for breast cancer prevention through changes in dietary intake.
https://www.medscape.com/viewarticle/910479_1
Breast Cancer Res. 2019;21(16)
-
Lumpie I'm running into a firewall.
-
You may have to register but it should be free.
-
Got it--thanks.
-
wanderingneedle
My new MO is “on board" for removing surgically and is part of my treatment plan.
I had a small town MO who was unsure of the next step and referred me to a teaching hospital. He also was against surgery. I move my care to Oregon Science Health University.
So much more to offer the patient, up on all new treatments.
Are you next To any cancer treatment centers? You should reach out to one - if only for a second opinion .
AMP47
-
Photos and resources from the Living Beyond Breast Cancer 2019 Conference on Metastatic Breast Cancer: Thriving Together held in Philadelphia, PA April 5-7 are now available online. Most presentations from the confernece are available in video or audio format.
-
Brilliant, thank you so much Lumpie
-
HER2-Amplified Breast Cancer and Circulating Tumor DNA
- This translational substudy of the NeoALTTO trial was designed to evaluate the prognostic impact of circulating tumor DNA (ctDNA) among patients undergoing HER2-targeted therapy in the neoadjuvant setting. Detection of ctDNA before neoadjuvant therapy was associated with lower pathologic complete response rates.
- Patients with HER2-enriched tumors and undetectable ctDNA at baseline may be the best candidates for treatment de-escalation, owing to their high pathologic complete response rates.
Published Online April 25, 2019DOI: 10.1158/1078-0432.CCR-18-2521 -
I can't post links, but there is an article recently published in medicalnewstoday about a study investigating a new potential approach for containing the spread of metastatic breast cancer. Link to the study is in the article if you find it.
Is it better to 'contain' rather than destroy cancer?
In the new study — the findings of which appear in the journal Cancer Research — the investigators used an existing drug to stop metastatic breast cancer cells from giving rise to new tumors by keeping them in a sleep-like state...
The researchers zeroed in on the drug fostamatinib, which is currently approved for the treatment of immune thrombocytopenia, an autoimmune disease characterized by a low platelet count in the blood...
The team explains that their research in mice has shown that fostamatinib is also able to contain metastatic cancer cells and stop them from developing into full tumors, causing further damage...
Working with mouse models of breast cancer, the researchers found that, when they treated metastatic cancer cells with this drug, those cells remained contained and did not give rise to new tumors...
"But you can imagine that [setting up] clinical trials for this kind of thing is going to be very difficult because, technically, the patients are in remission and disease-free," he adds.
-
This is new for Professionals
Welcome to the OncLive® CommunityThe OncLive® Community comprises community, academic, and clinical oncologists throughout the world. Nurse practitioners, physician assistants, case managers, and all allied health professionals also contribute to this unique, diverse community of professionals working in the field of oncology. Together, this community has immense power to improve today's cancer care. This platform is a forum where everyone can communicate and collaborate in real time to provide solutions to current challenges.
-
Sharing this post from Best Bird's website:
Trastuzumab Deruxtecan (DS-8201) is a novel drug consisting of a HER2 antibody attached to a "topoisomerase I inhibitor" (a new class of anticancer agents that interrupt DNA replication in cancer cells).
The recent Phase 2 DESTINY BreastO1 clinical trial studied trastuzumab deruxtecan in 115 patients with unresectable and/or metastatic cancer who had previously received a median 7 lines of therapy including Herceptin and Kadcyla (as well as Perjeta in most cases). The patients in the study had either: HER2-positive breast cancer, HER2–low expressing breast cancer (considered HER2 negative), HER2-positive gastric cancer, or various other HER2-expressing solid tumors. Data revealed that the overall response rate with trastuzumab deruxtecan was 59.5% and the disease control rate was an impressive 93.7%. The median duration of response was 20.7 months, the median progression-free survival was 22.1 months, and the median overall survival has not yet been reached. From: https://www.targetedonc.com/news/fam-trastuzumab-deruxtecan-demonstrates-encouraging-responses-in-advanced-her2-breast-cancer As of May 2019, there are three recruiting clinical trials of trastuzumab deruxtecan for MBC patients.
You can find Best Bird's web site at www.insidersguidembc.com. It is an excellent resource. Her ebook is available in multiple formats for a small charge, in PDF format free of charge. It is also available in print form.
-
Mammo-Based Deep Learning Model Assesses Breast Cancer Risk
Deep learning models more accurate than models that use traditional risk factors, breast density
THURSDAY, May 9, 2019 (HealthDay News) -- Mammography-based deep learning (DL) breast cancer risk models are more accurate than models that consider traditional risk factors and breast density, according to a study published online May 7 in Radiology.
Adam Yala, from Massachusetts Institute of Technology in Cambridge, and colleagues conducted a retrospective study involving 39,751 women with 88,994 consecutive screening mammograms to develop a mammography-based DL breast cancer risk model. For each patient, all examinations were assigned to training (71,689 examinations), validation (8,554 examinations), or test set (8,751 examinations). Three models were developed to assess breast cancer risk within five years: a risk factor-based logistic regression model (RF-LR) that included traditional risk factors, a DL model (image-only DL) that used mammograms alone, and a hybrid model combining traditional risk factors and mammograms.
The researchers included 3,937 women in the test set. The areas under the receiver operating characteristics curve (AUCs) were 0.70 and 0.68 for the hybrid DL and image-only DL, respectively. The AUCs for RF-LR and a comparison model that included breast density (Tyrer-Cuzick [TC] model) were 0.67 and 0.62, respectively. Compared with the TC and RF-LR models, the AUC for hybrid DL was significantly higher.
"These results support the hypothesis that mammography contains informative indicators of risk not captured by traditional risk factors, and DL models can deduce these patterns from the data," the authors write. "These models have the potential to replace conventional risk prediction models."
Massachusetts Institute of Technology and Massachusetts General Hospital have filed patents on the deep learning models.
https://www.practiceupdate.com/C/83470/56?elsca1=emc_enews_topic-alert
-
The Impact of Chest Wall Boost on Reconstruction Complications and Local Control in Patients Treated for Breast Cancer
- International Journal of Radiation Oncology*Biology*Physics The authors of this study performed a retrospective chart review of 746 breast cancer patients to evaluate whether delivery of a chest wall boost (CWB) to the mastectomy scar/chest wall is independently associated with reconstruction complications. Upon multivariate analysis, the authors found that CWB was significantly associated with infection, skin necrosis, and implant exposure. Among patients receiving implant reconstruction, CWB was independently associated with increased risk of implant failure.Based on these findings, the study authors conclude that omission of CWB in post-mastectomy radiation may improve breast reconstruction outcomes without a deleterious effect on local tumor control.
-
Resistance Mechanisms to Anti-HER2 Therapies in HER2-Positive Breast Cancer
- Critical Reviews in Oncology / Hematology The authors of this review highlight current knowledge regarding the mechanisms involved in the development of anti-HER2 therapy resistance in HER2-positive breast cancer.The authors provide detail on mechanisms such as impaired drug binding to HER2, constitutive and self-sufficient signaling in HER-related signaling pathways, metabolic reprograming, and attenuation of the immune system activation state.
Abstract:HER2-positive breast cancer (HER2 + BC) represents 15–20% of all BCs. In the last two decades, the introduction of monoclonal antibodies (MoAbs), tyrosine kinase inhibitors (TKIs) and antibody-drug conjugates (ADCs) directed against HER2 impressively improved patient prognosis in all disease stages.Yet, not all patients with limited-stage disease are cured, and HER2+ metastatic BC (mBC) remains an almost invariably deadly disease. Primary or acquired resistance to anti-HER2 therapies is responsible for most treatment failures. In recent years, several resistance mechanisms have been identified, such as impaired drug binding to HER2, constitutive activation of signaling pathways parallel or downstream of HER2, metabolic reprogramming or reduced immune system activation. However, only a few of them have been validated in clinical series; moreover, in the era of standard-of-care dual HER2 blockade, these mechanisms should be re-assessed and, in case, confirmed with anti-HER2 combinations.Defining the best strategies to delay or revert resistance to anti-HER2 treatments will be crucial to improve their clinical efficacy.https://www.practiceupdate.com/C/83253/56?elsca1=emc_enews_topic-alerthttps://www.sciencedirect.com/science/article/pii/S1040842818304463https://doi.org/10.1016/j.critrevonc.2019.05.001{At present, there is a charge for access tot he full article unless you have access to a research library.} -
Less Invasive Mastectomy an Option for More Patients
Higher-risk patients may now be eligible for nipple-sparing mastectomy
WEDNESDAY, May 8, 2019 (HealthDay News) -- Complication rates for nipple-sparing mastectomy (NSM) are decreasing despite expanded indications for the procedure among higher-risk patients, according to a study presented at the annual meeting of the American Society of Breast Surgeons, held from April 30 to May 5 in Dallas.
Whitney Young, M.D., from the Mayo Clinic in Rochester, Minnesota, and colleagues examined complication and reconstruction success rates among patients treated in 2009 to 2017 with NSM identified from an institutional, prospective breast surgery registry. Analysis included 1,301 breasts in 769 women undergoing NSM for cancer or risk reduction (median age, 48 years).
The researchers found that the overall 30-day complication rate was 7.5 percent but declined from 14.8 percent in 2009 to 6.3 percent in 2017. During the same time period, the proportion of patients with obesity and treated with neoadjuvant chemotherapy increased. There was a significant increase in 30-day complication rates among patients with prior radiation (odds ratio, 2.3) and recent/current smoking (odds ratio, 3.3). At one year, reconstruction success was 98.5 percent. One-year reconstruction failure was significantly associated with previous radiation (odds ratio, 4.6) and postoperative adjuvant radiation (odds ratio, 3.3).
"These data confirm a team learning curve with NSM and also demonstrate the nipple-sparing approach is suitable for appropriately selected higher-risk patients for both risk reduction and cancer treatment," the authors write.
https://www.practiceupdate.com/C/83453/56?elsca1=emc_enews_topic-alert
https://www.breastsurgeons.org/meeting/2019/press_releases/nipple_sparing.php
-
Detailed Phenotyping and Distinct Trajectories of Cardiovascular Function and Symptoms With Exposure to Modern Breast Cancer Therapy
- Journal: Cancer
- Breast cancer therapies are associated with a risk of cardiac dysfunction, most commonly defined by changes in left ventricular ejection fraction (LVEF). Recently, the authors identified 3 classes of LVEF change after exposure to anthracyclines and/or trastuzumab using latent class growth modeling. The objective of the current study was to characterize the clinical, biochemical, and functional profiles associated with LVEF trajectory class membership.
-
New Lesions ID'd on Breast MRI During Treatment Likely Benign
New suspicious lesions detected on breast MRI during neoadjuvant therapy are more likely benign
For patients undergoing neoadjuvant chemotherapy for locally advanced breast cancer, magnetic resonance imaging (MRI) examinations with new suspicious findings are unlikely to represent a new site of malignancy, according to a study presented at the annual meeting of the American Roentgen Ray Society, held from May 5 to 10 in Honolulu.
Donna Eckstein, M.D., from the University of California in San Francisco, and colleagues identified all breast MRI examinations performed to assess response to neoadjuvant chemotherapy from 2000 to 2018. Study cases classified as Breast Imaging Reporting and Data System (BI-RADS) 4 or 5 were identified. All cases with new suspicious lesions found after initiation of neoadjuvant treatment were included; 28 MRI examinations were included.
The researchers found that all study cases were identified as BI-RADS 4. Sixteen lesions were contralateral to known malignancy, while 11 and one were ipsilateral and bilateral, respectively. Lesions included mass, nonmass enhancement, and focus (18, eight, and two, respectively). Twenty-five of the cases had tissue diagnosis or sufficient imaging follow-up to establish diagnosis; the outcomes were unknown in three cases. In cases with known outcomes, none of the new suspicious findings were malignant, while 11, five, and nine were proven benign at percutaneous biopsy, proven benign at surgical pathology, and presumed benign after resolution of the suspicious lesions or stability over more than two years, respectively.
"Our findings suggest that new suspicious findings on MRI arising during neoadjuvant therapy are almost certainly benign, although larger studies across facilities are needed to confirm whether biopsy may be safely averted in these scenarios," the authors write.
https://www.practiceupdate.com/C/83394/56?elsca1=emc_enews_topic-alert
https://cf.arrs.org/abstracts/oralpresentations/index.cfm?fid=2406
Abstracts 1913-2417
-
Trastuzumab Deruxtecan in Advanced HER2+ Breast Cancer Previously Treated With Trastuzumab Emtansine
- The Lancet Oncology - Published:April 29, 2019
-
Impact of Lymphoscintigraphy as Part of Sentinel Node Biopsy in Early Breast Cancer
- Journal of Clinical Oncology
- The aim of the current work was to clarify whether a preoperative lymphoscintigraphy (LSG) enhances staging accuracy of sentinel lymph node biopsy (SLNB).
DOI: 10.1200/JCO.18.02092 Journal of Clinical OncologyNote: Lymphoscintigraphy (sentinel lymph node mapping) is an imaging technique that is used to identify the lymph drainage basin, determine the number of sentinel nodes, differentiate sentinel nodes from subsequent nodes, locate the sentinel node in an unexpected location, and mark the sentinel node over the skin for biopsy. -
WOW on a roll Lumpie.. many thanks
-
I had gotten behind and have been trying to catch up.
")
-
https://www.medpagetoday.com/hematologyoncology/br...
Adjuvant Denosumab Improved DFS in HR+ Breast Ca
"Combining an every-6-month dose of the osteoporosis medication denosumab (Prolia, Xgeva) with standard adjuvant aromatase-inhibitor treatment significantly delayed disease recurrence in postmenopausal women with hormone receptor-positive breast cancer, according to updated results of the ABCSG-18 trial."
-
https://www.medpagetoday.com/hematologyoncology/br...
Adjuvant Denosumab Improved DFS in HR+ Breast Ca
"Combining an every-6-month dose of the osteoporosis medication denosumab (Prolia, Xgeva) with standard adjuvant aromatase-inhibitor treatment significantly delayed disease recurrence in postmenopausal women with hormone receptor-positive breast cancer, according to updated results of the ABCSG-18 trial.
At 8 years of follow-up, women randomly assigned to denosumab had about a three percentage-point difference in absolute disease-free survival compared with those who received placebo (80.6% vs 77.5%), Michael Gnant, MD, of Medical University of Austria in Vienna, and colleagues reported."
Sources listed in medpage today (see below)
Primary Source
Lancet Oncology
Source Reference: Gnant M, et al "Adjuvant denosumab in postmenopausal patients with hormone receptor-positive breast cancer (ABCSG-18): disease-free survival results from a randomized, double-blind, placebo-controlled, phase 3 trial" Lancet Oncol 2019; DOI: 10.1016/S1470-2045(18)30862-3.Secondary Source
Lancet Oncology
Source Reference: Lippman M "Adjuvant denosumab in postmenopausal patients with hormone receptor-positive breast cancer" Lancet Oncol 2019; DOI: 10.1016/S1470-2045(18)30913-6.
-
Not a scientific journal, none the less interesting: "..opens up the prospect of long-term control with a good quality of life." https://www.theguardian.com/science/2019/may/16/new-war-on-cancer-aims-at-longterm-survival-not-cure
-
Perspectives on Conversations About Costs of Cancer Care of Breast Cancer Survivors and Cancer Center Staff: A Qualitative Study
With the cost of cancer care, and health care in general, there is more and more discussion about the importance of providers having cost of care conversations with patients.
However, as this article highlights, "little formal guidance is available on how to conduct these sensitive conversations in ways that are acceptable to both patients and providers." It is an important step that everyone involved is open to having these critical conversations, but now we need to figure out the actual steps to do so that is best for everyone.DOI: 10.7326/M18-2117
-
Hormone Therapy in Transgender Women Ups Breast Cancer Risk
Transgender women receiving hormone treatments are at greater risk for developing breast cancer than cisgender men, according to a study published online May 15 in The BMJ. {Researchers} retrospectively performed an observational study of transgender women and men who received gender-affirming hormone treatment between the years of 1972 and 2016. Transgender women received a combination of antiandrogens and estrogens for an average duration of 13 years, with treatments beginning at a median age of about 31 years. Transgender men underwent testosterone treatments for an average of eight years, beginning at a median age of 23 years. The incidence and characteristics of breast cancer were compared for those in the cohort and the general population. The researchers identified 18 cases of breast cancer (15 invasive and three noninvasive) in 17 of the 2,260 transgender women after an average of 18 years of hormone treatment. The average age at diagnosis was 50 years. Compared with cisgender men, transgender women had a 46-fold higher risk for breast cancer (standardized incidence ratio [SIR], 46.7); however, this risk was lower than that seen in cisgender women (SIR, 0.3). The majority of these cases were found to be ductal in origin and estrogen and progesterone receptor-positive; 8.3 percent were human epidermal growth factor receptor 2-positive. Invasive breast cancer was diagnosed in four of the 1,229 transgender men (no noninvasive cases were reported), with diagnosis occurring at an average age of 47 years after a median of 15 years of hormone treatment. Compared with cisgender women, this number was lower than expected (SIR, 0.2). This research "suggests that hormone treatment alters the risk of breast cancer in transgender people compared with initial risk based on their birth assigned sex," the authors write.
News report: https://www.practiceupdate.com/C/83943/56?elsca1=emc_enews_topic-alert
Juournal article: https://www.bmj.com/content/365/bmj.l1652
doi: https://doi.org/10.1136/bmj.l1652 (Published 14 May 2019)
{I have not seen a lot of research specific to breast cancer and transgender men and women so I wanted to make a point to share this reference.}
-
Perhaps good news for those of us on Tamoxifen and Antidepressants such as Cymbalta. My MO brought this new study to my attention at our appt yesterday.
https://www.ncbi.nlm.nih.gov/pubmed/30542984CYP2D6-inhibiting medication use and inherited CYP2D6 variation in relation to adverse breast cancer outcomes after tamoxifen therapy
PURPOSE:
Tamoxifen is widely used to reduce the risk of breast cancer (BC) recurrence and extend disease-free survival among women with estrogen-sensitive breast cancers. Tamoxifen efficacy is thought to be attributable to its active metabolite, which is formed through a reaction catalyzed by the P450 enzyme, CYP2D6. Inhibition of tamoxifen metabolism as a result of germline genetic variation and/or use of CYP2D6-inhibiting medications ("inhibitors") is hypothesized to increase the risk of adverse BC outcomes among women taking tamoxifen.
METHODS:
The present cohort study of 960 women diagnosed with early-stage BC between 1993 and 1999 examined the association between concomitant use of CYP2D6 inhibitors and adjuvant tamoxifen and the risk of adverse BC outcomes (recurrence, second primary BC, BC mortality), both overall and according to CYP2D6 metabolic phenotype.
RESULTS:
Six or more months of CYP2D6 inhibitor use concomitant with tamoxifen was not associated with any appreciable increase in risk of recurrence or second primary BC or BC mortality, and there was no clear evidence of variation by CYP2D6 metabolic phenotype.
CONCLUSIONS:
These results are consistent with the relatively few other large, population-based studies conducted to date that have not observed an increased risk of adverse BC outcomes associated with CYP2D6 inhibition.
KEYWORDS:
Breast cancer; CYP2D6; Pharmacogenetics; Survival; Tamoxifen
-
A Rare Genetic Mutation Leads to Cancer. The Fix May Already Be in the Drugstore (NYT Article)
Study: https://science.sciencemag.org/content/364/6441/eaau0159
"In a study published on Thursday in the journal Science, researchers found evidence that a compound called indole-3-carbinol (i3c) blocks an enzyme that inhibits the activity of Pten. With the gene more active, patients with the mutation may be better protected against cancer."
"The mutation is not just inherited; the Pten gene is spontaneously mutated in many tumors. When that happens, the patient's prognosis is poor."
"The gene governs production of an enzyme that stops cells from dividing too quickly, reducing the chances that cancers will form. With reduced activity in Pten, cells grow uncontrollably.Pten mutations do not completely halt the gene's functions. Instead, the mutations tamp down the gene's activity, so cells make less of the enzyme needed for orderly growth.
But one of the hardest things for researchers to do is to find a way to increase, rather than turn off, a gene's activity. Eventually, Dr. Pandolfi and his colleagues learned enough about the Pten system to reason that i3c might do the trick.
"We got lucky, or smart," he said.
Dr. Pandolfi and his colleagues tested their treatment on human prostate cancer cells and in mice bred to develop prostate cancer. It worked: In the cells and in mice, i3c treatment resulted in fewer cancers, and those that arose were small and less deadly."
Keywords: DIM Supplement, i3c, Indole-3-Carbinol
-
Also, there is this new breaking news...
A Rare Genetic Mutation Leads to Cancer. The Fix May Already Be in the Drugstore (NYT Article)
Study: https://science.sciencemag.org/content/364/6441/eaau0159
"In a study published on Thursday in the journal Science, researchers found evidence that a compound called indole-3-carbinol (i3c) blocks an enzyme that inhibits the activity of Pten. With the gene more active, patients with the mutation may be better protected against cancer."
"The mutation is not just inherited; the Pten gene is spontaneously mutated in many tumors. When that happens, the patient's prognosis is poor."
"The gene governs production of an enzyme that stops cells from dividing too quickly, reducing the chances that cancers will form. With reduced activity in Pten, cells grow uncontrollably.Pten mutations do not completely halt the gene's functions. Instead, the mutations tamp down the gene's activity, so cells make less of the enzyme needed for orderly growth.
But one of the hardest things for researchers to do is to find a way to increase, rather than turn off, a gene's activity. Eventually, Dr. Pandolfi and his colleagues learned enough about the Pten system to reason that i3c might do the trick.
"We got lucky, or smart," he said.
Dr. Pandolfi and his colleagues tested their treatment on human prostate cancer cells and in mice bred to develop prostate cancer. It worked: In the cells and in mice, i3c treatment resulted in fewer cancers, and those that arose were small and less deadly."
Keywords: DIM Supplement, i3c, Indole-3-Carbinol
Glad to hear that one of the supplements I'm taking is DIM. Fingers crossed. -
First U.S. use of CRISPR to directly target cancer will seek go-ahead from regulators
If all goes as planned, the first clinical trial in the United States testing CRISPR against cancer by altering the DNA of tumor cells inside patients could begin recruiting participants next year, the scientist leading the effort told STAT.
The Gene Editing Institute....is preparing to seek regulatory approval for a much bolder CRISPR cancer study. If it receives the OK from the Food and Drug Administration, which it plans to request in the next few months, it would recruit six to 10 patients with late stage non-small-cell lung cancer and test whether using CRISPR to disable a particular gene would allow standard chemotherapy to work better and longer, ideally buying patients a little more time. "The goal is to give them a few more months of life, but we hope there will be additional benefits."
His target: a gene called NRF2 (nuclear factor erythroid 2-related factor). It produces a protein called a transcription factor, which activates some 200 genes that, among other things, pump alien chemicals out of tumor cells. Those chemicals include the chemotherapy drugs cisplatin and carboplatin, so lung cancer cells become resistant to them. "NRF2 is a major culprit in fighting off cisplatin and carboplatin," Kmiec said. "And expression of NRF2 increases as lung cancer goes from stage 1 to 2 to 3 to 4," advancing first to the lymph nodes and then to distant organs. "We thought it would make a good target."
One reason to believe the edit will hit its target and nothing else is that cells with high expression of NRF2 have a little chunk of DNA that serves as a roadside beacon for CRISPR. Healthy cells lack it. Called a PAM sequence, it should ensure that CRISPR disables NRF2 only in tumor cells and not normal ones.
Because the trial will recruit patients with lung cancer so advanced (stage 3 or 4) they have at most six months to live, Kmiec hopes that regulators will demand fewer guarantees of safety. For instance, there have been concerns that CRISPR'd cells might be prone to developing new cancers decades hence. But that might not be relevant to patients with almost no chance to live that long. Exactly what safety assurances the FDA will require, however, is unclear.
"I think we'll be underway in 18 months," Kmiec said, "but it might be earlier."
{Site may require a sign in but there is not a fee for access.}
-
'I want to live': Women share realities of living with terminal breast cancer, raise money to eradicate the disease
POSTED 6:54 AM, MAY 24, 2019, BY STACEY FREY, UPDATED AT 08:41AM, MAY 24, 2019
Not research, but some of you may be interested in seeing this news report on a group of women in the Cleveland, Ohio, area supporting one another through MBC. Nice to get some coverage of MBC! They have a fundraiser coming up. There's a link in the print report.
-
Liquid biopsy could identify cancer patients at risk of metastatic disease, offering an opportunity to tailor treatment
Analysing fragments of DNA that are shed by tumours into the bloodstream, could indicate early on whether patients are at risk of their cancer spreading, according to new research presented today.
16 May 2019
Researchers at The Royal Marsden say ctDNA, a form of liquid biopsy, may be an accurate technique to monitor treatment response in patients with locally advanced rectal cancer, allowing treatment to be adapted or changed earlier to try to prevent the development of metastatic disease.
"Importantly what this study showed, which has not yet been explored, is that persistence of ctDNA mid-way through treatment could be an early indicator of the cancer's potential to spread. Using this measure, along with MRI scans, we can offer a more personalised treatment approach for patients." "Whilst our findings are interesting and exciting, it's important to note that this was carried out in a small cohort of patients and would require further validation in a larger trial."
-
New method of breast reconstruction may reduce pain for some cancer survivors
NOVEMBER 21, 2018
But in recent years...surgeons have found a way to keep the implant on top of the muscle and address those problems: they're surrounding the implants with a biologic mesh, essentially a thin layer of collagen.
"Now we can put the implants under the skin and a subsequent next layer of biologic mesh to protect the implant – so the implants are not right under skin, so the implants are sitting under a layer of mesh, in a pocket we've created using the mesh," said Sbitany. "In essence, we have the ability to do a totally muscle-sparing, muscle-preserving breast reconstruction."
The fat grafting helps to be able to add protection around the implant and better contour the shape of the new breast, he said.
we've found this is a very safe option in the setting of radiation," said Sbitany.
Another benefit of avoiding dissecting the pectoral muscle is a substantial reduction in pain.
-
Surveillance After Treatment of Localized Breast Cancer: Time for Reappraisal?
https://www.medscape.com/viewarticle/912080?src=wnl_edit_tpal&uac=153476CT&impID=1974273&faf=1
The lead author, Joseph Sparano, is a highly respected figure in breast cancer research and probably familiar to many of you. It seems to me that if he's discussing this topic there is hope that it will arouse interest in the wider oncology community sooner rather than later.
(You may need to register to read the article but it's free and non-intrusive.)
-
Seems we can’t access this link Lumpie, but appreciate the effort! Kare
-
Is it better to 'contain' rather than destroy cancer?
A recent study in mice has found that an existing drug could effectively contain metastatic breast cancer cells.
Existing drug can block stray cancer cells
The researchers zeroed in on the drug fostamatinib, which is currently approved for the treatment of immune thrombocytopenia, an autoimmune disease characterized by a low platelet count in the blood.
The team explains that their research in mice has shown that fostamatinib is also able to contain metastatic cancer cells and stop them from developing into full tumors, causing further damage.
-
-
Thanks for posting, mysticalcity. That was at once both hopeful and terrifying!
-
First-in-Class Treatment Approved for Advanced Breast Cancer
https://www.empr.com/home/news/first-in-class-trea... -
Promising HER2+ cancer research out of Turku, Finland, funded by our Pink Ribbon campaign. Inhibiting SORLA protein inhibits HER2+ cell growth. Only at the lab bench stage, but I'm excited about all new findings that can potentially help us!
https://www.nature.com/articles/s41467-019-10275-0
-
Proposed legislation aims to boost patient access to data The Lower Health Care Costs Act of 2019, a proposal introduced by the Senate Health, Education, Labor, and Pensions Committee, aims to promote health information exchange, enhance the security and privacy of health data, and reduce health care costs. The bill, which is open for public comment until June 5, "ensures that patients have full, electronic access to their own health information and information on what the patient would pay out of pocket for specific care" and "emphasizes that all existing privacy and security protections for patient health data under HIPAA and state laws apply," according to a summary of the draft legislation.Health Data Management (free registration) (5/28)
-
WHO urges members to publicly disclose drug price info
A World Health Organization committee agreed to a draft resolution that urges member states to share information on net drug prices with the public and support distribution of voluntarily provided or publicly available information about clinical trial costs. The resolution did not support requiring drugmakers to disclose research and development costs, as some activists had suggested.Reuters (5/28)
-
Seniors' out-of-pocket spending on cancer drugs rises
Seniors now pay an average of $10,470 annually out of pocket for cancer drugs through Medicare Part D, up from $8,794 in 2010, according to a study in the Journal of the American Medical Association. Researchers said new cancer drugs have substantially higher starting price points while prices for older drugs have steadily increased.
Prices for 13 anticancer drugs available through Medicare Part D in 2010 rose an average 8% over inflation every year over the past decade...
"We're also seeing that the newer products are just starting out with higher price points,"
In 2018, 48 of the 54 medications had monthly prices exceeding $10,000 per prescription fill, and 21 cost more than $15,000 per fill...
"There is no major increase in the cost of manufacture of those drugs," Fishman said. "These quite substantial cumulative increases are just a result of the power of these drug manufacturers to set price and increase price."
-
Grail, a deep-pocketed startup, shows 'impressive,' if early, results for cancer blood test
Could a blood test detect cancer in healthy people? Grail, a Menlo Park, Calif.-based company, has raised $1.6 billion in venture capital to prove the answer is yes. And at the world's largest meeting of cancer doctors, the company is unveiling data that seem designed to assuage the concerns and fears of its doubters and critics. But outside experts emphasize there is still a long way to go.
The data, from a pilot study that Grail is using to develop its diagnostic before running it through the gantlet of two much larger clinical trials, are being presented Saturday in several poster sessions at the annual meeting of the American Society of Clinical Oncology. The data show that the company's test can detect cancer in the blood with relatively few false positives and that it is fairly accurate at identifying where in the body the tumor was found. Another abstract seems to show that the test is more likely to identify tumors if they are more deadly. One big worry with a cancer blood test is that it would lead to large numbers of patients being diagnosed with mild tumors that would be better off untreated.
"The progress of the technology is impressive," said Dr. Len Lichtenfeld, the acting chief medical officer of the American Cancer Society. But he also urged caution. "Grail is one organization that is pursuing this goal. We will get there. But we still have to prove the technology, and we still have to learn how to apply the technology."
Dr. Eric Topol, the director and founder of the Scripps Research Translational Institute, called the results "encouraging" and commented that Grail is "trending toward credibility." He agreed that if these early results hold up, the blood test could be more predictive than existing screening tools, like prostate-specific antigen or mammography. But he, too, emphasized the need for much more research. "All of this requires a large, prospective assessment," he wrote via email.
Grail is running a preliminary study called the Circulating Cell-Free Genome Atlas (CCGA), which is being conducted in 15,000 patients. The goal from the beginning was to use this study to optimize a diagnostic test. This would then be tested in two more studies: one of 100,000 women enrolled at the time of their first mammogram, and a second of 50,000 men and women between the ages of 50 and 77 in London who have not been diagnosed with cancer. These huge studies are one reason Grail has raised so much money.
But the data being reported at the ASCO meeting are from a tiny sliver of that first study: an initial analysis of 2,301 participants from the training phase of the sub-study, including 1,422 people known to have cancer and 879 who have not been diagnosed. These data are being used to pick exactly what test Grail will run.
Dr. Steven Joffe, the chief of the division of medical ethics at the University of Pennsylvania Perelman School of Medicine, called it "important and necessary work, but very different from the envisioned use as a screening tool."
The first big surprise is exactly what test the company is using. When it was spun out of DNA sequencing giant Illumina in 2016, Grail was focused on genes. The idea was that little bits of DNA shed by cancer cells could be detected in the blood. But Grail is now not looking at the genes themselves, but patterns called methylation, which is used by the body to change how the genetic code is read.
"You start out with a few cells, but then they become tremendously differentiated into brain cells, heart cells, skin cells, all of those things," said Dr. Alex Aravanis, Grail's head of research and development. "Methylation is the fundamental signal that determines those cell identities and cell fates."
Grail had previously presented strategies of using DNA in the blood to detect cancer: sequencing the entire genetic code, or a targeted panel of genes, or using methylation. Aravanis said that methylation was not only the most accurate method, but the best at telling where the tumor originated — whether it was breast cancer, lung cancer, or pancreatic cancer, for instance, that the patient had.
The test was set up so that it would have a 99% specificity — meaning that for every 100 people told they had cancer, 1% would actually not have the disease. The test could detect 34% of cancers at stage 1, when the cancer is least risky, 77% at stage 2, and 84% at stage 3. For 94% of patients, the diagnostic gave the tissue of origin of the test, and it was right nine times out of 10.
Ability to correctly identify where the cancer was varied by tumor type. At 99% specificity, the test identified 59% of early-stage lung cancers, 74% of colorectal cancers, and 78% of pancreatic cancers. The test got better when later-stage cancers were included: identifying location for 92% of lung cancers, 97% of colorectal cancers, and 79% of pancreatic cancers.
With these data, it's possible to start to imagine what the use of a Grail cancer blood test would look like in the real world. Dr. Anne-Renee Hartman, Grail's vice president of clinical development, said that between 1% and 1.5% of people older than 50 develop cancer each year. So a test that looked at 100,000 individuals and detected cancer in 70% of them would find 700 cancers. If it had a 99% specificity, it would tell 1,000 people who do not have cancer that they had the disease. The test would tell doctors where to look, and they would have to calm those whose tumors could not be found and treat those whose tumors were findable.
This may not sound great. The test would still be scaring more people unnecessarily than it's helping. But Hartman and Aravanis pointed out that that's far better than existing tests like mammography, CT screening, or PSA. Those, Aravanis said, have false positive rates that are 10 times higher.
Still, while the Grail executives said they envision the company's test used to screen large numbers of people, they also pointed out that their big studies contain plenty of people at higher risk, like heavy smokers or people with mutations known to increase their risk of cancer. Anirban Maitra, a pancreatic cancer researcher at MD Anderson Cancer Center, said that if you look just at pancreatic cancer, not all cancers, it's likely almost 1,000 people who don't have cancer would be identified for every 15 that are diagnosed. "It may be better to apply tests of this nature in a pre-selected high risk population (mutation carriers, or cohorts being followed for cancer surveillance due to some concurrent high risk features) before going all in on a general population," he said.
Dr. Charu Aggarwal, an assistant professor of medicine at the University of Pennsylvania, said she, too, would like to see the test tried in patients at higher risk. But she also was surprised and impressed by the data. "I'm really intrigued," she said.
Aravanis also argued that Grail has another advantage here: that it appears to be detecting deadlier early-stage tumors, no matter where they are in the body. "All cancers are not the same. We really want to find those cancers that are dangerous that grow, progress and cause clinical harm," he said.
Grail is taking the next steps. Hartman, its head of clinical development, said that the company plans to soon start experiments where it will return results back to patients and their doctors, so they can understand what patients do with the information. Until now, Grail has been taking patients' blood and watching, but not telling them about the results of its still-experimental tests.
Dr. Otis Brawley, a professor of oncology and epidemiology at Johns Hopkins University, said he was impressed by the data.
"This is truly exciting in that it's a company that has consistently tried to do the right thing in developing a screening test," he said. "Many companies have tried to cut corners."
Aravanis also said that the company is cognizant that its final test can't be too expensive, and that it is targeting small enough areas of the genome that it can make the test affordable. "We want this to be broadly accessible when deployed," he said. "Being able to price it in a way that's compatible with that is very important to us." He gave a range from $600 to a few thousand dollars, and said that it would get to the low end of that range if possible.
There will definitely be competition. Yesterday, Thrive, a Cambridge., Mass.-based company, announced that it had raised $110 million to develop a competing test developed by researchers at Johns Hopkins University. That test combines DNA and protein data to tell where in the body tumors are. Thrive says its test will cost hundreds of dollars. The race is on.
Matthew Herper, Senior Writer, Medicine, STAT News
-
Brain Metastases From HER2-Positive Breast Cancer
- This retrospective study was designed to evaluate the impact of local and systemic therapies for patients with brain metastases related to HER2+ breast cancer.
- Patients treated with surgery or stereotactic radiosurgery and HER2-targeted therapy experienced the best outcomes, whereas patients with a low performance status and neurologic symptoms experienced worse outcomes.
BACKGROUND
There is no sufficient evidence to establish a standard of care for patients with brain metastases (BM) from HER2-positive (HER2+) breast cancer (BC). The aim of this study was to assess the impact of local and systemic treatments on the outcome of patients diagnosed with BM from HER2+BC over a period of 10 years, from 2005 to 2014.
METHODS
Data of 154 patients were retrospectively collected at 14 Italian institutions through a specifically designed database
CONCLUSIONS
Patients with BM from HER2+BC treated with surgery/SRS as local treatment and HER2-targeted therapy as systemic treatment achieved the best outcomes. Patients with low Karnofsky performance score (KPS) and neurological symptoms had poor survival.
Commentary on study provided by Lillie D Shockney RN, BS, MAS
https://www.practiceupdate.com/C/84183/56?elsca1=emc_enews_topic-alert
https://www.clinical-breast-cancer.com/article/S1526-8209(19)30011-4/abstract
-
I was a 31-year-old kid in a way': How a cancer diagnosis changed a health care reporter
Rebecca Robbins and Damian Garde and Adam Feuerstein, STAT News • May 24, 2019
All health care reporters deal with the medical system outside of work. But not many of them have dealt with it like Alexandra Glorioso has in recent months.
Glorioso is a reporter for Politico. She's based in Tallahassee, Fla., and she writes about health care, insurance, and the state legislature. She covers stories like the push to expand Medicaid in Florida and legislative proposals to rein in drug costs.
Last summer, at age 31, Glorioso was diagnosed with stage 2 breast cancer. She underwent chemotherapy, participated in a clinical trial with an experimental drug, and had surgery. Then, in March, she announced she was in remission, with no evidence of disease. This week, Glorioso talked with STAT about what the whole experience has been like — and how it shaped her thinking as a health care reporter.
Go to:
https://news.yahoo.com/31-old-kid-way-cancer-084540348.html
for coverage of the interview.
{Story originally published by STAT news. Lightly edited version published at Yahoo News. Free access at Yahoo or subscribe to STAT.}
Alexandra Glorioso's article
I'm Coping With Cancer by Reporting On It. This is what it's like to go from journalist to patient.
Can be accessed here:
https://www.politico.com/magazine/story/2018/08/19/im-coping-with-cancer-by-reporting-on-it-219372
-
Health spending and life expectancy, 1970-2017
The Economist
It is difficult to argue with this chart showing America is getting a much lower return on investment of our health care dollars than other countries. There are obviously no easy answers, but this seems quite simply unsustainable.{check out the great chart!}
"THE REPUBLICAN PARTY will soon be known as the party of health care—you watch," President Donald Trump declared in March. "We're coming up with plans." Alas, like many of Mr Trump's claims, this one proved untrue. Days later, following conversations with Mitch McConnell, the Republican Senate majority leader, Mr Trump admitted via tweet that his much-touted health-care proposal would in fact be delayed until at least 2021 after "Republicans hold the Senate & win back the House".
Republican reluctance to embrace health care, despite the president's best efforts, is understandable. On the one hand, America's health-care system is woefully dysfunctional: the country spends about twice as much on health care as other rich countries but has the highest infant-mortality rate and the lowest life expectancy (see chart). Some 30m people, including 6m non-citizens, remain uninsured. And yet, though costs remain a major concern—out-of-pocket spending on insurance continues to rise—Americans say they are generally satisfied with their own health care. Eight in ten rate the quality of their care as "good" or "excellent". Few are in favour of dramatic reform.
{Access to full article requires subscription. This article noted by NCCS.}
-
Researchers are hoping any positive outcomes can be appliedhumans in the future.
https://news.wisc.edu/clinical-trial-begins-to-test-universal-vaccine-against-canine-cancer/
The trial is slated to run over five years. Cancer-free, healthy dogs between the ages of six to 10 will be randomized to receive either a series of the investigational vaccine or placebo vaccines.
Two sets of vaccines will be given every two weeks, for a total of four treatments, and then annually. Researchers have not observed any side effects other than those typical to any vaccine, such as moderate local pain or swelling at the site of injection, in mice or dogs to date, but the study will characterize any unanticipated adverse reactions in the larger study population.
-
I thought I would post links to a couple of research studies that may be of interest. Both seek stool samples.
This one actually pays you for them! And its stated mission is to make cancer treatment more effective.
This one is "citizen funded" which means you pay to participate.
-
Breast Cancer Histologic Subtypes Cluster in Families
- Using a large, population-based database, the authors sought to investigate familial clustering of breast cancer by histologic subtype. The authors identified 23,629 individuals who had more than three generations of genealogy and more than one primary breast cancer; 2883 had specific histologic subtypes other than invasive ductal carcinoma (eg, inflammatory, lobular, and mucinous). The relative risk (RR) for breast cancer was increased among second-degree relatives of patients with inflammatory (RR, 1.32), lobular (RR, 1.36), and mucinous (RR, 1.27) subtypes.
- The lobular, mucinous, and inflammatory histologic subtypes of breast carcinomas appear to cluster within families, but the genetic variants responsible for increased risk and inheritance need to be identified.
- CONCLUSIONS: These findings provide evidence for significant familial clustering within histological subtypes for lobular, mucinous, and inflammatory breast carcinomas. Further research is required to identify the underlying genetic variants responsible for the increased risk. Studies of high-risk pedigrees segregating a specific histologic subtype could be a powerful design for predisposition gene identification.
DOI: 10.1002/cncr.32198 -
Resistance Mechanisms to Anti-HER2 Therapies in HER2-Positive Breast Cancer
- The authors of this review highlight current knowledge regarding the mechanisms involved in the development of anti-HER2 therapy resistance in HER2-positive breast cancer.
- The authors provide detail on mechanisms such as impaired drug binding to HER2, constitutive and self-sufficient signaling in HER-related signaling pathways, metabolic reprograming, and attenuation of the immune system activation state.
HER2-positive breast cancer (HER2 + BC) represents 15-20% of all BCs. In the last two decades, the introduction of monoclonal antibodies (MoAbs), tyrosine kinase inhibitors (TKIs) and antibody-drug conjugates (ADCs) directed against HER2 impressively improved patient prognosis in all disease stages.
Yet, not all patients with limited-stage disease are cured, and HER2+ metastatic BC (mBC) remains an almost invariably deadly disease. Primary or acquired resistance to anti-HER2 therapies is responsible for most treatment failures. In recent years, several resistance mechanisms have been identified, such as impaired drug binding to HER2, constitutive activation of signaling pathways parallel or downstream of HER2, metabolic reprogramming or reduced immune system activation. However, only a few of them have been validated in clinical series; moreover, in the era of standard-of-care dual HER2 blockade, these mechanisms should be re-assessed and, in case, confirmed with anti-HER2 combinations.
Defining the best strategies to delay or revert resistance to anti-HER2 treatments will be crucial to improve their clinical efficacy.
-
On a roll Lumpie, thank you
-
Drugs make headway against lung, breast, prostate cancers
Kisqali...best
https://apnews.com/4c83cc7cc92a430b8c026691e77815c... -
AKT Inhibitor Doubles PFS in Advanced Breast Cancer
Early randomized trial of capivasertib shows promise in ER-positive disease
-
Heart Meds Help in HER2+ Breast Cancer Patients
-ACE inhibitor or beta-blocker cuts cardiotoxicity in patients treated with trastuzumab and anthracyclines
-
New Principle for Eradicating Cancer: Leave No Dead Cells Behind
Killing cancer cells is the fundamental objective of chemotherapy, radiation and targeted cancer therapies. However, these treatments often fail to eradicate tumors, and cancer often recurs.
So, is killing the problem?
Dr. Sui Huang (pictured above), professor and cancer biologist at Institute for Systems Biology, along with former mentee and longtime collaborator Dr. Dipak Panigrahy at Beth Isreal Deaconess Medical Center in Boston and colleagues at Harvard Medical School, show that dead cells, or cell debris, generated by treatments intended to eradicate tumor cells, actually act as strong stimulators of tumor progression. Their findings were published in The Journal of Experimental Medicine on November 30 {2017}.
Traditional cancer therapies, then, become a double-edged sword: Too much and too fast, yet incomplete, killing of the tumor cell population will generate so much debris that the tumor stimulatory effect overpowers the decimation of tumor cells. The dead cells trigger a reaction that strengthens the cancer cells that have just escaped death by drugs: These become more like stem cells, which are resilient and robust, and eventually cause recurrence of the tumor.
This phenomenon of cancer drugs as a double-edged sword may be considered discouraging. (Will cancer drugs then ever work?) However, knowing about new mechanisms offers new strategies for new drugs.
"As with wars, focusing solely on killing thy enemy may not be productive and can backfire," Huang said. "A broad assessment of the enemy's culture, the danger of empowering them by attacks and parallel diplomacy help. What politicians and military leaders have long learned, cancer research is now realizing: Look beyond just making killing more efficient. This new vista may open ample new opportunities for gentler, less toxic non-killing – but effective – anti-cancer drugs."
https://systemsbiology.org/news/2017/11/30/cancer-debris/
http://jem.rupress.org/content/215/1/115
DOI: 10.1084/jem.20170681
-
High-Deductible Plans and Breast Cancer: Not What You Want to See
Diagnosis made nearly 7 months later than for women in low-deductible plans
High-deductible health plans (HDHPs) were linked to delays in diagnosis and treatment for breast cancer among low-income women, J. Frank Wharam, MD, said here at the AcademyHealth Annual Research Meeting.
High-deductible health plans -- in which patients pay lower premiums than traditional health plans but pay deductibles ranging anywhere from $1,000 to $7,000 before coverage kicks in -- are becoming an increasingly larger part of the health insurance landscape, Wharam noted. "Between 2006 and 2018, HDHPs grew to [cover] almost 60% of workers...
"Rural women in HDHPs experienced substantial delays across the arc of cancer care, from diagnostic testing to treatment," said Wharam. "Adding high out-of-pocket costs to preexisting barriers might cause especially pronounced 'financial toxicity' among rural women."
"We believe further research is needed to determine if these delays cause adverse health outcomes; we're trying to work on that now,"
https://www.healthaffairs.org/doi/abs/10.1377/hlthaff.2018.05026
-
Lumpie--if you take requests, I think you should make a new thread about that persephone biome study. I bet there would be lots of takers.
-
Ingerp: I take requests! That's a great idea! I'll do that.
And in case anyone needs a link immediately... here you go:
Poop for the Cure
-
Apparently they don't want Canadian poop!. I was so ready!
-
My BS is absolutely convinced that low Vit D levels are a big contributor to BC so it was interesting to read that article. My levels were horribly low at diagnosis and that's despite having an outdoor job. He says it's because we use so much sunscreen.
-
hahahaha Greek Ninja!
-
Sorry, Greek. Hope you’re not personally insulted. I hear it smells like maple syrup.
-
Yes it smells like maple syrup and looks like poutine.
-
<like!>
-
Shetland ...I've been following the MSH6 studies. I had Myriad testing prior to diagnosis (where they told me I had a very low chance of getting breast cancer) and then got diagnosed within months. I have the MSH6 variant which, at the time, was noted as a "variant of unknown significance". The genetic counselor told me to keep checking in because as they collect more data, they tie more genes besides BRCA to breast cancer. And sure enough....
The study reads that a normal woman has a 15% chance of getting breast cancer while a woman with an MSH6 variant has a 30-38% chance of getting breast cancer.
I just don't understand why they can't move faster with this research. It's frustrating.
-
Drug to Replace Chemotherapy May Reshape Cancer Care
http://www.bnnbloomberg.ca/drug-to-replace-chemoth... -
lala1: regarding the vitamin D levels.... I have done some reading about this because my D levels are sometimes low. My impression is that there seems to still be a good deal of uncertainty around any consequence of vitamin D produced by your body vs vitamin D taken in table/capsule form. I know that they have identified at least one, and quite possibly more, genetic mutations that can be related to vitamin D synthesis. But even people with homozygous (two) mutated genes sometimes do ok so there is obviously more to the story than just the gene pair I have read about. It is possible to be tested but I think that most physicians feel it is not worth it. If you have done a genealogy DNA test, you can run your results thru an analyzer at https://promethease.com/.
-
This courtesy of Ingerp (I don't think it is already posted...)
STUDY: UNHEALTHY GUT PROMOTES SPREAD OF BREAST CANCER
An unhealthy, inflamed gut causes breast cancer to become much more invasive and spread more quickly to other parts of the body, new research from the University of Virginia Cancer Center suggests.
...a research faculty ...found that disrupting the microbiome of mice caused hormone receptor-positive breast cancer to become more aggressive. Altering the microbiome, the collection of microorganisms that live in the gut and elsewhere, had dramatic effects in the body, priming the cancer to spread.
https://news.virginia.edu/content/study-unhealthy-gut-promotes-spread-breast-cancer?
http://cancerres.aacrjournals.org/content/early/2019/05/07/0008-5472.CAN-18-3464
DOI: 10.1158/0008-5472.CAN-18-3464
(access to full journal article requires subscription)
-
Here's a little more about Marijen's article... sounds promising....
Drug to replace chemotherapy may reshape cancer care
A class of drugs is emerging that can attack cancer cells in the body without damaging surrounding healthy ones. They have the potential to replace chemotherapy and its disruptive side effects, reshaping the future of cancer care.
The complex biological medicines, called antibody drug conjugates (ADCs), have been in development for decades, and are now generating renewed excitement because of the success of one ADC in late-stage testing, a breast cancer treatment called DS-8201.
"DS-8201 may become one of the largest cancer biologic drugs,''
Analysts say DS-8201 could triple the number of patients who get powerful targeted treatment for breast cancer, the most common tumor in women that kills more than half a million annually. As importantly, its ability to target cancer cells without affecting normal cells is a key advantage over the take-no-prisoners approach of chemotherapy.
Daiichi's treatment has been seen to double survival time for advanced breast cancer patients ... patients using DS-8201 experienced less nausea and hair loss compared with chemotherapy.
DS-8201's full potential is still years away, as it will take time for data to validate the drug's efficacy in a wide range of patients....About 56 pharmaceutical companies are developing ADC candidates..."ADCs are being positioned as a chemo replacement,''
The concept behind ADCs was envisioned in 1900 by German Nobel laureate Paul Ehrlich, who formed the idea of a "magic bullet" in which a single toxic molecule would be delivered to attack a diseased cell without damaging surrounding healthy cells.
The actual use of ADCs began in 2000, but the interest in the sector cooled down as many failed to live up to expectations. The therapies belong to a broader category of cancer immunotherapies that include Merck & Co.'s Keytruda and Novartis AG's CAR T-cell therapy Kymriah that harness the immune system to kill tumors.
Daiichi Sankyo's drug takes ADCs to another level. Its advantage is that it carries eight payloads stably to cancer cells, double the number of the industry standard..."Currently available ADCs are far from being perfect technically because the payload linked to antibodies aren't properly delivered to cancer cells,''... "We wanted to challenge and improve that.
{For HER2 BC}...their first treatment is chemotherapy alongside Roche's Herceptin and Perjeta, a related drug. While DS-8201 is currently in testing for later-stage cancer, the plan is to go up against the first-line treatment *in the next two years.* {emphasis added}
"It would be transformative" if the drug were to become the sole first-line treatment...."If we can eliminate the side effects associated with chemotherapy, that would be a tremendous benefit for women."
"...my gut feeling is that DS-8201 is the most effective among existing medicines targeting HER2 positive patients, including Herceptin and chemotherapy,'' said Shunji Takahashi, deputy director at the Cancer Institute Hospital of the Japanese Foundation for Cancer Research, who took a part in an early-stage DS-8201 trial. He noted that interstitial pneumonia is a concern as a side effect, and needs to be monitored.
https://www.bnnbloomberg.ca/drug-to-replace-chemotherapy-may-reshape-cancer-care-1.1271773
-
On this: "STUDY: UNHEALTHY GUT PROMOTES SPREAD OF BREAST CANCER" interesting concept and study. It would be more useful if we could define better what really IS a healthy gut and how to get it. Yes, eating a varied, high-fiber, high-vegetation diet and getting plenty of sleep, and having low stress, all probably helps. I think it's hard for many people to grasp that as any prescription for living, achieving a healthy gut, low inflammation, and lower risk of cancer.
Not meaning to shoot the messenger here... Thanks as always for posting these.
-
Very good question Mountain Mia. You can do a search and find bits and pieces or here is a best seller. Doctors don’t know much about healthy eating unfortunately.
The Microbiome Solution: A Radical New Way to Heal Your Body from the Inside Out Paperback – August 9, 2016
by Dr. Robynne Chutkan M.D. (Author)
4.5 out of 5 stars 217 customer reviews#1 Best Sellerin Gastroenterology
ISBN-13: 978-0399573507 ISBN-10: 039957350X Edition: Reprint
-
MountainMi: true. I think that this is still an evolving area of knowledge. There are at least a couple of ongoing studies. If you are interested, I have posted info on those in this thread:
https://community.breastcancer.org/forum/73/topics/871909?page=1#idx_13
See entries regarding The American Gut Project and the British Gut and The Persephone Biome study.
-
Oh this is very interesting, hope you don’t mind lumpie!
Can an Airport Scanner Detect a Tumor or Medical Issue? - YouTube
-
Regarding Vit D testing--previous MO required, new MO requires it. It's easy to do within the CBC panel labs that I have done before each check up, so (so far) my Vit D is still being monitored. I take Vit D liquid supps (4000 IUs) and when I hike, or walk the dog (nearly every day) I don't use sunblock and try to expose arms and legs for 30 min. My levels are so far above 60, mostly hover around mid 70s. Both MOs wanted levels at 70+, Naturopath wants at least that. MOs get concerned when it rises above 80 since it can skew blood calcium on labs, so 4000 IUs plus exposure seems right to me. At any rate, Vit D testing and supplementing doesn't seem to cause me any harm.
Claire in AZ
-
Sounds promising:
Tumor cells that spread cancer via the bloodstream face a new foe: a laser beam, shined from outside the skin, that finds and kills these metastatic little demons on the spot.
-
Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer
- This prospective trial involved 9427 women with HR-positive, HER2-negative, axillary node–negative breast cancer in whom an assay of 21 genes had been performed. Their clinical risk of recurrence of breast cancer was classified as low or high on the basis of the tumor size and histologic grade.
- The authors found that clinical-risk stratification provided prognostic information that facilitated the identification of premenopausal women who could benefit from more effective therapy when this prognostic information was combined with the 21-gene recurrence score.
DOI: 10.1056/NEJMoa1904819 -
This op-ed piece may be of interest to some:
New Program Will Offer Unapproved Drugs to Dying Cancer Patients
Kevin Campbell looks at the pros and cons of this controversial FDA decision
-
Lazer Beam.... what took them so long?
-
Great if the Airport Scanners give you a heads up, but don't count on them for diagnostics. An editorial word of caution about those "health scans" provided by some "virtual physical" centers, also. My impression is that they may be pretty good for cardiac issues but they are not very good for cancer detection. Some market themselves as providing early detection of cancer but if you question the providers, they will tell you what most of us know which is that you are not likely to see anything cancerous without contract - which they do no provide. So.... have realistic expectations.
-
Well I worry about how much radiation we are getting from the airport scanners that they can see into our bodies. That’s not nice. Intrusion of privacy.
-
I just found this one, not sure if it's already been posted. I don't particularly understand it, but sounds promising at least.
-
If you are interested in business start-ups doing cancer research and development, you may be interested in this "blast" that came out from Angel List (angel.co)
Cancer sucks, but there are some exciting developments on the research front. In the last month alone, we've seen regulators consider a CRISPR therapy that directly targets tumor cells—a first for the U.S.—as well as a laser that zaps tumor cells from patients bloodstreams without damaging healthy tissues.
And it's not just the research around new cancer therapies that's exciting. There's a host of startups attempting to tackle other parts of the cancer treatment puzzle, from diagnostics, to emotional support, to medical record logistics.
In the world of diagnostics and early detection, we have startups like:
- Freenome, backed by a16z, using unique blood tests and AI to detect early signs of cancer.
- Ezra, using full-body MRIs and machine learning to detect 11 kinds of cancer in men and 13 in women.
On the logistical side of treatment, there are startups like:
- Flatiron Health, a collaborative platform for doctors, academics, regulators, and more.
- Embleema, a blockchain company for patient health data, which has partnered with Europe's leading cancer center.
And then there are other cancer-focused startups that are tougher to categorize, like Belong.life. A platform for cancer patients, it offers a social network where users can connect with other patients, explore a clinical trial matching service, leverage oncologist-staffed support chat, and use a file storage system for medical records.
The number of people diagnosed with cancer makes the potential for impact huge, while the difficulty of the market's core problems makes the barrier to entry for companies high. For a startup looking to innovate and affect as many individuals as possible, there might not be a more exciting space. If you're interested in joining such a startup, search AngelList here.
-
Re: DS-8201 and the hope that it will someday replace chemo and its toxic side effects - it's important for people to know that based on Phase I and II trials of DS-8201, the rate of Grade 3 and higher Adverse Events was 50+% (50% for breast cancer, 64% for gastric cancer), 22.9% had a "serious" AE (ie life-threatening, Grade 5 is death), the rate of interstitial lung disease (ILD) has been so high that they now have an independent outside agency monitoring it during the Phase III trials, and the drug was directly responsible for the death of 2 out of the original 12 breast cancer patients in the Phase I trial. Despite those horrific stats, they claim that maximum toxicity was never achieved in Phase I and the drug is "well tolerated". The rate of AEs in Phase II was similar to the rate in Phase I. Other than the ILD, the most common all-grade AEs were "nausea (79.4 percent), decreased appetite (54.1 percent), alopecia (46.5 percent), vomiting (45.9 percent), fatigue (42.4 percent), anemia (40.0 percent), constipation (38.2 percent) and diarrhea (38.2 percent)", so how is this any better than chemo for early stage patients?
Since I'm HER2+ I pay close attention to HER2+ trials and do a lot of research to see what the media doesn't talk about (thank you Vinay Prasad for teaching me how deceptive these media releases for "ground-breaking miracle drugs" can be). With a $7 billion investment riding on this drug I guess it's easy for them to try to convince people that a rate of 50+% Grade 3 and higher AEs is acceptable so they can fast track drug approval, but as someone who is Stage IV and acutely aware of the Quality of Life vs Quantity of Life spectrum and as someone who has already experienced a Grade 3/4 AE that made me wish I was dead, it's not a risk I'd be willing to take in exchange for the possibility of a few extra months of life. It just blows my mind that this is considered an acceptable level of toxicity; I've seen several research oncologists say that a rate of Grade 3 and higher above 10% should be unacceptable and this drug is more than 5x that. It's bad enough that Stage IV patients will be tempted to try something this toxic, but I can't even wrap my mind around the fact that people are talking about possibly using DS-8201 for early stage patients instead of chemo.
I'll be watching the Phase III DESTINY trials closely, but after reviewing the Phase I and Phase II data, I do not share in the excitement about this drug.
-
LBBC has posted a page of links to some highlights on presentations made at the American Society of Clinical Oncology annual meeting. You can access those here: https://www.lbbc.org/news-opinion/updates-2019-asco
-
LoriCA, thanks for summarizing and putting in perspective the results from the DS-8201 studies. I also have been following the development of that drug but I hadn't seen the adverse effects numbers that you shared. Do you have a link to the full report on results that you could share? I've had trouble finding anything but the glowing press reports on its efficacy. Thanks!
Margi -
Margi a lot of the info was shared directly by the drug company itself, Daiichi Sankyo, in their press releases. The media just seems to gloss over it, maybe because it's always near the bottom of the article. The numbers cited in this press release are the updated Phase I results, it mentions the 50% Grade 3 and higher AEs -
https://www.daiichisankyo.com/media_investors/media_relations/press_releases/detail/006943.html
From Targeted Oncology May 2019 (Phase II) - "Fifty percent of patients experienced a grade ≥3 AE and 19% had a serious AE; this included 2 earlier reported cases of grade 5 treatment-related pneumonitis. Additionally, reported cases of interstitial lung disease or pneumonitis in the clinical development program for this agent are evaluated by an independent adjudication committee. A formal monitoring and management program is also in place to help determine the risk of these toxicities." https://www.targetedonc.com/news/fam-trastuzumab-deruxtecan-demonstrates-encouraging-responses-in-advanced-her2-breast-cancer
This article in Oncozine discussing the results for colorectal cancers says there were five Grade 5 (death) cases of ILD attributable to the drug - https://oncozine.com/encouraging-results-for-fam-trastuzumab-deruxtecan-in-her2-expressing-advanced-colorectal-cancer/
So I originally said there were two deaths attributable to the drug and it looks like that number is now 5.
After they released the Phase II trial results I started doing some digging, found the early published Phase I results (not the "updated" results cited above) and some interesting articles posted in other countries that don't have the same marketing spin we often see in the US. Since the first trials including several different types of cancer including breast, gastric, and colorectal, you sometimes have to dig to find the sub-group analyses. Anyway, the links I posted should be a good start for you to get an idea of the safety profile of the drug.
Lori
-
Mountain Mia here’s your answer.
http://www.bbc.com/future/story/20190121-what-we-do-and-dont-know-about-gut-health
-
Breast Cancer Subtypes Among Eastern-African–Born Black Women and Other Black Women in the United States
Although triple-negative breast cancer disproportionately affects black women in the U.S., the risk varies according to where they were born.
CONCLUSIONS: The prevalence of triple-negative breast cancer among black women in the United States varied significantly by birthplace, particularly among Eastern-African–born black women. These findings underscore the importance of considering geographic origin in studies characterizing breast cancer among women of African descent in the United States and elsewhere.
Cancer 2019;0:1-11.
DOI: 10.1002/cncr.32293
-
Novel Treatment Turns Tumors Into 'Cancer Vaccine Factories'
In-situ vaccine may enhance immunotherapy response in resistant cancers, study shows
A novel approach to cancer immunotherapy injects immune stimulants directly into a tumor to "teach," induce the immune system to destroy the cancer and other tumor cells throughout the body. The three-step approach works as an in-situ cancer vaccine, researchers said.
A preliminary study could point to a new way of making immunotherapy more effective in cancers that have proven to be resistant to treatment and also enhance the effects of checkpoint blockade.
A clinical trial for lymphoma, breast, and head and neck cancer patients opened in March 2019 to test the vaccine with checkpoint blockade. The in-situ vaccine is also being tested in the laboratory in liver and ovarian cancers.
-
Clinical Challenges: Avoiding Chemotherapy in Breast Ca
The associated toxicity has breast cancer researchers investigating non-chemotherapeutic approaches
{This article starts out with a discussion of the TAILORx study which studied avoiding chemotherapy in patients with estrogen receptor (ER)-positive, HER2-negative, lymph node-negative breast cancer. It goes on to discuss a less reported study on the possibility of treating HER2+ BC without chemotherapy.}
A recent study adds another potential method of identifying patients who can benefit from certain treatments, while avoiding chemotherapy. Researchers from Johns Hopkins Kimmel Cancer Center in Baltimore identified a positron emission tomography (PET) scan biomarker that may be able to identify patients with human epidermal growth factor receptor 2 (HER2)–positive breast cancer who might benefit from targeted therapy alone, without chemotherapy.
Study CONCLUSION: Early changes in SULmax predict response to four cycles of PT in estrogen receptor–negative, HER2-positive breast cancer. Once optimized, this quantitative imaging strategy may facilitate a more tailored approach to therapy in this setting.
https://ascopubs.org/doi/abs/10.1200/JCO.2018.78.7986?journalCode=jco
DOI: 10.1200/JCO.2018.78.7986 Journal of Clinical Oncology 37, no. 9 (March 20 2019) 714-722.
-
Cannabinoids in Oncology: A Growing Role
Mellar Davis, MD, on the pros and cons, benefits of cannabis in cancer patients
{Interesting video, + transcription, op-ed on cannabis in palliation. Discussion of history of medicinal use in the U.S., challenges related to dosing and risk for drug interactions.}
-
The Arc of Therapy: From Cure to Humbling Legacy
{This is not research, but is a very insightful reflection on the experience of long term survivorship. The physician-author has a history of Hodgkin lymphoma, radiation therapy, breast cancer, a thyroid nodule, and lung cancer. It acknowledges the uncertainty of living with long term survivorship in ways that may speak to others similarly situated.}
https://ascopubs.org/doi/full/10.1200/JCO.19.00666
In a similar vein, here is a commentary on the frustration physicians experience as a result of "not having a crystal ball."
https://connection.asco.org/blogs/modern-day-cassandras-reflections-asco19
-
ASCO 2019: SOPHIA Trial Shows Promise for Margetuximab in HER2-Positive Breast Cancer
This is the first trial to use CD16A genotype as a predictor of response
The HER2-targeted antibody margetuximab was associated with better progression-free survival (PFS) rates than trastuzumab for the treatment of HER-2 positive breast cancer, particularly among carriers of the low-affinity CD16A-158F allele, in the SOPHIA trial, presented here at the Annual Meeting of the American Society of Clinical Oncology, which took place from May 31 to June 4.
The primary endpoints of the trial were central blinded PFS and overall survival (OS), assessed sequentially. Objective response rate (ORR) was a secondary endpoint.
Among 524 patients with baseline measurable disease, the ORR was higher with margetuximab versus trastuzumab.
Safety profiles were comparable in 529 patients who received study therapy.
"This is the first prospective analysis of a CD16A genotype as a predictor of efficacy from anti-HER2 therapy. said Dr. Rugo, "and we demonstrated that an enhanced PFS benefit with margetuximab in patients carrying the low-affinity CD16A-158F allele."
Interim survival analyses did not yield significant differences between the two treatment groups. A second interim OS analysis will be available late in 2019.
https://www.practiceupdate.com/C/85100/56?elsca1=emc_enews_topic-alert
-
Pyrotinib Plus Capecitabine for HER2+ Metastatic Breast Cancer
- Interview with Lee S. Schwartzberg MD, FACP Interview by Farzanna S Haffizulla MD, FACP, FAMWA
- one of the key studies presented this year looks at the novel compound pyrotinib for HER2+ breast cancer.
- Double-blinded, double randomized controlled study in patients who were HER2+, metastatic breast cancer, had previously been exposed to taxane and trastuzumab, and the results of the study showed that the progression-free survival, the primary endpoint was more than doubled, to about 11 months, from four months, with the addition of pyrotinib. That was quite good, and has a ratio of less than 0.2, so more than 80% improvement overall, highly statistically significant, and that was a very positive result, I think, we can say.
- Not a very large study, under 300 patients, so by phase III standards it was somewhat small, but the results are very strong
- Pyrotinib, like other ERBB inhibitors, tend to have diarrhea as a common side effect, and that was also seen here as the most common toxicity, and of course capecitabine, of course, is hand-foot syndrome, which was the other common toxicity here.
- ... this will be, potentially, the third small molecule TKI that would come to market, potentially. What we don't know, though is the relative benefit of one versus the other{s}. ...where does pyrotinib fit? I don't think we know ....It has attractive biochemical properties and it could potentially find a place in the armamentarium of HER2 therapy.
- https://www.practiceupdate.com/C/84876/56?elsca1=emc_enews_topic-alert
-
Lori, thanks for the follow-up information on the DS-8201 study results.
And Lumpie, thanks so much for all the interesting information that you post.
This is really helpful!
Margi
-
Three Cheers for Lumpie!!
-
!Hip hip hooray!
-
NIH Leader Shuns All-Male Panels. Many Applaud the Gesture, but Not All.
Francis Collins won't participate in those so-called manels anymore. Many scientists see that as a constructive move toward inclusiveness, but a critic calls the stance unscientific political theater.
https://www.chronicle.com/article/NIH-Leader-Shuns...
{Requires subscription. I will see if I can find a free report on same subject matter.}
-
The NIH director is tired of all-male panels at scientific conventions. So he's doing something about it
https://www.cnn.com/2019/06/13/us/nih-director-male-panels-trnd/index.html
N.I.H. Head Calls for End to All-Male Panels of Scientists
Francis Collins pledged to decline to speak at conferences that do not include enough women in prominent speaking roles.
https://www.nytimes.com/2019/06/12/health/collins-male-science-panels.html
{NYT generally allows a limited number of free accesses per month.}
-
Shame on the FDA, is there any agency we can trust?
Published 12 hours ago
Breast implants linked to rare form of cancer, but FDA declines to ban
https://www.foxnews.com/health/breast-implants-lin... -
I have thought about this many times and want to get feedback from thread followers: much of what is posted here is research news. But some things that I post fall more into the category of healthcare related news. Does it go here or should we have a separate thread? Thanks for sharing your thoughts. And also for your consistent, generous encouragement.
-
Clinical Challenges: Lymphedema in Breast Cancer
Risks have been reduced, but condition remains problematic
Article discusses standards of care, "prehabilitation" -- that is, maximizing patients' physical functioning prior to treatment; efforts toward education "about the procedure they are undergoing, as well as lymphedema risk reduction principles"; non-treatment risk factors; diagnosed and treated in a timely manner. "And that's important because chronic lymphedema is thought to be a condition that can be irreversible and lead to quality of life altering changes like infections and hospitalization, and other morbidities."
There are links to "results of an interim analysis of the PREVENT trial, a randomized trial evaluating bioimpedance spectroscopy versus tape measurement in the prevention of lymphedema following treatment for breast cancer."
-
Lumpie - in response to your question, I would not like a separate thread. I think the research news & health care news you post here are both appropriate. I like that there is a place to come get information without lots of discussion about personal issues.
-
This is a great thread. No need to separate the issues. Please continue as is. I am very grateful that you take the time.
-
Lumpie, regarding the thread, please Keep On Doin’ Whatcher Doin’
-
Lumpie- i agree, keep together.Thank you
-
YIP... keep this tread going Lumpie
-
agree, together is better
-
Moi aussi. General health news/research is interesting to all of us.
-
thank you lumpie
-
Lumpie
Thanks for posting he two articles.
Between the Stanford oncologist suggesting that giving false hope by suggesting treatment for recurrent breast cancer is like treating a chronic disease, and now this doc who is sort of saying the same thing when accessing past performance for survival prediction is like looking into a crystal ball.
Being recently diagnosed where are we really in predicting our future? Do we have a “day by day promise", “month to month luck" or just a plain “crap shoot" for survival with one median outcome for success - you and how you handle all these drugs?
Both oncologist seem to be saying past stats are like leaves blowing in the wind hard to know what tree they came from, hard to know where they will land with central tendency of no value. May be opinion - but very discouraging read.
My MO subscribes to a long survival cure-who to believe-a question now in my mind.
-
Hi Lumpie,
Love this thread, and come here often to catch up with what is new in research and healthcare. I think that is what makes it different to other threads - it is News rather than specific topic content. I have noticed that if you think content is relevant to other threads, you will post it there too.
I hope you keep the two together and share your discoveries with us here.
Cheers,
Jackie
-
I like it all in one place Lumpie, plus there is no other place to post related healthcare news. And when BCO posts a study we are not allowed to discuss it at their threads. I like that we can make comment here. You know as long as we don’t start talking about puppies and tights
-
I vote to have one common thread too but if puppies somehow landed here on occasion, I wouldn’t mind 😀🐶
-
Lumpie I vote to continue the thread as you have been doing it. It is so informative and I thank you so much for all your efforts!
Illimae once again you made me crack up!
-
YIP Lumpie.. you rock with this and we very much appreciate it
-
Thanks SO much, everyone, for your input. Everyone seems to be in favor of keeping things in one place - which sounds good to me. I have a couple of additions to post. Thanks again!!!
-
The Worst Patients in the World
Americans are hypochondriacs, yet we skip our checkups. We demand drugs we don't need, and fail to take the ones we do. No wonder the U.S. leads the world in health spending.
{Present company excepted, I am sure! But it's an interesting perspective.}
-
Never Say 'Die': Why So Many Doctors Won't Break Bad News
After nearly 40 years as an internist, Dr. Ron Naito knew what the sky-high results of his blood test meant. And it wasn't good.
But when he turned to his doctors last summer to confirm the dire diagnosis — stage 4 pancreatic cancer — he learned the news in a way no patient should.
The botched delivery of his grim diagnosis left Naito determined to share one final lesson with future physicians: Be careful how you tell patients they're dying.
https://khn.org/news/never-say-die-why-so-many-doctors-wont-break-bad-news/
This story also picked up/reported by NBC:
https://www.nbcnews.com/health/health-news/never-say-die-why-so-many-doctors-won-t-break-n1016876
{"Bless their hearts"... my doctors take turns giving me bad news. I know it's not fun... and I know that they don't have crystal balls. But as a patient, I need a raod map, even we don't know how fast we're going.}
-
ASCO 2019: KRISTINE Suggests Role for Chemotherapy-Sparing Regimen in HER2-Positive Breast Cancer
Combining trastuzumab-emtansine (T-DM1) with pertuzumab may be an effective chemotherapy-sparing regimen for some women with operable HER2-positive breast cancer, but identifying which women are good candidates for this approach and which would fare better with chemotherapy remains a challenge, according to the results of the KRISTINE trial presented here at the Annual Meeting of the American Society of Clinical Oncology, which took place from May 31 to June 4 (2019).
https://www.practiceupdate.com/C/85097/56?elsca1=emc_enews_topic-alert
---------------------------------------------------
Neoadjuvant Trastuzumab and Pertuzumab Plus Chemotherapy Versus T-DM1 and Pertuzumab in HER2+ Breast Cancer
- Interview with Lee S. Schwartzberg MD, FACP Interview by Farzanna S Haffizulla MD, FACP, FAMW
- https://www.practiceupdate.com/C/84837/56?elsca1=emc_enews_topic-alert
- {includes video}
-
Neoadjuvant Trastuzumab Emtansine and Pertuzumab in HER2–Positive Breast Cancer
- Journal of Clinical Oncology PURPOSEThe KRISTINE study compared neoadjuvant trastuzumab emtansine plus pertuzumab (T-DM1+P) with docetaxel, carboplatin, trastuzumab plus P (TCH+P) for the treatment human epidermal growth factor receptor 2–positive stage II to III breast cancer. T-DM1+P led to a lower pathologic complete response rate (44.4% v55.7%; P = .016), but fewer grade 3 or greater and serious adverse events (AEs). Here, we present 3-year outcomes from KRISTINE.CONCLUSION
Compared with TCH+P, T-DM1+P resulted in a higher risk of an EFS event-free survival events owing to locoregional progression events before surgery, a similar risk of an IDFS event, fewer grade 3 or greater AEs during neoadjuvant treatment, and more AEs leading to treatment discontinuation during adjuvant treatment.
DOI: 10.1200/JCO.19.00882 Journal of Clinical Oncology -
6 Months vs 12 Months of Adjuvant Trastuzumab in Early Breast Cancer
- The Lancet This final report from a phase III trial provides data from patients with HER2-positive early breast cancer who were given 6 months versus 12 months of adjuvant trastuzumab. Therapy with 6 months of trastuzumab was not found to be noninferior to 12 months in this study.This study supports 12 months of trastuzumab as standard of care.
-
Compassion fatigue hits not only professional caregivers. Other people get it, too.
Vicki tried to lighten the load of a friend who was facing a terminal illness. "As she got sicker, I tried to relieve every burden I could imagine," ...She did this while also caring for her parents throughout their illnesses and deaths. ...her contemporaries continue to face dreaded diagnoses, with many needing assistance. Finally, she rightfully asked herself, "How much more could I do without getting even more tired and sad?"
{Article discusses compassion fatigue among caregivers.}
{Washington Post allows a limited number of views per month without subscription.}
-
The Business of Health Care Depends on Exploiting Doctors and Nurses
One resource seems infinite and free: the professionalism of caregivers.
{Opinion piece. A chilling and persuasive account of how the system - the business of healthcare - relies on physicians and nurses being rushed and doing work on uncompensated time - and how electronic medical records and administrative bloat exacerbate this problem.}
"The health care system needs to be restructured to reflect the realities of patient care. From 1975 to 2010, the number of health care administrators increased 3,200 percent. There are now roughly 10 administrators for every doctor..... Counting on nurses and doctors to suck it up because you know they won't walk away from their patients is not just bad strategy. It's bad medicine."
https://www.nytimes.com/2019/06/08/opinion/sunday/hospitals-doctors-nurses-burnout.html
{The New York Times allows a limited number of views per month without subscription.}
-
Success of breast cancer candidate spurs interest in ADCs
The late-stage testing success of the antibody drug conjugate DS-8201 for breast cancer has spurred increased interest in developing ADCs for what some analysts say could be treatments that replace chemotherapy. Some 56 drug companies are working on ADC candidates, and the ADC market is expected to hit nearly $10 billion by 2025.The Economic Times (India)/Bloomberg (6/14)
{I think that there was discussion above about ES's with this therapy. I think that this is actually the same article referenced in one of the posts above.}
-
Ultrasound, laser device detects and destroys circulating cancer cells
University of Arkansas for Medical Sciences researchers developed a device that uses ultrasound to detect circulating cancer cells and a laser to destroy the cells. An ultrasound transducer applied to the skin surface is able to detect sounds emitted by the cancer cells as they are heated by the laser, which then further heats them to kill them, the researchers report in Science Translational Medicine.New Atlas (6/17)
https://newatlas.com/cancer-cells-laser-ultrasound-detection-and-treatment/60158/
-
CMS drafts rule to improve e-prescribing, prior authorizations
The CMS released a proposed rule that would update the electronic prescribing standards and prior authorization process for Medicare Part D. The proposed changes "would reduce the time it takes for a patient to receive needed medications and ease the prescriber burden by giving clinicians the flexibility and choice to complete prior authorization transactions electronically," CMS Administrator Seema Verma said.Becker's Hospital Review (6/17),Health Data Management (free registration) (6/17)
-
Cancer indicator may also predict diabetes risk
Research links epidermal growth factor receptor to diabetes risk
A study in Diabetes Care showed that adults with the highest circulating levels of the epidermal growth factor receptor HER2/ErbB2 were at a higher risk for diabetes than those with the lowest levels. Swedish researchers used a cohort of 4,220 participants from the Malmo Diet and Cancer-Cardiovascular study and found that each 1-standard deviation increase in ErbB2 levels was tied to an increased diabetes risk in both men and women.Healio (free registration)/Endocrine Today (6/17)
Adults with larger amounts of the epidermal growth factor receptor HER2/ErbB2 are at a higher risk for diabetes compared with those with lower measures, according to findings published in Diabetes Care.
"In addition to breast cancer, circulating ErbB2 levels are positively associated with an increased risk of diabetes," the researchers wrote. "Our results are interesting and worth exploring regarding the potential role of ErbB2 in the development of diabetes and in novel therapeutic approaches."
Diabetes Care. 2019; doi:10.2337/dc18-2556.
-
Guiding Cancer Control: A Path to Transformation webinar
On June 27, 2019, from 1 to 2 pm EDT, the National Academies of Sciences, Engineering, and Medicine will release its new report Guiding Cancer Control: A Path to Transformation in a webinar report release event.
This new report will look at cancer control efforts in the United States and will recommend a new approach to reduce the burden of cancer and improve quality of life for cancer survivors.
Authoring committee members participating in the webinar include:
Michael Johns (Committee Chair), Emory University
Ashleigh Guadagnolo, University of Texas MD Anderson Cancer Center
Joseph Lipscomb, Emory University
Mary McCabe, Weill Cornell Medical College and Columbia University School of Nursing
William Rouse, Stevens Institute of Technologyregister here (free):
{The National Academies of Sciences, Engineering, and Medicine offer numerous publications on cancer and other topics free of charge in PDF format or in print for a fee.}
-
Impact of muscle volume on breast cancer outcomes
Prognostic impact of skeletal muscle volume derived from cross-sectional computed tomography images in breast cancer
This study analysed if the volume of muscle or the volume of fat in a patient with breast cancer had any impact on their survival. The study found that patients with breast cancer who had higher volumes of muscle survived better than patients with low volumes of muscle.
CONCLUSION: This study demonstrated that breast cancer patients with higher skeletal muscle volume showed more favorable prognosis.
https://www.ncbi.nlm.nih.gov/pubmed/30132218
DOI: 10.1007/s10549-018-4915-7 -
High Soy Intake May Cut Fracture Risk in Younger Breast Cancer Survivors
Findings seen among pre-/perimenopausal survivors of stage 0 to III breast cancer
- HealthDay
- Higher soy consumption is linked to fewer osteoporotic fractures in younger breast cancer survivors, according to a study published online May 21 in JNCI Cancer Spectrum.
- https://www.practiceupdate.com/C/85457/56?elsca1=emc_enews_topic-alert
- https://academic.oup.com/jncics/article/3/2/pkz017/5488692
- https://doi.org/10.1093/jncics/pkz017
-
Thank you, Lumpie, for all your work on finding and posting these! That ultrasound device that can destroy CTCs sounds very promising!
My MO is very research oriented, but when I asked her about doing a CTC test, she said: "we know having higher levels of CTC in an early BC patient is associated with higher probability of relapse, but we don't know what to do about this yet". Now there may be a mechanism to destroy the CTCs!
-
FarAwayToo: Ditto - my MO said the same thing: Even if we figure out that you have a high level of CTC's, we don't know what to do about it. That is not very comforting to patients. I am optimistic that, with further research, some version of CTC's will be used as a diagnostic tool and will become actionable.
-
Rate of breast implant removal surgeries rising
The number of women having breast implants removed has increased almost 40% over the past decade, and they report an array of symptoms they say are linked to the implants, including headaches, fever, brain fog, rashes, chronic fatigue and joint pain. Dr. Dave Rankin of Aqua Plastic Surgery in Jupiter, Fla., said he performed at least 400 explant procedures in 2018 and he sees demand for explant surgeries outpacing demand for implants.WFTS-TV (Tampa, Fla.) (6/17)
-
Make palliative care automatic for breast cancer, expert says
Palliative care should be "automatic, expected and a routine part of excellent breast cancer care," said Dr. Michael Rabow, a palliative care medical director at the University of California at San Francisco's Helen Diller Family Comprehensive Cancer Center. Progress has been made for patients with metastatic breast cancer, but palliative care remains underutilized overall. Medscape (free registration) (6/14)
https://www.medscape.com/viewarticle/913957
-
New models may address cancer survivors' care coordination headaches
Because their medical histories are lengthy and complex, cancer survivors in particular struggle with poorly coordinated care that can compromise access to needed follow-up, writes Michelle Doose, an epidemiology researcher and cancer survivor. However, patient-centered medical homes, accountable care organizations and other emerging frameworks show promise for ensuring cancer survivors get well coordinated care that could also become a model for other patients. Scientific American (tiered subscription model) (6/2019)
https://blogs.scientificamerican.com/observations/cancer-survivors-deserve-coordinated-care/
-
Lawmakers introduce data privacy proposal
The Protecting Personal Health Data Act, proposed by Sens. Lisa Murkowski, R-Alaska, and Amy Klobuchar, D-Minn., aims to create data protection standards and regulation not currently covered by HIPAA, including those from technologies such as health apps. The proposal would require HHS to create a national task force to protect health data and develop security standards for apps, consumer devices, software and services, and establish regulations to help enhance health data security and privacy. Health IT Security (6/17)
https://healthitsecurity.com/news/proposed-bill-would-close-hipaa-gaps-curb-health-app-privacy-risks
-
Life And Debt: Two Health Professionals. Two Hurricanes. Two Heart Surgeries.
A physician married to a psychologist got very sick. As expenses mount, these providers are experiencing the woes of American health care from the other side.
https://www.huffpost.com/entry/life-and-debt-doctors-hurricanes-surgeries_n_5cee9494e4b0975ccf5ea272
{Financial and social toxicity of a medical crisis. Most of us can relate.}
-
Traumatic injuries linked to later social dysfunction
(Reuters Health) - Nearly half of trauma patients, even those without brain injuries, experience social deficits that make it harder for them to interact with friends and stay involved in the community, a recent study suggests.
{This article reports on trauma patients but I believe that there are some studies out about the traumatic effects of a cancer diagnosis and the burdensome consequences of dealing with the whole process. Some may find this topic interesting, relevant.}
-
-
Metformin, 1p diabetes pill, is new weapon against breast cancer
'A diabetes drug that costs as little as 1p a tablet can curb the growth of breast cancer by up to 76%, experts have found.
Scientists discovered that metformin, taken by millions of diabetes patients, dramatically alters the make-up of breast cancer stem cells by forcing them to become addicted to glucose.
This creates a treatment "sweet spot", enabling cancer drugs to target and kill the stem cells.
The Southampton University team found that treating breast cancer with a low dose of metformin before attacking it with cancer drugs called CtBP inhibitors produced a reduction of up to 76% in the growth of the disease.In results published in the journal Carcinogenesis, researchers showed that an eight-week programme of low-dose metformin, commonly used to treat type 2 diabetes, altered the metabolism of breast cancer stem cells.
Normally, the cells rely on both oxygen and glucose for the energy they need to grow and survive. But breast cancer stem cells are incredibly resilient, and can alter how they produce their energy depending on their surroundings.
To survive the metformin treatment, the stem cells switched their metabolism to become more reliant on glucose, which creates a new treatment "sweet spot".
r Jeremy Blaydes, a reader in cancer cell biology at Southampton University and the lead author of the report, said: "Our work has given us the first glimpse into how changes in metabolism can alter the behaviour of breast cancer stem cells and reveal new targets for therapy. "We hope these could lead to new treatment options for breast cancer patients who most need it."
The laboratory findings will allow combinations of metformin and CtBP inhibitors to be trialed in patients.
Baroness Morgan of Drefelin, chief executive of Breast Cancer Now, which funded the research, said: "While it's often brand new drugs that make the headlines, the repurposing of drugs used in other health conditions to develop new cancer therapies, or improve existing ones, is a really exciting research avenue."
The method could help all breast cancer patients, but experts say it could be particularly useful in halting the spread of triple negative breast cancers. -
If anyone has an answer to this it would clear things up for me. Why do cancer cells switch to getting their energy from glucose when Metformin is taken? Is it because the insulin is lowered so there is a switch to glucose? Kind of confused about the mechanism...
-
I'm not sure completely, but I did find this:
Cancer cells need a lot of energy to grow and spread as fast as they do. However, an obstacle in the way of cancer's metabolic needs is a molecule called NAD+. This molecule turns nutrients into energy.
 Cancer cells' use of sugar holds the key to their destruction
Cancer cells' use of sugar holds the key to their destructionRestricting cancer cells' glucose supply and interfering with their ability to metabolize it could help destroy them.
"In order to keep the energy-generating machinery running, NAD+ must be continuously generated from NADH," Benjamin explains, adding,"[B]oth metformin and syrosingopine prevent the regeneration of NAD+, but in two different ways."
Many cancer cells rely on glycolysis in their metabolism, which means that they break sugar down into lactate. When there is too much lactate, however, glycolytic pathways are blocked.
So, to avoid this, cancer cells dispose of lactate via special transporters, and this is where the drug combination comes in.
"We have now discovered," Benjamin points out, "that syrosingopine efficiently blocks the two most important lactate transporters and thus, inhibits lactate export. High intracellular lactate concentrations, in turn, prevent NADH from being recycled into NAD+."
Metformin, meanwhile, blocks the second of the two cellular pathways that help NAD+ regenerate. So, when metformin is combined with syrosingopine, NADH can no longer be recycled into NAD+. This, in turn, creates an energy shortage.
The energy shortage ultimately leads to the death of cancer cells, which no longer have an energy supply. The combination of the two drugs, therefore, "may prove a viable anticancer strategy," conclude the researchers.
-
And this:
In living cells, glucose plays a major role to energy metabolism, taken up by specific glucose transporters (GLUT). Once inside the cell, it is converted to pyruvate through the glycolytic pathway generating a small amount of energy in the form of adenosine triphosphate (ATP). Pyruvate is then transported into the mitochondria, enters the tricarboxylic acid cycle and is oxidized through in the mitochondria respiratory chain (oxidative phosphorylation system [OXPHOS]), generating ATP. This aerobic process is a major source of energy supporting life. Mitochondria are frequently dysfunctional in type 2 diabetes, but most of the ATP in patients with type 2 diabetes is generated through OXPHOS.
Cancer cells, meanwhile, tend to synthesize more ATP through glycolysis than normal cells do. This metabolic shift to aerobic glycolysis is a hallmark of cancer, and is applied to a common clinical test for it, positron emission tomography. Recent studies have suggested that this metabolic shift could be to facilitate the uptake and incorporation of more nutrients into cell building blocks, such as nucleotides, amino acids and lipids, which are required for highly proliferating cells. Mitochondrial dysfunction in cancer cells might be behind this phenomenon, which is well appreciated after Otto Warburg proposed it could be the primary cause3. All in all, the mechanisms underlying the dysregulated cellular metabolism of cancer cells remain poorly understood. Whatever the mechanisms are, blocking these metabolic alterations is now emerging as a new therapeutic approach of cancer, and as such, some of the metabolic enzymes involved in the glycolytic pathway are currently considered as therapeutic targets. Glucose deprivation is currently considered as one of such therapeutic options.
Very recently, Madiraju et al.7 reported that metformin inhibits mitochondrial glycerophosphate dehydrogenase (mitoGPD), and thus alters the mitochondrial and cytosolic redox state, and reduces reactive oxygen species production. It is not clear how metformin inhibits complex 1 and mitoGPD or if the two mechanisms are interrelated. We are fully aware that there are other possible mechanisms for the anticancer effect of metformin, including stimulation of adenosine monophosphate-activated protein kinase (AMPK) and its upstream regulator, liver kinase B1 (LKB1), although they could well be secondary to its inhibitory effect on the mitochondrial function and the reduction of free radicals through inhibition of mitoGPD, as suggested by Madiraju et al.7
-
Thanks so much! Still not clear but interesting nonetheless!
-
I have been n metformin 1000 mg (2 x 500) since diagnosis as I had seen other articles showing reduced recurrences among women on the drug. I asked my MO and he prescribed it.
It seemed low risk and high potential benefit.
There are anti pinworm and anti tapeworm drugs which seem to target stem cells as well...
-
Pain patients left in anguish by doctors 'terrified' of opioid addiction, despite CDC change
Ken Alltucker and Jayne O'Donnell, USA TODAYPublished 3:54 p.m. ET June 24, 2019 | Updated 4:33 p.m. ET June 24, 2019
https://www.usatoday.com/story/news/health/2019/06... -
Cannabinoids: Preclinical hope for breast cancer therapy
This review concluded that cannabinoids have been shown to inhibit tumor cell growth, cancer spread and blood vessel formation in multiple trials involving animal models and cell cultures. Clinical trials investigating the potential benefits of cannabinoids on the outcomes of breast cancer patients are warranted.
Overall, cannabinoids have been shown to block cancer cell proliferation and reduce cancer cell migration in all breast cancer subtypes.
THC (tetrahydrocannabinol), the most commonly investigated cannabinoid, has been found to reduce both the rate of tumor growth and the overall number of developing tumors in HER2-positive breast cancer through the reduction of cell proliferation and by increasing cancer-cell death. Some studies have also shown cannabinoids to decrease the formation of blood vessels within the tumor, which inhibits cancer growth.
https://www.cancertreatmentreviews.com/article/S0305-7372%2812%2900139-9/abstract
DOI: https://doi.org/10.1016/j.ctrv.2012.06.005
{This article is old - 2012 - but the topic was kind of interesting. There is a charge to access the full journal at this website.}
-
VD3 mitigates breast cancer aggressiveness by targeting V-H+-ATPase
Author links open overlay panelhttps://www.sciencedirect.com/science/article/pii/...
Lumpie, please let me know if I duplicate anything, that’s what happened to me yesterday
-
Salinomycin is an antiparasitic drug.
Salinomycin inhibits breast cancer progression via targeting HIF-1α/VEGF mediated tumor angiogenesis in vitro and in vivo
Author links open overlay panelJayantDewanganaSonalSrivastavaaSakshiMishraaAmanDiva
https://www.sciencedirect.com/science/article/abs/... -
Trump's Plan To Lower Your Hospital Costs: Here's What You Need To Know
President Trump signed an executive order Monday (6/24/2019) that he says would make such comparisons easier, and make the pricing process more transparent.The order directs agencies to draw up rules requiring hospitals and insurers to make public more information on the prices they hammer out in contract negotiations. Also, hospitals and insurers would have to give estimates on out-of-pocket costs to patients before they go in for nonemergency medical care. But just how useful the effort will prove for consumers remains unclear. If the executive order leads to finalized HHS rules, proponents say it could encourage competition and lower prices. Other health care analysts say much depends on how the administration writes the rules over the next several months — rules that govern what information must be provided and in what format. Trump's executive order already is running into opposition from some hospitals and insurers who say disclosing negotiated rates could drive up costs.
Interesting Q&A follows the introduction.
-
Interesting article about hospital pricing. It is all smoke and mirrors. Hospitals price things with magic words and insurance companies adjust the prices with different magic words. And poof! there is the amount you still owe.
Comparing prices on healthcare for individual services also is an interesting idea. It assumes that we buy our healthcare one illness or surgery at a time -- or perhaps it assumes we SHOULD buy it that way. Which is ridiculous, because we are whole people and should have our health considered as a whole bodily and mental being, and not as bits and pieces to be returned to the factory for a tune-up, one at a time.
Another assumption is that people actually CAN comparison shop, or that it is a good idea to shop on price. I have 2 hospitals in my town that provide cancer care. One is in the top 20 on the country for cancer care, and the other is not even on the list. Which one should I go to? Should I make that decision based on the cost of care or on the expertise?
And what about the people who have no cancer center close to them? Or hospital that is qualified to do knee replacement? What competition is there for their business? They will go to whatever hospital they can manage in their lives, even if it's a 90 minute drive each way. Rural American lives this way.
In the meantime, today I got a letter from the insurance company saying my base rate is going up another 12.6% for next year. Year after year I have double digit increases in rate. And still, ridiculously, every day I am grateful I have health insurance, that somehow the republicans have not managed to pry out of my hands yet. Because this year's care for me will likely exceed $150,000. And I hit my out-of-pocket maximum for the year months ago.
Sorry for the rant. I know that's not really the point of this thread. Just call me skeptical that new rules or executive order will actually improve healthcare in the US.
-
Senate Committee OKs Act to End Surprise Billing
Core focus of the "Lower Health Care Costs Act" is price transparency
A bipartisan bill focused on eliminating surprise medical bills and lowering patients' out-of-pocket costs passed out of the Senate Health, Education, Labor and Pensions Committee in a 20-3 vote on Wednesday.
A core focus of the "Lower Health Care Costs Act" is price transparency, said Committee Chairman Lamar Alexander (R-Tenn.).
....he, along with ranking committee member Patty Murray (D-Wash.), agreed that the best solution is to pay out-0f-network doctors in hospitals the median contract rate that in-network doctors are paid for those same services in a particular geographic area -- a strategy dubbed "the benchmark solution."
While Alexander noted that the benchmark solution was deemed the most effective approach to lowering healthcare costs by the Congressional Budget Office, he said he was open to continue working on the bill to see if it could be improved.
Alexander outlined other measures included in the current bill:
- Mandating that healthcare facilities offer a summary of services after discharge, and requiring that hospitals send all medical bills within 45 days
- Directing doctors and insurers to give patients price quotes on their expected out-of-pocket costs for care
- Helping to bring biosimilars to market faster by leveraging a "transparent, modernized and searchable" patent database
- Keeping the FDA drug patent database system up to date in order to accelerate generic product development
- Banning the abuse of "citizen petitions" which can "unnecessarily delay drug approvals"
- Closing a loophole that enables drug companies to retain exclusivity and prevent less expensive drugs from coming to market by making insignificant tweaks to old drugs
The bill would also increase prescription drug competition by eliminating "gag clauses" in insurance contracts, and by banning pharmacy benefit managers from charging more for a drug than they paid for it,it would target several public health challenges, such as supporting state and local efforts to raise vaccination rates, efforts to prevent and curb obesity, and expanding healthcare technology to better serve rural communities, as well as enforce mental health parity laws.
The bill would also expand mandatory funding for community health centers and four additional programs "to ensure that 27 million Americans who rely on these centers for primary care and other healthcare can continue to access centers close to home,"
...amendment to the bill ...also wrapped in two other measures; one that would raise the minimum age for purchasing any tobacco product to 21 from 18, and another that would ban anti-competitive practices in generic drug development such as sample-blocking.
An amendment to require insurance companies to post information regarding network adequacy, based on the insurers last interaction with a provider, was also approved by the committee, along with the FAIR Drug Pricing Act, an amendment that calls for transparency from pharmaceutical companies that plan to raise prices of their products.
Alexander said he aims to hold a floor vote on the bill before the end of July.
-
MountainMia: yes. There are so many problems.... outrageous out of pockets, even with "good" insurance...access to facilities, especially for those in rural areas....the fact that, for many of us, our health insurance is wrapped up with our jobs, so if we lose our jobs, we lose our insurance. Not to mention that, if lifetime limits come back, many of us are proverbial toast. Lots of issues that need to be addressed.
-
Banned Antibacterial Tied to Osteoporosis—
Associations strongest in postmenopausal women
The antibacterial chemical triclosan was tied to deleterious bone changes in women, according to researchers in China.
In an analysis of over 1,800 adult women, high exposure to triclosan was associated with a nearly 2.5-fold increased chance of developing intertrochanteric osteoporosis...
An endocrine-disrupting chemical (EDC), triclosan is a chemical with antibacterial properties that was commonly used in household items such as soap, mouthwash, and hand sanitizers. Along with a slew of similar chemicals, the FDA banned triclosan from being used in over-the-counter soaps in 2016 and hand sanitizers in April 2019. Despite the current ban, the chemical may still be found in other daily products not regulated by the FDA, such as clothing (athletic wear) and contaminated water.
the authors reported that women who fell into the highest tertile of triclosan exposure also had significantly lower bone mineral densities (BMDs) compared with women in the lowest exposure group...
When the analysis was restricted only to premenopausal women, there were no associations between any degree of triclosan exposure with BMD in any area of the body.
Primary Source
The Journal of Clinical Endocrinology & Metabolism
-
SHARE Report Back from ASCO on Metastatic Breast Cancer
Webinar
Dr. Linda Vahdat, medical oncologist at Memorial Sloan Kettering Cancer Center and Chief of Medical Oncology and Clinical Director of Cancer Services at Norwalk Hospital, will summarize research presented at ASCO 2019 focusing on metastatic breast cancer. Dr. Vahdat will also discuss her current research in triple negative metastatic breast cancer.
{This webinar was presented 6/25/2019. If you register, the recording opens up.}
-
This website has a calendar of events that you may be interested in. It includes webinars! https://thestormriders.org/ Some conferences do live streaming.
I’ve put some webinars on my calendar and will be attending the breast cancer conference in Seattle in September. Lots of interesting stuff!
-
Scientists discover 'switch' that helps breast cancer spread around the body
-
Researchers Turn On PTEN Tumor-Suppressor Protein in Cancer Cells
-
-
Rate of Memory Change Before and After Cancer Diagnosis
Question Are factors associated with carcinogenesis associated with a slower decline in memory function before and after cancer diagnosis in middle-aged and older US adults?
Findings In this population-based cohort study of 14 583 individuals, those with an incident cancer had modestly higher memory function and slower memory decline both before and after their diagnosis than similarly aged individuals who remained cancer free for a mean 11.5-year follow-up.
Conclusions and Relevance In this study, older individuals who developed cancer had better memory and slower memory decline than did similarly aged individuals who remained cancer free. These findings support the possibility of a common pathologic process working in opposite directions in cancer and Alzheimer disease.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2736177
JAMA Netw Open. 2019;2(6):e196160. doi:10.1001/jamanetworkopen.2019.6160
-
Hematologic Safety Analysis of Palbociclib With Letrozole in Postmenopausal Women With ER+/HER2− Advanced Breast Cancer
- The Oncologist This analysis of clinical trial data evaluated the hematologic adverse effects of palbociclib associated with the use of letrozole in patients with ER+/HER2− advanced breast cancer. The incidence of grade 3 neutropenia was 55.6%, and 95.3% of patients experienced some neutropenia, which was managed by dose modification. The progression-free survival was similar among those experiencing grade ≥3 neutropenia requiring dose modification and those without grade ≥3 neutropenia.The use of palbociclib with letrozole for women with ER+/HER2− advanced breast cancer is associated with a high incidence of neutropenia, which can be managed by dose modification. This change in dose does not appear to impact efficacy.https://www.practiceupdate.com/C/85638/56?elsca1=emc_enews_topic-alerthttp://theoncologist.alphamedpress.org/content/early/2019/06/06/theoncologist.2019-0019doi:10.1634/theoncologist.2019-0019 Additional commentary on this study: https://www.practiceupdate.com/C/85638/56?elsca1=emc_enews_topic-alert
-
Cancer-related financial burden among patients with metastatic breast cancer.
Presented at ASCO Saturday, September 29, 2018
Background: Recent data suggest that the adverse financial impact of cancer is an underappreciated source of potential harm to patients, also known as "financial toxicity". Little is known about the financial impact of cancer in patients with widespread, incurable disease, despite the relatively high cost of their care. We conducted a national survey of patients with metastatic breast cancer to address this gap.
Conclusions: Metastatic breast cancer patients reported an unprecedented level of cancer-related financial harm and significant worry about the financial legacy left behind in the wake of their illness. Health insurance expansion is a necessary, but insufficient strategy to address this financial burden; additional interventions to prevent and mitigate cancer-related financial harm are urgently needed.
https://meetinglibrary.asco.org/record/166359/abstract
Citation: J Clin Oncol 36, 2018 (suppl 30; abstr 32)
There is a related article/discussion on this presentation/article here:
-
Interesting video montage of newspaper articles regarding breast cancer over the last 100+ years.
"This is a story spanning over a century of headlines for breast cancer and promises for a cure."
https://www.facebook.com/watch/?v=891998281148250
{You may need to be a group member to view the video.... not sure....}
-
I like the video of the bullies.
-
Appreciate the palbo/ Letrozole article Lumpie
-
New Study Shows a Decline in the Incidence of Recurrent Metastatic Breast Cancer Over Time but no Improvement in Survival
New York, NY (February 1, 2019) A retrospective analysis – reported in the journal Breast Cancer Research and Treatment, by Judith Malmgren, PhD, and co-authors – studied 8292 women with stage I-III invasive breast cancer, 964 of whom (11.6%) were later diagnosed with recurrent metastatic breast cancer (rMBC). The authors found a significant decline in rMBC over time, but no increase in distant disease survival. Distant disease survival after an rMBC diagnosis decreased over time, from 23% in the years between 1990 and 1998, to 21% between 1999 and 2004, and to 13% between 2005 and 2011.
https://4fq5um2tr9f1r1ne5s8uo915-wpengine.netdna-ssl.com/wp-content/uploads/press-release-Feb-1-2019.pdfhttps://link.springer.com/article/10.1007/s10549-018-05090-y
DOI https://doi.org/10.1007/s10549-018-05090-y
-
MRI vs Mammography for Breast Cancer Screening in Women With Familial Risk
- The Lancet Oncology This multicenter, randomized trial compared the benefit of MRI versus mammography for breast cancer screening among patients with a familial risk of breast cancer who were BRCA1/2 or TP53 wildtype. MRI screening detected more breast cancers and detected breast cancer at an earlier stage than mammography. Higher breast density was associated with poorer tumor stage and lower specificity in both screening groups.MRI screening appears to detect breast cancer at an earlier stage compared with mammography, and this could potentially improve outcomes. However, MRI may be associated with more false positives, particularly in women with a high breast density.
-
New Study Shows a Decline in the Incidence of Recurrent Metastatic Breast Cancer Over Time but no Improvement in Survival
Would I be interpreting this plausibly to say that the current regimes for preventing progression (hormone blockers, etc) are doing a good job preventing some women who would otherwise have progressed from progressing, but that possibly they are the ones who would not have died from metastasis anyway, and would have brought up the survival stats, and now are not? That is... interesting and disturbing in a way.
-
Mixed Results for Profiling in Predicting Late Recurrence in ER+ Breast Cancer
Tools may, however, help select patients for extended treatment
-
Dueling Views on Genetic Testing in Breast Cancer
Journal correspondence makes cases for, against expanded germline testing
A call for universal genetic testing in women with newly diagnosed breast cancer stirred up strong views on both sides of the issue, which played out in correspondence to a leading oncology journal.
Late last week, JCO published three letters about the study, two from oncologists who disagreed with Beitsch and colleagues and one from a group of cancer specialists who supported the recommendation for universal testing. Additionally, JCO published a response from Beitsch and coauthors.
The disparate views reflected the complexities of interpreting, explaining, and acting on test results.
-
Hi Salamandra: Yes, I think that you interpretation is pretty much correct. They seem to be saying that treatments are pretty good at keeping cancer from coming back (recurrence or metastasis) but that overall survival has not gotten better. I read at least a fair amount of the article and I am trying to recall discussion of causality.... Maybe some of the healthier patients never progressed. I have read elsewhere that therapies for MBC patients are improving quality of life but not extending it (although I can't give you a citation for that off the top of my head). This state of affairs leaves many parties frustrated and puzzled.... not to mention disappointed.
-
Almost Half of Breast Cancer Mutations Missed by Test Criteria
Similar rate of variants in women included, excluded by NCCN guidelines
Women who did not meet guideline criteria for genetic testing in breast cancer had a prevalence of potentially pathogenic mutations similar to that of women who met current testing criteria, data from a multicenter prospective registry showed. The results showed that 9.39% of women who met National Comprehensive Cancer Network (NCCN) testing criteria had pathogenic or likely pathogenic (P/LP) aberrations in their breast tumors. Women who did not qualify for testing by NCCN criteria had a prevalence of 7.9%, which did not differ significantly from the NCCN-qualified group...
https://www.medpagetoday.com/hematologyoncology/breastcancer/78190
https://ascopubs.org/doi/full/10.1200/JCO.18.01631
DOI: 10.1200/JCO.18.01631 Journal of Clinical Oncology 37, no. 6 (February 20 2019) 453-460.
{This relates to the post regarding "dueling views" above.}
-
Analytics, AI begin to show results in oncology
Research using data, analytics and artificial intelligence in oncology is in the early stages, but studies presented at a recent conference show there is real-world progress to report, writes Dr. Nathan Levitan of IBM Watson Health. AI can help physicians manage large amounts of data and facilitate shared decision-making with patients, as well as process clinical trial eligibility criteria and match patients to trials, Levitan writes.
Note: author is Nathan Levitan, M.D. the chief medical officer for IBM Watson Health Oncology and Genomics.
-
Frequency of Pathogenic Germline Variants in CDH1, BRCA2, CHEK2, PALB2, BRCA1, and TP53 in Sporadic Lobular Breast Cancer
Christos Petridis, Iteeka Arora, Vandna Shah, Charlotte L. Moss, Anca Mera, Angela Clifford, Cheryl Gillett, Sarah E. Pinder, Ian Tomlinson, Rebecca Roylance, Michael A. Simpson and Elinor J. SawyerDOI: 10.1158/1055-9965.EPI-18-1102 Published July 2019
Abstract
Background: Invasive lobular breast cancer (ILC) accounts for approximately 15% of invasive breast carcinomas and is commonly associated with lobular carcinoma in situ (LCIS). Both have been shown to have higher familial risks than the more common ductal cancers. However, there are little data on the prevalence of the known high and moderate penetrance breast cancer predisposition genes in ILC. The aim of this study was to assess the frequency of germline variants in CDH1, BRCA2, BRCA1, CHEK2, PALB2, and TP53 in sporadic ILC and LCIS diagnosed in women ages ≤60 years.
Methods: Access Array technology (Fluidigm) was used to amplify all exons of CDH1, BRCA2, BRCA1, TP53, CHEK2, and PALB2 using a custom-made targeted sequencing panel in 1,434 cases of ILC and 368 cases of pure LCIS together with 1,611 controls.
Results: Case–control analysis revealed an excess of pathogenic variants in BRCA2, CHEK2, PALB2, and CDH1 in women with ILC. CHEK2 was the only gene that showed an association with pure LCIS [OR = 9.90; 95% confidence interval (CI), 3.42–28.66, P = 1.4 × 10−5] with a larger effect size seen in LCIS compared with ILC (OR = 4.31; 95% CI, 1.61–11.58, P = 1.7 × 10−3).
Conclusions: Eleven percent of patients with ILC ages ≤40 years carried germline variants in known breast cancer susceptibility genes.
Impact: Women with ILC ages ≤40 years should be offered genetic screening using a panel of genes that includes BRCA2, CHEK2, PALB2, and CDH1.
Footnotes
- Note: Supplementary data for this article are available at Cancer Epidemiology, Biomarkers & Prevention Online (http://cebp.aacrjournals.org/).
- Cancer Epidemiol Biomarkers Prev 2019;28:1162–8
- Received October 9, 2018.
- Revision received December 7, 2018.
- Accepted April 3, 2019.
- Published first July 1, 2019.
- ©2019 American Association for Cancer Research.
-
Lumpie of course my brain went somewhere else when I read “AI.” 😉
-
New name for breast-cancer syndrome could help to save lives
People of all sexes can have risk genes that are often assumed to affect only women. Renaming the syndrome should aid cancer prevention and treatment
Patients do "not realiz{e} that people of all sexes (including transgender people) can have mutations in BRCA1 and BRCA2 genes. These genes do encode the proteins associated with susceptibility to breast cancer. But they are also associated with an increased risk of prostate and pancreatic cancer, among others.
"Because this is not widely understood, testing is not being done for the right people at the right time. Those who identify as men are especially less likely to be tested. And people who are tested can have difficulty understanding the full meaning of their results...
"...hereditary breast and ovarian cancer syndrome, or HBOC. This term is not only misleading, it is also cumbersome and hard to remember. Fortunately, there is a simple solution: rename the syndrome.
"I propose that HBOC be renamed King syndrome. ...it would recognize the seminal contributions of pioneering cancer geneticist Mary-Claire King, the discoverer of BRCA1.
Article by Colin C. Pritchard
https://www.nature.com/articles/d41586-019-02015-7
Nature 571, 27-29 (2019)
doi: 10.1038/d41586-019-02015-7
-
Ingerp: Oh, that's funny! Yes, our minds automatically go to a different AI...except those, perhaps who work in IT. Then, if they have BC, they must constantly pause and change gears!
Happy Independence Day to all!
-
Facebook seeks to limit circulation of debunked medical claims
07/02/19
Facebook on Tuesday announced it is seeking to limit the circulation of debunked medical claims after multiple reports found that bogus cancer cures are rampant on the platform.
"In order to help people get accurate health information and the support they need, it's imperative that we minimize health content that is sensational or misleading," the blog post reads.
The tweaks come on the heels of two reports from The Washington Post and The Wall Street Journal detailing how users can get sucked into rabbit holes of medical misinformation when they're seeking more information about cancer diagnoses.
The Post identified groups dedicated solely to sharing "natural" cures for cancer, which have been shown to be ineffective when pursued without modern medicine.
The Journal's investigation found multiple figures without medical licenses selling bunk cancer "treatments" such as baking soda injections and juice regimens.
At a hearing last week, lawmakers dug into a Facebook representative over the continual presence of anti-vaccine content, saying it amounts to a public health hazard and the company is not taking action quickly enough.
-
Study Probes How to Tell Elderly Patients Not to Bother With Cancer Screening
07/02/2019
...current clinical guidelines recommend against screening many older adults, such as those with less than 10 years' life expectancy. For doctors, talking to a patient about the idea that they've "aged out" of cancer screening can be a challenging conversation.Studies have found that cancer screening in adults with limited life expectancy can present unnecessary risks and lead to unnecessary treatments. That's because the tests may detect slow-growing tumors that aren't likely to affect an older person's lifespan.Patients and clinicians ... agreed that patients should play an active role in making the decision to stop screening. Clinicians tended to worry that patients might perceive the recommendation to stop screening in a negative light and that it would make patients angry. However, patients mostly responded that if they trusted their clinician, they would not think negatively of them for initiating the conversation. -
Why It's Still 1989 for Primary Care
Time and financial pressures keep PCPs from keeping up
- by Milton Packer, MD
- July 03, 2019
{This article provides remarkable insight on the "nuts-and-bolts" challenges associated with providing good quality primary care in today's healthcare - and payment - environment.}
Without doubt, U.S. patients with many chronic illnesses are not receiving good quality medical care to reduce suffering and prolong life.
What happens if a physician tries to make a difference and spends a bit of extra time? Their schedule runs late. When a survey subsequently asks if their appointment started on time, patients say no. And thus, the physician's patient satisfaction scores suffer.
To get real medical attention these days, you need to have an illness that requires or is amenable to a procedure for which the physician is paid. The result: when compared with other countries, we have the most expensive healthcare in the world, but we have worse outcomes.
..finding someone to blame does not fix the problem.
Our healthcare delivery system for chronic illness is horribly ill, even for those with full access to healthcare. Financialization has hollowed out its core mission and has made it meaningless. Increasing access to a failing medical infrastructure may sound good, but it does not address our core issues.
Healthcare for patients with chronic illnesses in the U.S. is on life support. The medical community seems helpless to fix this problem -- presumably because the solution is political, not medical.
The most important crisis facing U.S. medicine is not access to healthcare. It is access to 21st century healthcare.
{Author provides disclosures.}
-
Cancer Deaths Cost U.S. Billions in Lost Earnings Each Year
Premature death from cancer each year costs the American economy a staggering amount in lost earnings, new research found.
In 2015, 8.7 million years of life were lost due to early cancer death, amounting to $94.4 billion in lost earnings,
As described in JAMA Oncology, breast cancer cost the economy $6.2 billion in lost earnings...
Conclusions and Relevance of study: Our findings indicate large state variation in the economic burden of cancer and suggest the potential for substantial financial benefit through delivery of effective cancer prevention, screening, and treatment to minimize premature cancer mortality in all states.
{A new and interesting take on the financial toxicity of cancer and related opportunities to improve outcomes.}
https://jamanetwork.com/journals/jamaoncology/article-abstract/2737074
doi:10.1001/jamaoncol.2019.1460
-
But Doc, What Is My Prognosis?
L. Michael Glode, MD, FACP, FASCO
Jul 02, 2019
{Many of us have been on the receiving end - or a lack thereof - of a prognosis. Most of us feel that "I don't have a crystal ball" is not helpful information. This commentary provides some insight and reflections. IMO, the (currently only) reply (by Denzler) provides an excellent example of the art of sharing what a practitioner knows about treatment and prognosis in an environment of uncertainty.}
-
Wooo what a loaded subject. Interesting article but I agree with the response/comment posted by Ms Denzler. Even if one doesn't want to know all the medical terms & permutations, (and follow the research - as obviously those who read this thread prefer to do) in my opinion every patient deserves a thoughtful answer that at least gives them a chance to get their lives in order. A chance to experience their "bucket lists" so to speak, or to enjoy fully whatever time may be left. Thanks for posting Lumpie.
-
This makes me think of one of the earlier studies you posted, about the mixed results of predicted MBC, where they found that something like 86% of women who had a certain count of cancer markers in their blood went on to metastasize in the next couple of years. But then said that this kind of testing is not standard of care because it has no implications for treatment.
I'd want to know if I had an 86% chance of metastasizing in the very near future, even if there was nothing I could do about it medically. I might cut down my 401k contributions, for one!
I feel that doctors (and health insurance companies) need to work more closely with social workers and mental healthcare providers to really think through their recommendations...
-
hi salamander. what specific test was that? thank you!
-
Thanks yet again Lumpie. As one who has already metastasised and doing fine on treatment and NED, prognosis is a bit of a thing. Frankly we keep going until we don’t... end of
-
Hi April1964,
It was from an article that Lumpie posted on the previous page:
Mixed Results for Profiling in Predicting Late Recurrence in ER+ Breast Cancer Tools may, however, help select patients for extended treatment https://www.medpagetoday.com/reading-room/asco/breast-cancer/80812?xid=nl_mpt_DHE_2019-07-03&eun=g1237212d0r&utm_source=Sailthru&utm_medium=email&utm_campaign=Daily%20Headlines%202019-07-03&utm_term=NL_Daily_DHE_Active
I looked again and it was a measure of "Circulating Tumor Cells". If a person's count was 2 or more CTCs per 7.5ml of blood, they had an 83% recurrence rate. (It mentioned that the doctors didn't know if the CTC count was predicting the recurrence or showing that a recurrence had already started and was not otherwise detectable).
-
thank you salamandra! it’s sometimes hard to understand this stuff
-
This was an interesting article that I read about resistance to AIs, and relates to the question talked about above related to survival statistics.
https://erc.bioscientifica.com/view/journals/erc/2...
In particular, in talking about why studies are not showing an increased survival pattern despite the development of new drugs, the article (from 2018) had this to say:
In fact, AIs therapy presents higher clinical efficacy, prolonged disease-free survival and time to recurrence, and significantly less severe side effects than tamoxifen. Nevertheless, clinical trials generally suggest that AIs therapy does not significantly improve overall survival when compared to tamoxifen therapy (Bonneterre et al. 2001, Mouridsen et al. 2001, 2003, Milla-Santos et al. 2003, Paridaens et al. 2004, 2008, Howell et al. 2005, Chumsri 2015, Early Breast Cancer Trialists' Collaborative Group 2015). This unintended effect on overall survival may be associated with immature data from many studies, which report an increase in the number of non-cancer deaths in patients with prolonged AI therapy, and, consequently, this increase attenuates the contribution of the treatment in reducing the number of breast cancer deaths (Goldvaser et al. 2018).
Not sure if I am reading this correctly (I am not a scientist) but it certainly offers some hope.
Bev
-
I wonder how many have their circulating tumor cells tested. Now I want mine tested. I bet it's not routine.
-
Hi Jessie,
I think you are right--not many MOs do test CTCs. I had mine done in April, ordered by my naturopathic oncologist. My former MO told me years ago that the test had too many false positives and that she doesn't rely on them, but my NO told me that the test has become much more accurate in the past years and she recommended it for me. Thankfully, it was zero. Amazingly my insurance company paid for it--I guess they did because I never got a bill.
Claire in AZ
-
Claire -- that's good to know. Although I'm not sure I want to know I think I'll go ahead and request the test when I see my MO in September. Did you ever find out what that lump was or is? Kind of the same thing happened to me --- just relaxed in bed one night watching TV and felt a quick sharp pain which made me put my hand to that area. My internist couldn't even feel it. I would have never known since it didn't show on mammogram.
-
I think this article is important especially if you are having a problem with drugs you are taking. A large percentage of our generic drugs are made in China.
July 10, 2019
Should U.S. Health Care Depend on China?
Two new books expose the health dangers posed by the import of pharmaceuticals from the People's Republic of China. The dependence of America's medical system on products of questionable quality does not just endanger patients today, but risks long-term problems as the push for "Medicare for All" or some similar national health insurance scheme grows in popularity. The enormous costs of such a government-run program will pressure bureaucrats and politicians to embrace the continued outsourcing of drug production to low-cost foreign sites to keep budgets down. China Rx: Exposing the Risks of America's Dependence on China for Medicine by Rosemary Gibson and Janardan Prasad Singh is the latest work by two authors with a long record of pushing for improved safety protocols. Gibson is senior advisor at the Hastings Center Bioethics Research Institute and Singh is an economic advisor at the World Bank. Bottle of Lies: The Inside Story of the Generic Drug Boom is by...(Read Full Article)
-
Hi Jessie, I sent you a PM...
Claire in AZ
-
FDA 'Satisfies' FOIA Request on Hidden Database
The FDA has closed out its file on the Kaiser Health News Freedom of Information Act request that exposed a hidden database of reported problems with medical devices.
KHN posted its correspondence with the FDA, which said that releasing the information online should satisfy the news outlet's request. The agency published the "alternative summary reporting" database on June 21 --it can be found here.
The program bypassed a public database known as MAUDE that is used by doctors, researchers, and patients to report and signal problems with devices. It included 5.7 million incidents of malfunctions and injuries linked to medical devices over 2 decades.
References:
-
HHS Inspector General Finds Serious Flaws In 20% Of U.S. Hospice Programs
There's no easy way for consumers to distinguish the good hospices from the bad. Two new government studies are the government's first to look at hospice deficiencies nationwide. The Office of the Inspector General in the Department of Health and Human Services found that from 2012 through 2016, health inspectors cited 87% of hospices for deficiencies. And 20% of hospices had lapses serious enough to endanger patients. The Centers for Medicare & Medicaid Services (CMS), doesn't make information on hospices previously cited for deficiencies available on Hospice Compare, its website for consumers, even though the agency has the authority to post at least some of that data.
https://www.npr.org/sections/health-shots/2019/07/09/739471717/hospice-oig-reports
-
New discovery targets stem cells of claudin-low BC.
-
when they test the tumor after surgery do they also test it for stem cells?
-
April1964:
To the best of my knowledge, there is no test for stems cells. I believe that they are presumed to be present in all tumors and are the mechanism by which cancer spreads. Also, as the article notes, "At present, there are no drugs that can kill cancer stem cells, but people are looking for them..." So even if it were possible to test for them, the test would probably not be done routinely if it were not "actionable" - in other words, it didn't indicate some specific treatment. I hope we will 'get there' - sooner rather than later!
-
Wow lumpie, does that mean chemo, radiation and aromatase inhibitors don’t kill stem cells?
-
thanks so much lumpie for explaining that!
-
How Long Is This Going to Take?
{In this memoir-esque piece, an oncologist reflects on his multi-year odyssey with a quirky stage 4 cancer patient.}
"There are times when I wished I might capture Leroy's spirit in a bottle to be passed around so that I and others might take a healthy swig of it from time to time.... {It} helps encourage us to "keep on keepin' on" at what we do."
https://ascopubs.org/doi/full/10.1200/JCO.19.01102
-
Effects of marital status on breast cancer survival by age, race, and hormone receptor status: A population‐based Study
First published: 02 July 2019
It remains unclear whether marital status could affect the breast cancer‐caused special survival (BCSS) of patients with breast cancer. Therefore, we sought to explore the influence of demographic and pathological factors on prognosis of patients with breast cancer.
Our findings demonstrated that married and single patients with breast cancer had better prognosis than their DSW (divorced/separated/widowed) counterparts. Age, race, and HRs could affect the correlation between marital status and BCSS.
we used SEER*Stat 8.3.4 software to extract eligible patients included in the database.
-
marijen I believe that chemo is reasonably effective at killing them systemically; radiation kills them locally; and aromatase inhibitors cut off their food supply if they are hormone driven. But there is still no good test for them.... especially if they are "hiding" somewhere in the body. Perhaps research on CTC (circulating tumor cells) will eventually allow an assessment of whether they are present in the sampled blood specimen....and, therefore, likely to be lurking elsewhere....
{Note: Upon rereading, I note that the article says "At present, there are no drugs that can kill cancer stem cells, but people are looking for them" so maybe chemo's systemic effect is limited to less potent cells that have broken off and are circulating. Still lots to figure out about this disease process.}
-
Sports playbook helps doctors predict cancer patient outcomes
Using in-game win probability techniques, Stanford researchers devised a way to predict a cancer patient's outcome at any point during treatment. The approach could also inform treatment decisions.
...researchers at the Stanford University School of Medicine have taken a page from this playbook to generate more accurate prognoses for cancer patients. They've done so by designing a computer algorithm that can integrate many different types of predictive data — including a tumor's response to treatment and the amount of cancer DNA circulating in a patient's blood during therapy — to generate a single, dynamic risk assessment at any point in time during a patient's course of treatment. Such an advance could be deeply meaningful for patients and their doctors.
"Our standard methods of predicting prognoses in these patients are not that accurate," Kurtz said. "Using standard baseline variables it becomes almost a crystal ball exercise. If a perfectly accurate test has a score of 1, and a test that assigns patients randomly to one of two groups has a score of 0.5 — essentially a coin toss — our current methods score at about 0.6. But CIRI's score was around 0.8. Not perfect, but markedly better than we've done in the past."
-
My parents were on hospice in my home for 6 years -- I know that's unusual since hospice was developed as a 6 month program ---- but I kept them on medicare only --- no supplement or HMO type program. Medicare is so large they don't monitor as well as private business. Anyway, our hospice was very good -- however the R.N. told me that they go into many very bad situations -- even some involving neglect --- but they never report the neglect. When I asked them why I was told the word would get around and they could lose potential patients. Isn't that horrible!!!
-
jessie123: that is sad. IMO, the state of care for our elders does not reflect well on us as a society. It is troubling that neglect is not reported.... but some seniors undoubtedly fear the alternative more than the neglect. I have personally observed some terrible states of care... but with no longer term care coverage, we pretty much 'hang our seniors out to dry.' The wave of elders that is coming may change things but not without a great deal of pain on the parts of many, I fear.
-
Why Elephants Rarely Get Cancer
They have multiple copies of a gene that causes mutated cells to commit suicide.
"I've always been so enamored with elephants -- one of the things that's just amazing to me is that elephants have such an incredibly low rate of cancer. And it doesn't make any sense that elephants have a low rate of cancer, because they're so big and their cells are dividing so fast,"
"Their cells are dividing so quickly that just by chance alone they should just have really high rates of mutation and cancer. But they have a gene -- they have many copies of this gene, as a matter of fact -- that causes their cells to commit suicide if they mutate. It could not have evolved to be that large if it did not also evolve to have that gene,"
Researchers at the University of Utah are now working with human cells to see whether the elephant's cancer-fighting technique could lead to new medical treatments.
https://www.insidescience.org/video/why-elephants-rarely-get-cancer
-
If I was a collector, I would have wall shelves with nothing but elephant sculptures.
-
More Attention Needed on Misdiagnosis, Experts Say
Study finds many cases fall into three disease categories
More money should be spent on researching ways to reduce misdiagnosis and to get patients diagnosed more quickly, several experts said here. "For too long, the problem of inaccurate and delayed diagnosis was not given the attention it deserved," Paul Epner, MEd, CEO and co-founder of the Society to Improve Diagnosis in Medicine (SIDM)... {A} study, published in Diagnosis, looked at nearly 12,000 diagnostic error malpractice cases and found that the "Big Three" disease categories -- vascular events, infections, and cancers -- accounted for 74.1% of high-severity cases, with the top five diseases in each category accounting for 47.1%. Roughly half of the cases involved primary care clinicians; the rest were divided between medical specialties like cardiology, gastroenterology, and neurology (16.3%), surgical specialties (15.4%), and diagnostic services like radiology and pathology (14.8%). Having physicians learn from their mistakes is important to improving diagnoses, Burstin said. "All of us can immediately think of a patient they saw where there is clearly an issue ... Some of it is that we don't know what the ultimate diagnosis was," she said. "Feeding that information back to clinicians is such a powerful learning tool ... Those opportunities [are needed] for better systems, better understanding, and outcome tracking." Several of the panelists told their own misdiagnosis stories. {Some are recounted in the article.} "Looking back, I just wish someone had listened to me..."
https://www.degruyter.com/view/j/dx.ahead-of-print/dx-2019-0019/dx-2019-0019.xml
-
-
Lumpie, that link about the Elephants having genes that cause cells with mutation errors to commit suicide is so very interesting! Coming from a humorous standpoint, it makes me wonder if fossils of dinosaurs might have dna with similar genetic code. I mean what's bigger than Elephants? Oh maybe a Brachiosaurus???! LOL. But this really is so exciting to learn. IMO there is SO much we can and should be learning from Elephants. I've always been enamoured by them. Thankfully I was able to go to AFrica as a part of my college studies back in the 90s and see herds of them that stretched for as far as the eye could see. Just amazing creatures.

-
And whales! "Scientists know that age and weight are risk factors in the development of cancer. That should mean that whales, which include some of the largest and longest-lived animals on Earth, have an outsized risk of developing cancer.
But they don't. Instead, they are less likely to develop or die of this enigmatic disease. The same is true of elephants and dinosaurs' living relatives, birds." (sorry can't post links yet)
-
Pairing targeted drugs for breast and lung cancer could overcome treatment resistance
Targeted drugs for breast and lung cancer could be used together to overcome resistance to treatment in several different tumour types, a new study shows. Scientists discovered that when the breast cancer drug palbociclib was combined with the lung cancer drug crizotinib, the two-drug combination was significantly more effective against cancer cells in the laboratory than either drug used on its own...
Based on this discovery, the researchers found that pairing CDK4/6 inhibitors such as palbociclib together with crizotinib -- which blocks MET activity -- created a combination treatment that was much more effective than either drug on its own against cancer cells grown in the lab or human tumours growing in mice.
https://www.sciencedaily.com/releases/2019/07/190711200609.htm
-
How cell-free DNA (cfDNA) can be targeted to prevent spread of tumors
"After infection or injury, a group of specialized immune cells called neutrophils release small sticky fibers of chromatin, which is undegraded dead-cell DNA. These fibers are called neutrophil extracellular traps (NETs). Although NETs can stop harmful bacteria from spreading in the bloodstream, NET release can sometimes become uncontrolled; this could cause clotting or embolism (lodging of the clot inside a blood vessel), a potentially fatal condition. Prof Mizuta states that DNase1L3 can degrade NETs into cfDNA and thus be used to treat thrombosis caused by NETs.
NETs are also known to be the "seeding soil" for tumors. Tumor cells released in blood might latch onto NETs and grow on them and spread to other organs. For this, Prof Mizuta says, "Because DNase1L3 degrades NETs and generates cfDNA, we speculate that DNase1L3 treatment may also be useful to prevent tumor metastasis. We are now conducting experiments to test this speculation."
That said, can more research on cell-free DNA make human life cancer-free? Only time will tell..."
-
Imprinted Spheres Fight Breast Cancer: Inhibition of HER2 on tumor cells by molecularly imprinted nanoparticles
A particularly aggressive, metastasizing form of cancer, HER2-positive breast cancer, may be treated with nanoscopic particles "imprinted" with specific binding sites for the receptor molecule HER2. As reported by Chinese researchers in the journal Angewandte Chemie, the selective binding of the nanoparticles to HER2 significantly inhibits multiplication of the tumor cells.
-
Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: Evidence from a national audit of cancer diagnosis
Includes a long list of breast cancer symptoms, a Venn diagram of different categories, and analysis of how non-lump and non-breast symptoms may lead to delay.
https://www.sciencedirect.com/science/article/pii/S1877782117300565
-
Debbew - is this the article you were referring to? Seems interesting if so. I'm currently in a "lump" + "non lump" symptoms group with this "new" thing that is going on with my Left nipple. Guess we'll see what my SO makes of it next week. Thanks for the article. The Venn diagram was easy to understand.
'Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: Evidence from a national audit of cancer diagnosis'
-
Oops, I've fixed my link. Thanks for catching that! Yes, you found the same study. Thanks and hoping for a good outcome for you!
-
I'd be curious to knw if any set of symptoms correlated with -type of cancer, -grade of cancer, -survival outcomes...?
-
santabarbarian, symptoms like you might have experienced pre-dx? Good question.
-
I had a red spot and a small fever, like a breast infection. I poked the area and sure enough a lump too. Came on all of a sudden from nowhere.
-
my breast felt very itchy above where the tumor was but i could not feel a lump there... found on mammo
-
Low Dose Naltrexone
Low dose naltrexone, referred to as LDN, is given as a capsule in the 3 mg to 4.5 mg range for cancer, as opposed to the 50 mg dose given for addiction. [1]
Low dose naltrexone might exert its effects on tumor growth through a mix of three possible mechanisms:
- By inducing increases of metenkephalin (an endorphin produced in large amounts in the adrenal medulla) and beta-endorphin in the blood stream;
- By inducing an increase in the number and density of opiate receptors on the tumor cell membranes, thereby making them more responsive to the growth-inhibiting effects of the already-present levels of endorphins, which induce apoptosis (cell death) in the cancer cells; and
- By increasing the natural killer (NK) cell numbers and NK cell activity and lymphocyte activated CD8 numbers, which are quite responsive to increased levels of endorphins. [2]
-
-
Curcumin plays a vital role in fighting cancer
 Sunil Pai, MD +
Sunil Pai, MD +
https://www.cancertutor.com/vital-role-curcumin-ca... -
Stolen from skyfly on another thread:
MIT supercharges cancer immunotherapy with a booster vaccine
"The team tested the vaccine on mice that had glioblastoma, melanoma or breast cancer, and saw a huge improvement in the T cell response. The mice were given about 50,000 CAR-T cells and then given a booster vaccine the next day, and then again a week later. In 60 percent of the mice, the tumors were completely eliminated. That's likely thanks to the boost in CAR-T cell numbers, which two weeks after treatment make up 65 percent of the total T cell population.
By contrast, in the mice that were given CAR-T cells but not the vaccine, there was no effect on the solid tumors and the CAR-T cells themselves were hard to detect in the bloodstream.
The technique also seemed to prevent the tumors from coming back later on."
https://newatlas.com/vaccine-supercharges-cart-cell-cancer-therapy/60550/
-
Blood-Based Markers Key to Precision Medicine Approach in Breast Cancer
Mark E. Burkard, MD, PhD, discussed the significance of utilizing markers in the blood and highlighted emerging actionable mutations in breast cancer.
(Registration at onclive.com is free
-
Researchers determine epigenetic origin of docetaxel-resistant breast cancer
"Researchers at the Bellvitge Biomedical Research Institute (IDIBELL) have published a study in Molecular Cancer Research in which they identify methylation patterns associated with different subtypes of breast cancer... '[W]e have identified changes in the methylation of specific genes that can improve the classification of patient samples, thus helping us know whether they will respond to docetaxel treatment or not,' Dr. González-Suárez says. 'The differentially methylated genes identified can help us find treatments associated with the new subgroups.'"
-
Broken heart syndrome may be linked to cancer, study suggests
Can cancer break your heart? A new study suggests that there's a link between cancer and a condition called broken heart syndrome.
The study, published Wednesday in the Journal of the American Heart Association, found that 1 in 6 people with broken heart syndrome had cancer, and that these patients in particular were more likely to die within five years, compared with broken heart syndrome patients without cancer.
Broken heart syndrome, which is also called stress cardiomyopathy or takotsubo cardiomyopathy, is a temporary condition that can be brought on by stressful situations. During broken heart syndrome, one part of the heart stops pumping normally, which may cause the rest of the heart to pump more forcefully, according to the Mayo Clinic.
-
My 5-Month Interlude as a Disabled Professor
{A professor reflects on his period of disability. Many of us will relate to how our lives change when we are affected by a disabling condition.... such as cancer....}
"...my five-mouth travail provided a glimpse of an unnerving alternative reality for me as a classroom teacher. It caused me to see with new eyes how even seemingly insignificant things can create major obstacles for disabled faculty members and students as they go about trying to teach and learn on a college campus."
{No subscription required for this article but you may need to sign in.}
-
Cancer Cells Switch Sugar for Fatty Acids to Spread Around the Body
Scientists have uncovered a crucial change in cancer cells that allows them to spread around the body – by switching from sugar to fatty acids to fuel their growth.
"We found that high levels of the protein AKR1B10 help tumour cells adjust to new environments as cancer spreads from the breast to other organs such as the lungs.
This research significantly improves our understanding of cancer cell metabolism and metastatic relapse and could lead to new avenues of exploration for new therapies and treatments for patients with metastatic breast cancer."
-
Another way to knock out the nasties!
I hope some of the remarkable research being done gets the funding to work with humans! Would be good if Governments could speed up these protocols for terminal patients
-
Cancer survivors are twice as likely to suffer from chronic pain
Researchers estimate over five million survivors struggle with the condition
A new study explored a unique symptom common to over five million cancer survivors: chronic pain.
According to researchers, cancer survivors are twice as likely to struggle with chronic pain compared with those who never had the disease.
"This study provided the first comprehensive estimate of chronic pain prevalence among cancer survivors," saidresearcher Dr. Changchuan Jiang. "These results highlight the important unmet needs of pain management in the large, and growing cancer survivorship community."
-
Aggressive breast cancers more likely to hit black and younger women
Black and younger women face elevated risks of developing breast cancers that are not only aggressive but also less responsive to treatment, a new study confirms.
Conclusions: The results of the current study demonstrated that there is a significant burden of disease in TNBC diagnosed among women of color, specifically non‐Hispanic black women, and younger women. Additional studies are needed to determine drivers of disparities between race, age, and stage of disease at diagnosis.
https://onlinelibrary.wiley.com/doi/10.1002/cncr.32207
https://doi.org/10.1002/cncr.32207
{Don't they keep doing this research and finding the same thing?}
-
Have Cancer, Must Travel: Patients Left In Lurch After Hospital Closes
Another example of an all too familiar trend — a rural hospital closes forcing patients to travel long distances to receive the care they need. The article looks at the impact on cancer patients in particular, as well as the community at large, when a local hospital like this shuts down. "Rural cancer patients typically spend 66% more time traveling each way to treatment than those who live in more urban areas, according to a recent national survey by ASCO."
-
Billionaire Sean Parker is nerding out on cancer research. Science has never seen anyone quite like him
An interesting article that looks at how billionaire Sean Parker, known as an innovator and disruptor in Silicon Valley, is bringing his approach and money to cancer immunotherapy.
"While 'medicine in general can be so staid and cautious,' said D.A. Wallach, a life sciences investor who has known Parker since around 2011, 'you've got in Sean a billionaire who doesn't need to answer to anyone, who's incredibly intellectually engaged with this science, and who has believed for a long time that he knows what the answer's going to be.'"{Most Stat articles require a subscrition, but I was able to access this one.}
-
{Don't they keep doing this research and finding the same thing?}
YES.
-
'Big Three' Diagnostic Errors Account for Nearly 75% of All Serious Harm | HealthLeaders Media
KEY TAKEAWAYS
Diagnostic errors that led to death or permanent disability were linked with misdiagnosed cancers (37.8%), vascular events (22.8%) and infections (13.5%) — which led the researchers to refer to them as the 'big three.'
Half of the most-severe harm cases ended in patient death and the other half resulted in permanent disability.
Failures of clinical judgment caused more than 85% of the misdiagnosed cases.
-
Paige touts study that validates its cancer diagnosis AI
Artificial intelligence-aided pathology company Paige said today that a new study has found that its computational decision-support systems can help clinicians diagnose and treat cancer. Published in Nature Medicine, a paper on the study describes an AI system for computational pathology that achieves clinical-grade accuracy levels. Researchers developed deep-learning algorithms to build a system that can detect prostate cancer, skin cancer and breast cancer with near-perfect accuracy, according to the paper.
https://www.nature.com/articles/s41591-019-0508-1
DOI: https://doi.org/10.1038/s41591-019-0508-1
-
A differentiated approach to referrals from general practice to support early cancer diagnosis – the Danish three-legged strategy
This paper argues for and describes the organisation of the Danish three-legged strategy in diagnosing cancer.... urgent referral to diagnostic centres when we need quick and profound evaluation of patients with nonspecific, serious symptoms and finally easy and fast access to 'No-Yes-Clinics' for cancer investigations for those patients with common symptoms in whom the diagnosis of cancer should not be missed.
...that patients with an early-stage cancer present very differently in general practice and that a single focus on alarm symptoms or red flags might not be sufficient.
A study among Danish GPs...showed that in about one-third of cases, the GPs reported a quality deviation which was strongly associated with longer diagnostic intervals ...
...we saw that countries with a strong gatekeeper role also had the lowest cancer survival rates. This could suggest that in some countries where GPs were good gatekeepers, the GPs had become too reluctant to refer early to diagnostic investigations. Further, that access to diagnostic services in the initial phase was slow or rationed, resulting in patients not obtaining timely cancer investigations.
doi: 10.1038/bjc.2015.44
{After reviewing the above referenced article "Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: Evidence from a national audit of cancer diagnosis," I was interested to read about how other regions were approaching this challenge. This article describes the organisation of the Danish three-legged strategy.}
-
Accelerate, Coordinate, Evaluate Programme: a new approach to cancer diagnosis
ACE was initiated in June 2014 as a 3-year NHS England initiative...The programme aims to address the NHS outcome of 'preventing people from dying prematurely', as well as improving overall patient experience along the diagnostic pathway. ACE supports many projects looking at the important role GPs and other primary care health professionals have in recognising symptoms of cancer and referring patients who need further investigation.
...one cluster is considering new approaches for patients that GPs find most difficult to place on a specific pathway, particularly those who present with vague but concerning symptoms.
-
Tumor Infiltrating Lymphocytes and Breast Cancer
Many of you have read about the announcement a year or so ago from the National Institutes of Health. Dr. Steven Rosenberg, the leading authority on immunotherapy, a treatment he pioneered that uses a person's own immune cells to fight cancer, told the world about Judy Perkins. Judy participated in a clinical trial that was part of the larger NIH tumor infiltrating lymphocyte cancer trial run by Dr. Rosenberg. Judy had MBC that was not responsive to treatment. Since participation in the clinical trial, Judy has been NEAD. You can see Judy's presentation at the NBCC Leadership Summit 2017 here: https://nsp.performedia.com/node/16793 Her talk is about 12 minutes. Additional presentations follow.
-
Something I came across. Sorry if already posted.
-
For those interested in advocacy....
CPAT Webinar: Meet with Your Lawmakers During August Recess
Wednesday, July 24, 2pm Eastern
The August Congressional district work period is right around the corner. No need to travel all the way to Washington, DC. This is a great opportunity to meet with Members and their staff in a district office to discuss cancer care policy and legislation.
To help you get started, NCCS {National Coalition for Cancer Survivorship} will host a webinar on Wednesday, July 24 at 2:00pm EDT to discuss everything you need to know about conducting district meetings.The Cancer Care Planning and Communications Act (CCPCA) is also scheduled to be reintroduced soon, so we'll be reviewing this important legislation for you as well.
Instructions to Join the Webinar
You do not need to register for this webinar, just follow the instructions below to join on Wednesday. You may join the webinar as early as 1:50pm.
- Join the webinar here: https://join.startmeeting.com/nccs_web
- Type your name and email address, and click "Join."
Note: If prompted, you do NOT need to install the StartMeeting.com browser extension in order to join the webinar. - To listen by phone: Dial (781) 448-0068. (no access code needed)
- Or, to listen through your computer speakers:
- Note: If your device does not have a built-in microphone, and you do not otherwise have a headset or microphone plugged in, the system may not recognize your speakers and you will have to listen in by phone (see Step 3).
- Click the phone icon on the left side of the toolbar, and then select "Mic & Speakers"
- If a pop-up box appears in your browser requesting access to your microphone, click Allow. Your mic will be muted throughout the webinar.
If you encounter any problems dialing in, call (877) 553-1680 for customer care.
Can't make the webinar? If the webinar conflicts with your schedule, NCCS has you covered. We will post the recording and any associated resources on the main CPAT page as soon as it is available.
- Join the webinar here: https://join.startmeeting.com/nccs_web
-
Not specific to breast cancer, but...
IBM has released three artificial intelligence (AI) projects tailored to take on the challenge of curing cancer to the open-source community...
IBM is working on the PaccMann algorithm [the first project] to automatically analyze chemical compounds and predict which are the most likely to fight cancer strains, which could potentially streamline this process...
The second project is called "Interaction Network infErence from vectoR representATions of words," otherwise known as INtERAcT. This tool is a particularly interesting one given its automatic extraction of data from valuable scientific papers related to our understanding of cancer...
The third and final project is "pathway-induced multiple kernel learning," or PIMKL. This algorithm utilizes datasets describing what we currently know when it comes to molecular interactions in order to predict the progression of cancer and potential relapses in patients.
https://www.zdnet.com/article/ibm-reveals-ai-projects-aiming-to-find-cancer-killing-drugs/
-
HER2-Positive Breast Cancer
FDA Approval Sought for Neratinib Combo in HER2+ Breast Cancer
An application has been submitted to the FDA for neratinib for use in combination with capecitabine for the third-line treatment of patients with HER2-positive metastatic breast cancer.
Expert Explains Evolution of De-Escalating Therapies in HER2+ Breast Cancer
Keerthi Gogineni, MD, MSHP, discusses several trials in the breast cancer field, specifically looking at de-escalation approaches with therapy.
Key Trials Showcase the Utility of Neratinib in HER2+ Breast Cancer
Michel Velez, MD, provides perspective on the clinical experience with neratinib in patients with early-stage HER2-positive breast cancer as well as promising data that may lead to an indication in the metastatic setting.
Incorporating Neoadjuvant and Adjuvant Data in Early-Stage HER2+ Breast Cancer
Yee Chung Cheng, MD, discusses the importance of integrating neoadjuvant and adjuvant trial data into practice in order to optimize outcomes for patients with early-stage HER2-positive breast cancer.

-
Where Do Your Med School Tuition Dollars Go?
'Our debt is an amount of money that schools might not actually need'
Daniel Barron, MD, a resident at Yale, detailed his quest to learn How are medical school tuition dollars actually spent? in a Scientific American post. Barron talked to Robert Grossman, MD, dean of NYU School of Medicine and CEO of NYU Langone Health, who famously nixed tuition for the school's medical students last year. Grossman said the $25 million in tuition that students used to pay largely went to supporting "unproductive faculty" -- those who don't get grants, teach, or see patients. Grossman also said this amount could effectively be considered a "rounding error" in the university's $10 billion annual budget. "What's frustrating is the idea that even though we've sacrificed so much already, our debt is an amount of money that schools might not actually need," Budde said in the post. Each year, thousands of new physicians graduate with an average of $195,000 in debt. We ought to be able to know where our tuition dollars are going and what we're buying with our money.
{Troubling....}
-
Predicting Breast Cancer Response With 'High' TMB
'Desperately seeking better biomarkers and an understanding of their relationship to one another'
The recent approval of nab-paclitaxel plus atezolizumab in patients with PD-L1 immune cell-positive triple-negative breast cancer, based on results from the Impassion130 study, has led to an explosion in the number of clinical trials in search of other biomarkers to enrich for responding breast cancer patients.
Discussion re TAPUR is a single-arm nonrandomized study. Patients eligible for TAPUR have advanced cancer and no standard treatment options.
-
Certain Breast Implants, Tissue Expanders Recalled Due to Cancer Link
Steve DuffyAllergan is recalling BIOCELL textured breast implants and tissue expanders due to the potential risk for breast implant-associated anaplastic large cell lymphoma (BIA-ALCL).
The move to recall was based on an analysis of medical device reports submitted to the Food and Drug Administration (FDA) related to BIA-ALCL and BIA-ALCL-related deaths associated with these devices. "Once the evidence indicated that a specific manufacturer's product appeared to be directly linked to significant patient harm, including death, the FDA took action to alert the firm to new evidence indicating a recall is warranted to protect women's health," said FDA Principal Deputy Commissioner Amy Abernethy, MD, PhD.
In a press release, Allergan said that "Effective immediately, healthcare providers should no longer implant new BIOCELL textured breast implants and tissue expanders." The recall includes the following products: Natrelle Saline-Filled breast implants, Natrelle Silicone-Filled breast implants, Natrelle Inspira Silicone-Filled breast implants, and Natrelle 410 Highly Cohesive Anatomically Shaped Silicone-Filled breast implants, Natrelle 133 Plus Tissue Expander and Natrelle 133 Tissue Expander with Suture Tabs. A complete list can be found here.
As of July 6, the FDA lists 573 unique cases of BIA-ALCL globally, of which 481 are attributed to Allergan implants. Thirty-three deaths have been reported; 12 of the 13 deaths in which the manufacturer was known were confirmed to have an Allergan breast implant at the time of BIA-ALCL diagnosis.
"The recall of these textured implants is a big deal in protecting women from the potential risks of developing, and dying from, this rare type of aggressive lymphoma," said Joshua Brody, MD, Director of the Lymphoma Immunotherapy Program at Mount Sinai. "While case reports have suggested a potential link between some types of breast implants and this disease for over 20 years, it has taken time to gain sufficient evidence to suggest, and understand, the causality."
At this time, the FDA recommends that healthcare providers do not remove these or other types of breast implants in patients who have no symptoms due to the low risk of developing BIA-ALCL, however patients should be informed of the risk. In patients with late onset, peri-implant changes, providers should consider the possibility of BIA-ALCL; in some cases, patients presented with a seroma, mass, hardening adjacent to the breast implant.
Additional recommendations for providers and patients can be found here.
Related Articles
- FDA: Breast Implants Linked to Cancer Can Still Be Sold in US
- Long-Term Outcomes of Breast Implants Explored
- FDA: Number of U.S. Women With Breast Implant-Caused Cancer Has Increased
"Many cases of implant-associated lymphoma have developed mutations and expression of immune-suppressive proteins which prevent anti-tumor immune cells from clearing the cancer, and these chances likely begin with the inflammation induced by some implants," added Brody. "By preventing further use of these implants, the FDA is helping women to protect themselves from the medically serious and emotionally exhausting effects of these risks."
The FDA also announced today that additional actions are being considered to help inform women on the benefits and risks of breast implants. These may include changes to the labeling for breast implants to include a Boxed Warning and a patient decision checklist.
For more information visit FDA.gov.
-
PLEASE read this article with care - not just the headline. BCO had posted extensively about this issue and the posts have been very accurate & informative.
Note: The risk is 6x as high - not 60% as stated on the television today. The craziness has officially started. As Marijen quoted, there have only been 33 deaths out of 573 cases sited. That is 6% - a relatively small number.
Note: The FDA is NOT advocating for the removal ('explant') of these products if you aren't having any problems. If you have questions or are having symptoms, by all means make an appointment with your plastic surgeon. Perhaps he/she will recommend an MRI as the next step. But this is not a call for mass panic.
I had an out of town friend call me so upset because I was going to die. Well..... I love my 410s. They have been in place for 9 years. At this point, I don't have any problems. I will see my PS just to discuss the issue, but at this point I certainly don't plan to have them pulled out.
-
Cellular soldiers created using the body's own defenses can track down and kill escaping cancer cells during surgeries, preventing metastasis and saving lives, a Vanderbilt University biomedical engineer has discovered, particularly in cases of triple negative breast cancer...
"We've tested this both in the bloodstream and in hundreds of blood samples from cancer patients being treated in clinics across the country. In all cases, within two hours, the viable cancer cells are cleared out. This has worked with breast, prostate, ovarian, colorectal and lung cancer cells."
Not only can the method work during surgeries, King said, but potentially with patients who already suffer metastatic cancer in multiple sites and who have no worthwhile treatment options...
The group's past experiments with TRAIL-coated leukocytes were effective in blocking metastasis, but required multiple repeated injections to sustain their beneficial effect. King said this new breakthrough overcomes those issues by designing three simple doses to coincide with the surgical procedure.
https://medicalxpress.com/news/2019-07-cellular-soldiers-cancer-cells-loose.html
-
Ah, so the cancer cells do escape during surgery! Of course they do
-
A new way to stop cancer cells from killing their healthy neighbors
Moreno and his team discovered that neighbouring cells in the body are constantly evaluating each other's fitness level by using special markers that each cell exhibits on its surface...
Next, to observe whether the fitness fingerprints impact cancer growth, the team analysed the expression of these four types in different types of tissues: malignant cancer (breast and colon), benign tumors (breast and colon), tissue adjacent to the tumour and normal tissue.
Their analysis revealed several striking findings: in normal tissue, the expression of Win was overall quite sparse, and expression of Lose was even lower. In contrast, the expression of Win was significantly increased in all tumors, with higher levels in malignant tumors than in benign...
Next, to test the full therapeutic potential of this approach, the team decided to combine blocking fitness fingerprints expression with chemotherapy. This two-pronged approach was very successful: "we were able to further reduce, and in some cases completely eliminate, tumorigenesis!", says Gogna.
https://medicalxpress.com/news/2019-07-cancer-cells-healthy-neighbors.html
-
Somebody finally admits it! "Surgical intervention in breast cancer is a known cause of metastatic growth and accelerated tumor relapse, either because of cancer cells shed during the process, inflammation at the wound site or a combination of the two factors. Chemotherapy is the most widely used treatment for the resulting metastasis, but still, the five-year survival rate for triple negative breast cancer sits well below 30 percent."
-
Beverly Hills Plastic Surgeons React to Breast Implant Recall: "Don't Panic" | Hollywood Reporter
https://www.hollywoodreporter.com/news/beverly-hil... -
Too Many Medicines Simply Don't Work
A pair of new studies sheds light on an old problem: Some things doctors do are useless. Some are even harmful.
ByPeter Coy
https://www.bloomberg.com/news/articles/2019-05-30... -
Pilot Study of Five-Hour Molecular Test Accurately Distinguishes Malignant and Benign Breast Tumors
Novel technology based on epigenetic alterations could shorten wait for a definitive diagnosis in resource-poor settings
A team led by Johns Hopkins Kimmel Cancer Center investigators reports that a new laboratory test they developed to identify chemical changes to a group of cancer-related genes can accurately detect which breast tumors are cancerous or benign, and do it in far less time than gold-standard tests on biopsied breast tissue.
-
New technology targets cancer, other diseases, and hidden elements that allow those diseases to thrive
A Purdue University-affiliated startup has created a platform aimed at treating relapse patients for cancers and other diseases by taking a holistic approach of not only seeking to impede the main cause but also to stop other elements that help that disease thrive. ...a platform that makes complex drug molecules rapidly using bioinformatics, multi-component compound synthesis and the understanding of disease biology. what KinaRx is doing is developing drugs that hit not only the main disease drivers but also the collaborative players that allow the disease to progress." "Kinases basically signal so many processes in a cell. So they are drug targets for many diseases," ... "We have developed a technology that is so powerful that we will be able to target many diseases associated with kinases."
-
FDA: Allergan Should Pull Some Breast Implants
Risk of rare lymphoma six times more common with company's textured implants
The FDA called on Allergan to pull certain textured breast implants from the U.S. market due to the risk of breast implant-associated anaplastic large cell lymphoma (ALCL).
Allergan said it would comply and that it was moving forward with a worldwide recall of six products in its Natrelle line of implants and tissue expanders...
https://www.medpagetoday.com/publichealthpolicy/fdageneral/81194
-
Share Triumph Conference
{Promo says:} LEARN FROM 40+ CANCER SURVIVORS, METAVIVORS, CAREGIVERS AND MEDICAL EXPERTS ABOUT DIAGNOSIS, TREATMENT AND THE AFTERMATH SO YOU CAN KEEP YOUR SPIRIT INTACT & SHARE YOUR TRIUMPH
{free pass to this online event here:} https://conference.sharetriumph.com/?utm_campaign=16&utm_content=SlC8Z_G0vbKQGsWqnu1tM5xKZ1E&utm_medium=email&utm_source=newsletter&utm_term=campaign-16
{I don't know much about this online conference but I am getting loads of email blasts about it. Seems to have lots of corporate backers and an extensive list of presenters. Dates Aug 5-15, 2019.}
-
First-Line T-DM1 for Patients With HER2+ Advanced Breast Cancer Who Are Unsuitable for Taxane-Based Therapy
- In the randomized, phase III, MARIANNE trial, the authors evaluated the efficacy of trastuzumab emtansine (T-DM1), T-DM1 plus pertuzumab, and trastuzumab plus a taxane in 1095 patients with HER2-positive breast cancer and no prior therapy for advanced disease. This post hoc, landmark analysis compared overall survival (OS) among the groups. Median OS was similar across all three groups. Toxicity was less in the T-DM1 arms compared with the trastuzumab plus taxane arm.
- Although the control group of trastuzumab plus taxane has since been superseded by the combination of trastuzumab, pertuzumab, and a taxane for first-line treatment, the authors conclude that these findings still offer support for T-DM1 as first-line treatment in patients with HER2-positive metastatic breast cancer deemed unsuitable for taxane-based therapy.
Interesting commentary/observations by Lee S. Schwartzberg MD, FACP -
Predictive and Prognostic Value of Stromal TILs Before and After Neoadjuvant Therapy in Triple-Negative and HER2-Positive Breast Cancer
- This retrospective analysis was designed to evaluate the predictive and prognostic value of stromal tumor-infiltrating lymphocytes (TILs) before and after neoadjuvant therapy (NAT) for patients with triple-negative and HER2-positive breast cancer. Low levels of TILs prior to neoadjuvant therapy were associated with a lower pathologic complete response rate in both triple-negative and HER2-positive disease.
- Low levels of pre–neoadjuvant therapy TILs were associated with a poor overall prognosis in patients with triple-negative breast cancer.
- CONCLUSION: In TN and HER2+ BCs, low pre-NAT TILs tumours had a low likelihood of achieving pathological complete response (pCR). In TNBC with residual disease (RD), both low pre- and post-NAT TILs were associated with shorter (relapse-free survival) RFS. These results suggest that TILs information should be taken into account when additional therapies may be given in the post-neoadjuvant setting.
https://www.practiceupdate.com/C/86600/56?elsca1=emc_enews_topic-alert
-
Michael Lisanti and antibiotics: the next cancer revolution
https://www.healtheuropa.eu/michael-lisanti-antibiotics/88900/ -
New discovery could open up PARP inhibitors to more cancer patients
PARP inhibitors have transformed treatment for breast and ovarian cancers, but their use has been limited to the small proportion of patients who have BRCA mutations. New research out of UT Southwestern Medical Center has uncovered a mechanism by which the drugs attack cancer, suggesting they could be put to use in many more patients.
https://www.fiercebiotech.com/research/new-pathway-could-open-up-parp-inhibitors-to-more-patients
-
On this article above: Predictive and Prognostic Value of Stromal TILs
Does anyone actually measure our stromal TILs? Would we or our docs know and adjust our treatments or expectations based on that?
-
A new therapeutic treatment uses engineered stem cells to target and kill cancer bone metastases while preserving the bone, a study with mice shows.
"This is a safe and almost nontoxic treatment compared to chemotherapy, which often leaves patients with lifelong issues."
Sandra Spivey, an Orange County patient advocate who has been living with metastatic breast cancer since 1997, has experienced firsthand the ravages of traditional treatment.
"Chemotherapy can kill both cancer cells and normal cells and create drastic side effects," she says. "I have lost my hair; I have lost sensation in my hands and feet. Most of all, chemotherapy really robs you of your time. This new targeted approach could improve quality of life both during and after treatment."
https://www.futurity.org/bone-metastases-cancer-chemotherapy-2115512/
-
MM, I asked my MO if my stromal TILs had been tested on my biopsy... and they were not.
I think with TNBC the first line chemos are basically the same for anyone. That probably needs more refinement as these various markers are identified.
-
... our recent live webinar, Precision Medicine in Oncology: No Two Tumors Alike.
Please feel free to view the event on demand, on your schedule.
Thank you,
The Scientist Webinars Team
https://globalmeet.webcasts.com/viewer/event.jsp?ei=1249185&tp_key=ab4b574682
{Hope this link works for others. It works for me. Interesting web presentation.}
-
Cancer Trials Often Hinge on Fragile Data
Handful of outcomes represent difference between positive, negative results
Major positive clinical trials in oncology frequently hung by a statistical thread representing a handful of outcomes, according to a statistical fragility analysis.
Publication of the study followed a recent call to "retire statistical significance" in favor of confidence intervals. Acknowledging that confidence intervals are no panacea, the authors argued that eliminating P values as a kind of Holy Grail of clinical trial outcomes would help put an end to unfounded hype and dismissal of potentially crucial effects.
{A brief, rather technical, but interesting discussion of the data behind clinical trials and drug approval.}
Primary Source
The Lancet Oncology
-
China's Churning Out Revolutionary Cancer Drugs Much Cheaper Than the U.S.
-
Just a wee note, ACE’s also refer to “adverse childhood experiences, which is a high profile trauma informed approach to working with children. There may be some cross referencing!
-
marijen...will keep looking at the China options as promising. Thanks
-
New cause of cell aging discovered
Findings have huge implications for cancer and age-related health conditions
- Date:
- July 25, 2019
- Source:
- University of Southern California
- Summary:
- New research could be key to our understanding of how the aging process works. The findings potentially pave the way for better cancer treatments and revolutionary new drugs that could vastly improve human health in the twilight years.
https://www.sciencedaily.com/releases/2019/07/190725151018.htm
-
MRI Screening Finds More Breast Cancers, but at What Cost?
Even breast cancer survivors may find it tough to sort out benefits and harms
Use of MRI to follow women with a previous history of breast cancer detected more cancers than mammography, but at a cost of significantly more biopsies, researchers reported.
While the cancer detection rate was higher for breast MRI compared with mammography alone (10.8 vs 8.2 per 1,000 examinations), the breast MRI biopsy rate was more than two-fold greater (10.1% vs 4.0%)
For women with a personal history of breast cancer, "the potential benefits and harms, specifically the effect of increased biopsies, should be carefully considered when incorporating breast MRI into surveillance imaging strategies,"
National recommendations lack consensus...
"...the radiologic interpretation of mammography does not appear to miss more second cancer events that would become clinically detectable during the screening interval of 12 months compared with the radiologic interpretation of breast MRI,"
"...it's really important when policymakers are thinking about new surveillance strategies that they consider how these comparisons are made, and that while it might be appropriate for some women to get a breast MRI, we must also consider how often to use mammography in finding second breast cancers," Wernli said. "Right now women are recommended to get a mammogram annually after the diagnosis of breast cancer," adding that, when looking at surveillance strategies, it may be appropriate to start thinking about shortening surveillance intervals for these women, rather than adding additional tests.
{The article includes an interesting discussion of study methodologies.}
Primary Source: Radiology
Source Reference: Wernli K, et al "Surveillance Breast MRI and Mammography: Comparison in Women with a Personal History of Breast Cancer" Radiology 2019; DOI: 10.1148/radiol.2019182475.Secondary Source: Radiology
Source Reference: Newell MS "Risk versus Benefit of Surveillance MRI: A Sticky Wicket" Radiology 2019;292:319-320.
-
I am pro-choice on breast cancer screening! Let me decide, it’s my body.
-
For breasts that aren't dense, more frequent mammography might be the key. For dense breasts, mammography might not be enough. My tumor wasn't visible by mammogram. What good would it do me to have a hundred mammograms, none of which could show my tumor?
-
I agree with Marijen. My choice. In 40 years with dense breasts, I never had a yearly mammogram that I wasn't called back for "further studies", which always included an ultrasound.
-
The article on MRI's didn't mention 3D mammograms. From all quarters, those seemed to be widely praised. Perhaps they help bridge the gap. Mammography did not find my lump. I did. Plus, my breasts are extremely dense. So I do them annually but I've never put that much stock in them. For some reason, it doesn't bother me that much that I don't view them as being terribly effective for me. Maybe it should.
-
Low doses of radiation promote cancer-capable cells: New research in mice helps to understand the risks around exposure to low doses of radiation, such as CT scans and X-rays -- ScienceDaily
https://www.sciencedaily.com/releases/2019/07/1907... -
Role of MEL-18 Amplification in Anti-HER2 Therapy of Breast Cancer
Resistance to HER2-targeted therapy with trastuzumab still remains a major challenge in HER2-amplified tumors. Here we investigated the potential role of MEL-18, a polycomb group gene, as a novel prognostic marker for trastuzumab resistance in HER2-positive (HER2+) breast cancer.
Conclusion: MEL-18 serves to prevent ligand-dependent ErbB heterodimerization and trastuzumab resistance, suggesting MEL-18amplification as a novel biomarker for HER2+ breast cancer.
https://www.medscape.com/viewarticle/915108?src=wnl_edit_tpal&uac=210289DR&impID=2044252&faf=1
J Natl Cancer Inst. 2019;111(6):609-619.
{full journal article available}
-
BMI and Hormone Receptor Status Influence Recurrence Risk in Patients With HER2+ Early Breast Cancer
- This retrospective study was designed to evaluate the impact of BMI and hormone receptor (HR) status on outcomes among patients with HER2-positive early breast cancer. Neither HR status nor BMI status alone was associated with recurrence. Among patients with a high BMI, HR-negative status was associated with an increased risk for recurrence.
- HR-negative patients and patients with BMI ≥25 may benefit from escalation approaches, whereas HR-positive patients and those with BMI <25 may benefit from a shorter duration of anti-HER2 adjuvant treatment.
CONCLUSIONS: Our real-life data highlight a different risk of eBC recurrence after grouping patients by HR status and BMI. These results might help clinicians to identify correct treatment strategies. HR-/BMI≥25 patients might benefit from escalation approaches, while HR+/BMI<25 ones might be eligible for a shorter duration of adjuvant treatment with anti HER-2 agents.
https://www.practiceupdate.com/C/86607/56?elsca1=emc_enews_topic-alert
https://www.clinical-breast-cancer.com/article/S1526-8209(19)30081-3/pdf
-
{Received the following from a colleague: }
HHS {the U.S. Health and Human Services Department} is revising its definition of Health Literacy and they are looking for public comments. Currently, health literacy is defined as:
"The capacity of individuals to obtain, process, and understand basic health information and services needed to make appropriate health decisions"
However, the current definition focuses only on patient's knowledge or ability to understand. The proposed new definition would recognize that health literacy is a two-way communication. So, it is not just how information is understood but how well it is written and communicated to patients to allow them to ask questions and to make informed health care decisions. This is an important change to make health care more patient centered.
The following information was prepared by Helene M. Epstein, who has a link to a draft letter that can be slightly modified and be submitted:
{I noted a few typo's on this web page that you may wish to correct if you rely on the information when commenting.}
I hope many of you will consider to submit your comments. The deadline to respond to this Federal Register is August 5:
-
Drug makers to pay $70 million over deals to keep cheap generics off the market
The settlements will also bar the companies from entering into similar deals.
Read in Ars Technica: https://apple.news/A3JG-c8XBQ4SOWe2uio_XbQ -
The big drug makers wont be able to keep cheap generics off the market once 3D becomes a reality. Hypothetically, people could print their own drugs at home.
This report focuses on 3D Printed Drugs volume and value at global level, regional level and company level. From a global perspective, this report represents overall 3D Printed Drugs market size by analyzing historical data and future prospect. Regionally, this report focuses on several key regions: North America, Europe, China and Japan.
-
Article | Published: 08 July 2019
Connecting blood and intratumoral Tregcell activity in predicting future relapse in breast cancer
Abstract
Regulatory T (Treg) cells play a major role in the development of an immunosuppressive tumor microenvironment. The origin of intratumoral Treg cells and their relationship with peripheral blood Treg cells remain unclear. Treg cells consist of at least three functionally distinct subpopulations. Here we show that peripheral blood CD45RA−FOXP3hi Treg cells (Treg II cells) are phenotypically closest to intratumoral Treg cells, including in their expression of CCR8. Analyses of T cell antigen receptor repertoires further support the hypothesis that intratumoral Treg cells may originate primarily from peripheral blood Treg II cells. Moreover, the signaling responsiveness of peripheral blood Treg II cells to immunosuppressive, T helper type 1 (TH1) and T helper type 2 (TH2) cytokines reflects intratumoral immunosuppressive potential, and predicts future relapse in two independent cohorts of patients with breast cancer. Together, our findings give important insights into the relationship between peripheral blood Treg cells and intratumoral Treg cells, and highlight cytokine signaling responsiveness as a key determinant of intratumoral immunosuppressive potential and clinical outcome.
https://www.medicalnewstoday.com/articles/325702.p... -
New 'don't eat me' signal may provide basis for cancer therapies
...Lastly, they implanted human breast cancer cells in mice. When CD24 signaling was blocked, the mice's scavenger macrophages of the immune system attacked the cancer.
Of particular interest was the discovery that ovarian and triple-negative breast cancer, both of which are very hard to treat, were highly affected by blocking the CD24 signaling. "This may be a vulnerability for those very dangerous cancers," Barkal said...
"There are probably many major and minor 'don't eat me' signals, and CD24 seems to be one of the major ones," Barkal said.
The researchers now hope that therapies to block CD24 signaling will follow in the footsteps of anti-CD47 therapies, being tested first for safety in preclinical trials, followed by safety and efficacy clinical trials in humans.
https://medicalxpress.com/news/2019-07-dont-basis-cancer-therapies.html
-
For those of us who suffer hot flashes, this would be fantastic
... the Reon Pocket ... slips into a pouch in a special T-shirt. The stealthy device doesn't condition the air as such. Rather, it sits at the base of your neck and uses the Peltier effect (where heat is absorbed or emitted when you pass an electrical current across a junction) to either lower your temperature by 23 [degrees Fahrenheit] or raise it by 14 [degrees Fahrenheit], all without bulk or noise. You could wear a stuffy business outfit on a hot day and avoid looking like you've just stepped out of a sauna.
-
AI takes advantage of existing mammography scans to make a cancer diagnosis
Though it's a well-established fact that mammographies (mammograms) reduce breast cancer mortality rates, the high proportion of false-positive recalls associated with such screenings has accelerated development of AI-driven systems from IBM, MIT's Computer Science and Artificial Intelligence Laboratory, and others. But these aren't perfect, either, because most models operate on a single screening exam.
This shortcoming motivated a team of researchers at New York University's Center for Data Science and Department of Radiology to propose a machine learning framework that takes advantage of prior exams in making a diagnosis ("Screening Mammogram Classification with Prior Exams "). They say that in preliminary tests, it reduced the error rate of the baseline and achieved an area under the curve (a metric indicating performance at all classification thresholds) of 0.8664 for predicting malignancy in a screening population.
-
Liquid biopsy chip snares circulating tumor cells in blood drops from cancer patients
Researchers at Worcester Polytechnic Institute (WPI) have developed a chip made of carbon nanotubes that can capture circulating tumor cells (CTCs) of all sizes and types, and can do so with far greater sensitivity than existing technologies. The unique design of the device makes it possible to easily identify and even culture the captured cells, which could make it possible to detect early-stage tumors, predict the course of a cancer, and monitor the effects of therapy.
https://www.sciencedaily.com/releases/2019/07/190731114158.htm
-
Integrated Analysis of TP53 Gene and Pathway Alterations in The Cancer Genome Atlas: Cell Reports
Highlights
- •TP53 mutation effects analyzed by five data platforms in 32 cancers/10,225 patients
- •More than 91% of cancers with TP53 mutations show loss of both functional TP53alleles
- •TP53 mutation affects genomic stability, global RNA, miRNA, and protein expression
- •Mutant p53 RNA expression signature helps prognostic predictions in 11 cancer types
https://www.medicalnewstoday.com/articles/325930.p... -
Leukemia Survivors Share How Cancer Affected Their Mental Health | Tell A Stranger
We invited two strangers to tell their cancer survival story. How did cancer impact their mental health?
{Not BC, but some will relate to these cancer experiences and the cathartic nature of sharing one's story.}
-
UC researchers unlock cancer cells' feeding mechanism, central to tumor growth
The findings could lead to new treatments by blocking tumor growth at its roots
Credit: Colleen Kelley / UC Creative Services
CINCINNATI–An international team led by researchers from the University of Cincinnati and Japan's Keio and Hiroshima universities has discovered the energy production mechanism of cancerous cells that drives the growth of the nucleolus and causes tumors to rapidly multiply.
The findings, published Aug. 1 in the journal Nature Cell Biology, could lead to the development of new cancer treatments that would stop tumor growth by cutting the energy supply to the nucleolus.
"The nucleolus is the 'eye' of the cancer storm that ravages patients' bodies. Being able to control the eye would be a true game-changer in cancer treatment," said Atsuo Sasaki, PhD, associate professor at the UC College of Medicine and one of the research team's lead investigators.
The nucleolus, located near the center of the nucleus, produces ribosomes. The discovery that cancerous cells have enlarged nucleoli occurred over 100 years ago, and studies have since shown that nucleolus enlargement results in significant ribosome increases, propelling protein synthesis to mass produce cancer cells, according to Sasaki. But, exactly how the nucleolus produces a massive amount of ribosome in cancerous cells has largely remained a mystery, he says.
"Nucleolus enlargement is a telltale sign of cancer, and its size has long been used as a yardstick to determine how advanced cancer is in patients," says Sasaki. "Now, our research team knows that the nucleolus quickly expands by devouring Guanosine Triphosphate, or GTP, a nucleotide and one of the building blocks needed for to create RNA, which is prevalent in cancerous cells."
"We were surprised to find out that among all types of energy that could be used for cell growth, it's GTP that spikes and plays the most crucial role in ribosome increases that are associated with nucleolus enlargement in cancer cells. We knew right away that this was a substantial discovery that would require a sweeping range of expertise to understand what it truly meant," Sasaki adds.
Sasaki says researchers saw an elevated level of inosine monophosphate dehydrogenase (IMPDH) in cancer cells, which accelerates GTP production and in turn fuels nucleolus growth. This is a major step toward solving the mystery surrounding nucleolus growth in cancer cells, he says.
To conduct the research, the multidisciplinary team zeroed in on the energy production pathways in malignant brain tumors and glioblastoma, the deadliest type of brain cancer, in animal models, followed by cohort studies for human specimens. The results showed a significant increase of GTP, which is a form of energy, in glioblastoma. Experts took a deeper look at brain tumor cells and determined that the significantly elevated level of IMPDH in cancer cells accelerates GTP production.
The close relationship between IMPDH and the nucleolus was discovered and prompted Sasaki's team to develop a new method of metabolic analysis, which enabled researchers to obtain critical data for demonstrating that GTP produced from IMPDH activities is used for the nucleolus's ribosome synthesis; this led to the discovery of a clear correlation between the suppression of glioblastoma cell growth and IMPDH inhibition, which prolonged animal models' lives.
"Thanks to our multinational cross-disciplinary collaboration and the team's hard work, we were able to unlock the mechanism through which cancerous cells hijack GTP metabolism to take control over the nucleoli. We are excited to continue our research on GTP for the development of therapies to annihilate the 'eye of cancer' in patients," Sasaki says.
###
Co-collaborators on the study include Tomoyoshi Soga, PhD, Hideyuki Saya, MD, PhD, and Makoto Suematsu, MD, PhD, all of Keio University; Ralph DeBerardinis, MD, PhD, and Robert Bachoo, MD, PhD, both of UT Southwestern; Wataru Yasui, MD, PhD, Hiroshima University; Ichiro Nakano, MD, PhD, University of Alabama; Hiroaki Wakimoto, MD, PhD, Harvard Medical School; William Young, PhD, UCLA; Craig Horbinski, MD, PhD, Northwestern University; Risa Kawaguchi, PhD, National Institute of Advanced Industrial Science and Technology of Japan; and Ingrid Grummt, PhD, and Holger Bierhoff, PhD, of the German Cancer Research Center.
The work is supported in-part by a UC College of Medicine Research Innovation grant, Molecular Therapeutics Program UC-Brain Tumor Center grant, Mayfield Education and Research Foundation grant, Marlene Harris Ride Cincinnati grant, American Brain Tumor Association Discovery Grant, B*Cured research grant, Ohio Cancer Research grant and National Institutes of Health grants R21NS100077 and R01NS089815 (ATS).
Media Contact
Katie Pence
katie.pence@uc.eduRelated Journal Article
http://dx.doi.org/10.1038/s41556-019-0363-9
-
Individualized Prediction of Survival Benefit From Post-Mastectomy Radiotherapy for Patients With Breast Cancer With One to Three Positive Axillary Lymph Nodes
- This analysis of the SEER database was conducted to develop a nomogram for prediction of the survival benefit from post-mastectomy radiotherapy among patients with breast cancer and one to three positive axillary lymph nodes. Independent predictors of survival were age at diagnosis, tumor grade, size, ER/PR status, and the number of positive nodes.
- The nomogram showed high accuracy for the prediction of survival at 5 and 10 years.
Conclusion: Besides the number of involved nodes, extra variables existed as predictors of survival outcomes in this cohort; therefore, the recommendation of PMRT or no PMRT requires comprehensive consideration. This clinically validated nomogram provided a useful tool that could aid decision making by estimating DSS and OS benefits from PMRT, useful in predicting 5- and 10-year DSS and OS for patients with one to three positive nodes after mastectomy.
https://www.practiceupdate.com/C/86890/56
http://theoncologist.alphamedpress.org/content/early/2019/07/17/theoncologist.2019-0124
doi:10.1634/theoncologist.2019-0124
-
Liquid Biopsy ID's Early Breast Ca Relapse
ctDNA in plasma samples detected return of disease 10.7 months earlier
Circulating tumor DNA (ctDNA) in ... blood samples following standard treatment for early-stage breast cancer detected patients' relapse nearly 11 months before clinical symptoms, a prospective U.K. study found.
At a median follow-up of close to 3 years, relapse-free survival was significantly worse for these early-stage patients when positive ctDNA was detected during post-treatment visits...In the cohort of 101 women with somatic mutations, relapse-free survival was also worse for those with positive ctDNA prior to treatment initiation...
...detection of ctDNA preceded clinical relapse by 10.7 months. "We hope that by identifying relapse much earlier we will be able to treat it much more effectively than we can do now, perhaps even prevent some people from relapsing... we will now need clinical trials to assess whether we can use these blood tests to improve patient outcome." the first of these studies have been launched and that plans for larger studies are in the works. The current study was conducted from 2011 to 2016 at five centers in the U.K....
Primary Source
JAMA Oncology
Source Reference: Garcia-Murillas I, et al "Assessment of molecular relapse detection in early-stage breast cancer" JAMA Oncol 2019; DOI: 10.1001/jamaoncol.2019.1838.Secondary Source
JAMA Oncology
Source Reference: Karthikeyan S, Park BH "Circulating tumor DNA as a marker for disease relapse in early-stage breast cancer -- Bad blood" DOI: 10.1001/jamaoncol.2019.2047.
-
Early stage breast cancer and metastasis:
https://bmccancer.biomedcentral.com/articles/10.1186/s12885-019-5949-x
Rossano Lattanzio1,2*† , Manuela Iezzi2,3†, Gianluca Sala1,2, Nicola Tinari1,2, Marco Falasca4, Saverio Alberti5, Simonetta Buglioni6, Marcella Mottolese6, Letizia Perracchio6, Pier Giorgio Natali2 and Mauro Piantelli2
Abstract
Background: Phospholipase Cγ1 (PLCγ1) is highly expressed in human tumours. Our previous studies reported that both stable and inducible PLCγ1 down-regulation can inhibit formation of breast-cancer-derived experimental lung metastasis. Further, high expression of PLCγ1 and its constitutively activated forms (i.e., PLCγ1-pY1253, PLCγ1-pY783) is associated with worse clinical outcome in terms of incidence of distant metastases, but not of local relapse in T1- T2, N0 breast cancer patients.
Methods: In the present retrospective study, we analysed the prognostic role of PLCγ1 in early breast cancer patients stratified according to the St. Gallen criteria and to their menopausal status. PLCγ1-pY1253 and PLCγ1-pY783 protein expression levels were determined by immunohistochemistry on tissue microarrays, and were correlated with patients' clinical data, using univariate and multivariate statistical analyses.
Results: In our series, the prognostic value of PLCγ1 overexpression was restricted to Luminal type tumours. From multivariate analyses, pY1253-PLCγ1High was an independent prognostic factor only in postmenopausal patients with Luminal-B tumours (hazard ratio [HR], 2.4; 95% confidence interval [CI], 1.1–5.3; P = 0.034). Conversely, PLCγ1-pY783High was a remarkably strong risk factor (HR, 20.1; 95% CI, 2.2–178.4; P = 0.003) for pre/perimenopausal patients with Luminal-A tumours.
Conclusions: PLCγ1 overexpression is a strong predictive surrogate marker of development of metastases in early Luminal-A and -B breast cancer patients, being able to discriminate patients with high and low risk of metastases. Therefore, targeting the PLCγ1 pathway can be considered of potential benefit for prevention of metastatic disease.
Keywords: Breast cancer, Phospholipase Cγ1, Prognosis, Luminal subtypes, Menopausal status
-
Factors Associated With Lymphedema in Women With Node-Positive Breast Cancer Treated With Neoadjuvant Chemotherapy and Axillary Dissection
- The authors of this cohort study of 486 patients with node-positive breast cancer evaluated factors associated with lymphedema after neoadjuvant chemotherapy and axillary lymph node dissection. High BMI (HR, 1.04) and duration of neoadjuvant chemotherapy of >144 days (HR, 1.48) were associated with lymphedema symptoms. Duration of neoadjuvant chemotherapy of >144 days was associated with a 20% limb volume increase (HR, 1.79). Both the removal of ≥30 nodes (HR, 1.70) and a higher number of positive nodes (HR, 1.03) were associated with a 10% limb volume increase. There was a significant association between obesity and lymphedema symptoms.
- Obese women and those with a long duration of neoadjuvant chemotherapy may obtain the most benefit from enhanced prospective lymphedema surveillance.
doi:10.1001/jamasurg.2019.1742 -
Lumpie - have you run across any articles describing lymphedema on the opposite side? Both the lymphedema therapist and oncologist think it is very unusual, but it seems to be happening to me. I noticed swelling in the opposite arm about 1 1/2 months ago. The oncologist has put in an order for imagery of the chest. I do not know if they image axilla as well.
2009 ER+ left breast. 52 yrs. Lumpectomy, Sentinel node removal, negative. Radiation 6 weeks, tamoxifen 5 years. Dense lumpy left breast, normal right. Acupuncture offered at facility as part of integrative medicine. It really helped with anxiety/stress during radiation treatment.
2016 ER+ left breast. Probably a new cancer, but unknown. 4 rounds TC Aug-Oct 2016, Bi-lateral (my choice) Nov 2016, no reconstruction. 2 sentinel nodes remove, negative. Cold Capping using Chemo Cold Caps (DIGNICAP not available). Anastrozole 1 mg starting May 2017. Joint issues noticed immediately. Stopped Anastrozole after 3-4 months due to joint stiffness in. After several months of no AIs, fingers were feeling better. Started tamoxifen March 2018
10/2018 noticed stiffness and some trigger finger again. Was eating meat a lot more (daily) than normal. Usually 1-2 /wk. Have cut way back on the meat, seems to help, but one finger still very prone to trigger finger. Trigger finger seemed to be getting better, but now 4/2019 seems worse, is it the break from added turmeric to meals?
7/19/2019 - swelling in R-arm, opposite side from where lymph nodes removed. Noticed 6/18/2019. Could have been swelling earlier but wearing long sleeves. Trip to urgent care. They did ultrasound, concerned that there might be a clot, there was not. Started seeing lymphatic therapist 7/2/2019. Wearing sleeve and glove (loaners), went in for a fitting 8/2/2019. Sometimes therapists wraps affected arm, but hard to do anything, like wash hands, selef-massage.
-
BlueGirlRedState:
I did a quick search and located this one. It's a bit old, but there doesn't seem to be much on the topic. It probably affects a relatively small subset of patients. Trunkal lymphedema is another variation that affects many of us. I'll keep my eyes peeled for more. Good luck!
Lymphatic abnormalities in the normal contralateral arms of subjects with breast cancer-related lymphedema as assessed by near-infrared fluorescent imaging
Published online 2012 May 3
Abstract
Current treatment of unilateral breast cancer-related lymphedema (BCRL) is only directed to the afflicted arm. Near-infrared fluorescent imaging (NIRF) of arm lymphatic vessel architecture and function in BCRL and control subjects revealed a trend of increased lymphatic abnormalities in both the afflicted and unafflicted arms with increasing time after lymphedema onset. These pilot results show that BCRL may progress to affect the clinically "normal" arm, and suggest that cancer-related lymphedema may become a systemic, rather than local, malady. These findings support further study to understand the etiology of cancer-related lymphedema and lead to better diagnostics and therapeutics directed to the systemic lymphatic system.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3370966/
doi: 10.1364/BOE.3.001256
-
This one is really old but does mention contralateral lymphedema...
Lymphedema in a cohort of breast carcinoma survivors 20 years after diagnosis
First published: 27 September 2001
BACKGROUND
To the authors' knowledge, there are no long‐term cohort studies of lymphedema, despite the substantial morbidity of arm swelling. The goal of this study was to identify prevalence of breast carcinoma–related lymphedema, time of onset, and associated predictive factors.CONCLUSIONS
This defined cohort, treated by axillary dissection 20 years ago, documents the high prevalence of lymphedema and its time course. Two significantly associated factors, both potentially controllable, are identified. The current study provides further support for treatments that limit lymph node dissection. The authors are prospectively evaluating patients undergoing sentinel lymph node biopsy.
https://doi.org/10.1002/1097-0142(20010915)92:6<1368::AID-CNCR1459>3.0.CO;2-9
-
Local Tissue Water in At-Risk and Contralateral Forearms of Women with and without Breast Cancer Treatment-Related Lymphedema
Published Online:24 Sep 2009
Background: Quantitative measurements to help detect incipient or latent lymphedema in patients at risk for breast cancer treatment-related lymphedema (BCRL) are potentially useful supplements to clinical assessments. Suitable measurements for routine use include arm volumes, arm bioimpedance, and local tissue water (LTW) determined from the tissue dielectric constant (TDC). Because BCRL initially develops in skin and subcutis, measures that include whole arms may not be optimally sensitive for detecting the earliest changes. Thus, there is also a need for a local measurement in which tissues most likely to demonstrate early lymphedematous changes can be more selectively assessed. The TDC method satisfies this criterion. Our goal was to use this method to compare arm-to-arm differences in LTW within and among women grouped as healthy normal (HN), diagnosed with breast cancer (BC), but prior to surgery and established unilateral lymphedema (LE).
Conclusions: The findings indicate that LTW of at-risk arms is not affected by breast cancer and that lymphedema does not significantly affect LTW of contralateral arms as measured with the TDC method. Further, based on the standard deviation of measured arm ratios, an at-risk/contralateral TDC ratio of 1.26 is suggested as a possible threshold for detecting preclinical or latent lymphedema.
https://www.liebertpub.com/doi/abs/10.1089/lrb.2009.0008
https://doi.org/10.1089/lrb.2009.0008
{May require subscription to access full article.}
-
BlueGirlRedState: It also occurs to me that if you have had a bilateral, even if they didn't (intentionally) biopsy or dissect lymph nodes on the contralateral/"good" side, there may have been intra/post operative injury to tissue and/or to the lymphatic system that could contribute to lymphedema.
-
Compound found in red wine opens door for new treatments for depression, anxiety
Resveratrol, found in grape skin, shuts down depression-causing enzyme in brain
- Date:
- July 29, 2019
- Source:
- University at Buffalo
- Summary:
- A new study has revealed that the plant compound resveratrol, which is found in red wine, displays anti-stress effects by blocking the expression of an enzyme related to the control of stress in the brain.
- https://www.sciencedaily.com/releases/2019/07/190729094553.htm
- http://www.buffalo.edu/news/releases/2019/07/032.html
- {Not strictly BC but potentially related to SE's. As the article notes, consumption of alcohol carries various health risks, including addiction.}
- Adding reference for journal article:
- The antidepressant- and anxiolytic-like effects of resveratrol: Involvement of phosphodiesterase-4D inhibition
-
The Prognostic Significance of Preoperative Tumor Marker Elevation in Breast Cancer Patients
- The authors of this retrospective study evaluated the prognostic significance of preoperative elevations of carcinoembryonic antigen (CEA) and cancer antigen 15-3 (CA15-3) levels in 149,238 patients with breast cancer in the Korean Breast Cancer Society Registry database. Preoperative CA 15-3 and CEA elevations had varying prognostic value according to breast cancer subtype. In patients with luminal A subtype, the CA 15-3- and CEA-elevated group had a hazard ratio of 2.14, while, in the group with luminal B subtype, the hazard ratio was 3.99 compared with patients with normal levels. In patients with the HER2 subtype, an elevated CEA level was the only independent prognostic factor. Neither CEA nor CA15-3 was a significant prognostic factor for overall survival in patients with triple-negative disease.
- Preoperative CEA and CA15-3 levels showed varying prognostic ability according to breast cancer subtype. Preoperative CA15-3 and CEA elevation are significant prognostic factors for luminal breast cancer, but they were not significant factors for TNBC
- These findings suggest the importance of careful surveillance in patients with luminal breast cancer and high preoperative elevation of tumor markers.
-
Surviving Cancer Costs
One in 4 cancer survivors struggles to pay medical bills and 1 in 3 worries about medical bills, according to a CDC report.
{Brief commentary on the financial toxicity of cancer and link to CDC study on the topic.}
https://jamanetwork.com/journals/jama/fullarticle/2738563
doi:10.1001/jama.2019.9666
https://www.cdc.gov/mmwr/volumes/68/wr/mm6822a2.htm?s_cid=mm6822a2_w
-
Annual Out-of-Pocket Expenditures and Financial Hardship Among Cancer Survivors Aged 18–64 Years — United States, 2011–2016
What is already known about this topic?
Many cancer survivors face substantial economic burden resulting from cancer and its treatment.
What is added by this report?
On average, cancer survivors had significantly higher annual out-of-pocket medical expenditures than did persons without a cancer history. Overall, 25% of survivors reported problems paying medical bills, and 33% reported worry about medical bills. Financial hardship was more common among the uninsured than among those with insurance coverage.
What are the implications for public health practice?
The population of cancer survivors is growing, and many struggle to pay for medical care. Evidence-based, sustainable strategies by providers, practices, and payers to reduce out-of-pocket costs could be an important component of high-quality cancer care.
{CDC report. See full article on CDC page.}
https://www.cdc.gov/mmwr/volumes/68/wr/mm6822a2.htm?s_cid=mm6822a2_w
citation for this article: Ekwueme DU, Zhao J, Rim SH, et al. Annual Out-of-Pocket Expenditures and Financial Hardship Among Cancer Survivors Aged 18–64 Years — United States, 2011–2016. MMWR Morb Mortal Wkly Rep 2019;68:494–499. DOI: http://dx.doi.org/10.15585/mmwr.mm6822a2external icon
-
CLEOPATRA End-of-Study Analysis in Metastatic Breast Cancer: 37% Alive at 8 Years
The end-of-study analysis of the landmark CLEOPATRA trial shows that 37% of patients with HER2-positive metastatic breast cancer are still alive at 8 years... The unprecedented overall survival improvement earlier shown with a first-line regimen of pertuzumab, trastuzumab, and docetaxel was maintained after an additional 4 years of long-term follow-up, as were the safety and cardiac safety profiles, she reported.
"These are 'knock-your-socks-off' data! There's never been another study in metastatic breast cancer to show anywhere near this kind of survival benefit with this length of follow-up," "As of November 2018, the data cutoff, 59 patients are still on study and have not progressed. It's a possibility—though I hesitate to use the word—that these patients are cured," she commented.
"These are spectacular results. Over one-third of patients who would have died years ago without HER2-targeted treatment are now alive at 8 years. The question now is when to stop treatment?" Dr. Swain said. "As of November, many patients were still on HER2-targeted treatment in this trial, and we see the same thing in our clinical practices. Patients often don't want to stop treatment."
-
Standard HER2 Regimen Still Going Strong
Seven-year relapse-free interval of 97.5% with paclitaxel-trastuzumab
Long-term follow-up in a large phase II trial of early HER2-positive breast cancer showed high rates of disease control and survival with a longstanding standard regimen.
Treatment with adjuvant paclitaxel and trastuzumab (Herceptin) led to a 7-year disease-free survival (DFS) of 93% and overall survival (OS) of 95%. Additionally, 97.5% of the 410 patients remained relapse-free for at least 7 years...
"...I think we're learning there might be more potent anti-HER2 therapies that are emerging, particularly antibody-drug conjugates, that might be able to provide highly effective therapy and potentially replace chemotherapy and trastuzumab."
"I'm hoping that the field continues to evolve, because I think the goal is to provide the right amount of therapy to the right patient. We'd like to avoid overtreating patients, particularly with these lower-risk tumors,"
Primary Source
Journal of Clinical Oncology
-
Great news for stage I patients.
-
I'll take it!!
-
Mine didn't show up on anything EXCEPT a MRI and by that time it was 6 cm because I have dense breasts and it couldn't be seen on regular mammogram. I never had a recommendation from a radiologist to have any follow up for all of the years I was having mammograms and mentioning in the "normal" results that I had dense breasts. It was only diagnosed (finally) because they saw two enlarged nodes on the mammo. It was only then that I had the MRI. If I had known then what I know now about dense breasts I would have insisted on a MRI at least every couple of years. BS said it could have been there for 10 years.
-
Gussy: Yeah... I am not sure which article you are referencing but I am with you. The dense breasts thing is a controversial issue. Which I don't really understand. But that is probably because I have strong opinions. I believe that we have a "right to know" and that our caregivers don't have a right to withhold information about our bodies and health status. If our caregivers don't believe that identified information is useful or that we might be confused about whether it presents a legitimate hazard to our health, then absolutely, they should share that information, counsel us and refer us to appropriate educational tools if needed. That is their professional opinion and that is why we consult them. From many quarters, however, it is argued that this information should be withheld because patients will be confused or are not competent to use it in making decisions about how to manage their health. Withholding information is always a bad idea. Education is always a good idea. Education has the misfortune to be expensive and time consuming.
-
Lumpie, Amen!
-
Ditto on the Amen.
I think a lot of us are on this sight, not just for emotional support, but also for bits of information that we suspect out doctors don’t share.
-
How Are States Dealing With Challenges Facing Patients With Cancer?
High costs of care, particularly for prescription drugs, dominated a discussion of cancer care at the state level during the June 27, 2019, National Comprehensive Cancer Network Policy Summit in Washington, DC.
July 31, 2019
-
Cost of Breast Cancer Surgery Influences Many Women's Treatment
But doctors seldom discuss financial differences between similarly effective treatments
Even among well-educated women with health insurance coverage, a significant proportion said the costs of cancer treatment influenced the type of surgery they chose for breast cancer treatment, a study led by the Duke Cancer Institute found.
"While other side effects of surgical choice are routinely discussed with their physicians, the potential for financial harm is not explicitly addressed, including both the out-of-pocket payments and lost productivity for patients and their families," she said. "Our study suggests this should change."
-
-
Long-term effects of moderate versus high durations of aerobic exercise on biomarkers of breast cancer risk: Follow-up to a randomized controlled trial | Cancer Epidemiology, Biomarkers & Prevention
http://cebp.aacrjournals.org/content/early/2019/08... -
Wanderingneedle: Thanks for the link to the LA Times article. Sharing the general theme:
"...we published a research letter in JAMA Internal Medicine summarizing industry payments to the 53 physicians who direct major academic cancer centers across the United States. These are the nation's most prominent cancer centers, those designated by the National Cancer Institute in recognition of their scientific leadership.... About a third of all directors...{received industry payments in 2017} above {$5,000} – typically receiving payments for research and consulting. A few were well above it (one had payments exceeding $2 million)."
The data are public and available to anyone with an internet connection.
{The article goes on to discuss the conflicts of interest that this situation creates given that these centers conduct clinical trials.}
"The public has an interest in the unbiased evaluation of new products....Industry-funded evaluations are more likely to reach pro-industry conclusions."
https://www.latimes.com/opinion/story/2019-08-05/directors-cancer-centers-money-drug-companies
https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2740204
doi:10.1001/jamainternmed.2019.3098
-
Yes, I found one doctor who received over two hundred thousand dollars from drug companies and decided not to see him. You think they push the drugs they receive payments for? I do.
-
Shelligirl - that's what brought me here - trying to find answers that my doctors didn't share. Maybe that's a method they employ with purpose, but I don't think it works for some people.
-
Breast Cancer Navigation and Survivorship Care
- Interview with Lillie D Shockney RN, BS, MAS, ONN-CG
- Interview by Farzanna S Haffizulla MD, FACP, FAMWA
- {Many of you are familiar with Lillie D Shockney RN, BS, MAS, ONN-CG who is known for her pioneering work as a B.C. oncology nurse navigator. In this interview, she shares insight on her work.}
- https://www.practiceupdate.com/C/84565/56?elsca1=emc_enews_topic-alert
-
Not bc-specific...
Researchers have opened up a possible avenue for new cancer therapies that don't have the side effects that oftentimes accompany many current cancer treatments by identifying a protein modification that specifically supports proliferation and survival of tumor cells...
Researchers led by Franco and Oregon State undergraduate student Jeanine Pestoni found that schwannoma cells produce an oxidant and nitrating agent, peroxynitrite, which modifies an amino acid, tyrosine, in proteins.
When tyrosine becomes nitrated in specific proteins, an effect is the reprogramming of the tumor cells' metabolism, enabling them to proliferate...
"We are uncovering a completely new category of targets for the treatment of solid tumors, and not only tumors of the nervous system -- it may have broader implications for the treatment of several cancer types. We can go after proteins that usually aren't modified in normal cells; we can target those modified proteins with inhibitors that don't affect normal cells, hopefully developing a treatment with minimal side effects."
https://www.sciencedaily.com/releases/2019/08/190805155916.htm
Study referenced: Peroxynitrite supports a metabolic reprogramming in merlin-deficient Schwann cells and promotes cell survival. Journal of Biological Chemistry, 2019; 294 (30): 11354 DOI: 10.1074/jbc.RA118.007152
-
Spreading the word: Triage Cancer has a number of good educational resources related to cancer. They have a webinar on genetics and genomics coming up on 8/8. You can register for the webinar and watch pre-recorded webinars here:
-
Decreased CTCs/ctDNA Post-Chemo Prognostic in Advanced Breast Ca
Clearance of both associated with improved outcomes, largest prospective cohort assessing the two shows
New data from the French cohort COMET study, presented at the 2019 ASCO annual meeting, evaluated the role of circulating tumor cells (CTCs) and circulating tumor (ct) DNA in predicting patient outcome to first-line treatment...While more data are needed, this study suggests the feasibility and importance of CTC/ctDNA testing in guiding chemotherapy choices in breast cancer patients. Additionally, it highlights the need for further quantification of CTC/ctDNA to assess tumor response to treatment, and the need for use of both serum markers in the measurement of tumor aggressiveness.
Primary Source
Journal of Clinical Oncology
-
New Super-Sensitive Liquid Biopsy Test For Breast Cancer Described As Possible "Game-Changer"
A new blood test for tracking breast cancer in patients with early stage disease may enable physicians to more sensitively monitor patients, including looking at responses to treatment, tailoring treatments more effectively and preventing some invasive surgeries...
The research published today in Science Translational Medicine is a collaborative effort between the Translational Genomics Research Institute (TGen), an affiliate of City of Hope in California and the Mayo Clinic in Arizona and the Cancer Research UK Cambridge Institute.
The test called "TARDIS" (TArgeted DIgital Sequencing) has been suggested to be up to 100 times more sensitive than other existing blood-based cancer monitoring tests.
-
There Is Such Thing as a Too-High LVEF
Study suggests sweet spot and proposes fourth left ejection phenotype
Higher is not necessarily better when it comes to left ventricular ejection fraction (LVEF), according to a retrospective study.
Compared with an LVEF of 60-65%, both reduced and elevated LVEFs were associated with worse all-cause mortality that persisted after multivariable adjustment...
Primary Source
European Heart Journal
{Those of use who get regular echos may have wondered....}
-
Very interesting Lumpie, thanks! Met with Cardio on Monday and with exercise EF is up to 58% from a dip to 53% 🙂
-
I am due for my next echo. My last one put me in 55-60% range. I have been duen as low as 35% twice in my life. Both times I was removed from herceptin. I have bounced back every time. I dipped to 40% this two echos again but s changevin heart meds brought me back o do I am still on herceptin.
-
Lumpie, Thanks for posting the links about resveratrol. I followed the links and didn't see mention of how it was administered. Was it just through drinking red wine? or through supplements? Do you know? I guess I could email the researcher. I'm wondering if it might help my chemo brain side effects? I've been avoiding wine because it gives me unpleasant feelings the next morning--sort of like a hang over but after only a little bit--like 1/4 of a glass.
-
Study says antidepressant could inhibit breast cancer
Researchers from National Chiao Tung University (NCTU) and Taipei Medical University (TMU) yesterday said they discovered that the antidepressant bupropion can be used as an anti-metastasis drug for triple-negative breast cancer...
For the study, researchers used big data and artificial intelligence to analyze large-scale cancer gene expression maps, and designed regulatory networks for nearly 2,000 types of different kinds of membrane proteins in 15 types of cancer to explore the roles membrane proteins play in different cancers, and their importance, the NCTU team said.
http://www.taipeitimes.com/News/taiwan/archives/2019/08/09/2003720184
-
Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer
- This prospective, multicenter, sample collection study assessed the clinical validity of molecular relapse detection with circulating tumor DNA (ctDNA) in early-stage breast cancer. The primary endpoint was relapse-free survival. Detection of ctDNA during follow-up was associated with relapse (HR, 25.5; P<.001). Detection of ctDNA at diagnosis, prior to any treatment, was also associated with shorter relapse-free survival (HR, 5.8; P=.01). Detection of ctDNA had a median lead time of 10.7 months compared with clinical relapse and performed better in distant extracranial metastatic relapse (detected in 96%) versus brain-only metastasis (17%).
- These important findings suggest the potential for ctDNA in follow-up of early-stage breast cancer. Further studies to assess the potential for this information to guide adjuvant therapy are needed.
- Meaning The findings suggest that molecular relapse detection has high levels of clinical validity, and clinical trials of treatment initiated at molecular relapse without waiting for incurable metastatic disease to develop are needed.
doi:10.1001/jamaoncol.2019.1838 -
Book note: Healthcare Choices
5 Steps to Getting the Medical Care You Wand And Need
Author: Archelle Georgiou, MD
Published 2017
I skimmed this book. I found a section on pages 38 and 39 particularly helpful. The physician author discusses her recommended approach to decision making and taking action in the face of a diagnosis (or progression) that can feel "overwhelming"/frightening. {Perhaps after taking time to vent and grieve as needed} She recommends taking a "clinical" approach. She calls this the "CARES" model. These are the steps:
1) understand your Condition
2) know your Alternatives
3) Respect your preferences
4) Evaluate your options
5) Start taking action.
In my experience, once I have a defined a plan in which I have some confidence and can focus on executing the plan, I feel much better.
I thought this approach might be helpful for others.
ISBN: 978-1-4422-6033-7 (978-1-4422-6033-4 for the e-book)
-
Re: the LVEF, my MO told me early on that greater was not necessarily better--that too high means the heart is having to work too hard to circulate the blood.
-
I take resveratrol in capsule form.
-
aterry: Based on the discussion in the referenced articles and other things I have read, I believe that the resveratrol is extracted from the wine. And like santabarbarian says, I believe that it can be purchased in capsule form. When I did a search for "resveratrol capsules" many "opportunities" popped right up. I have heard about the alleged merits of resveratrol for decades so it is great to learn that it is being studied.
As with any supplement, care should be taken to try to identify a reputable purveyor. And it goes without saying that clearing such with your care providers is a good idea.
-
I don't find that I have posted this... but I have been getting loads of emails about this online cancer conference. Some of the speakers sound interesting. Unfortunately, I haven't had much time to watch. Dates are Aug 5-15. Maybe some presenters will be available via recorded video later...?
Here is the promo material:
LEARN FROM 40+ CANCER SURVIVORS, METAVIVORS, CAREGIVERS AND MEDICAL EXPERTS ABOUT DIAGNOSIS, TREATMENT AND THE AFTERMATH SO YOU CAN KEEP YOUR SPIRIT INTACT & SHARE YOUR TRIUMPH!
Join us for this free, virtual event and get your questions answered. Learn from women just like you as they share how they made decisions about treatment and discuss how the emotional effects of diagnosis impact them today.
This event brings together the best doctors, therapists, nonprofits, fashion brands, comedians, podcasters, survivors and metavivors teaching you how to get through diagnosis, treatment and the aftermath helping keep your mind and spirit intact!
There ARE so many awesome stories of TRUE WARRIORS SHARING TRIUMPH!
If you know someone dealing with a cancer diagnosis and the emotional aftermath, forward them this email and encourage them to Get Their Free Conference Pass:
https://conference.sharetriumph.com/joinThe conference also has a Facebook page:
-
BRCA Mutation, Preventive Surgery, and Osteoporosis
— Researchers advocate for increased hormone therapy for high-risk women
Bone health suffered in women with a BRCA mutation who underwent preventive oophorectomy, Canadian researchers reported.
Premenopausal women with the BRCA1 or BRCA2 mutation experienced a significant decline in bone mineral density (BMD) after undergoing prophylactic bilateral salpingo-oophorectomy...
"These pre-menopausal women looked a lot like post-menopausal women after a year following surgery,"
...use of hormonal therapy was able to offset most of the deleterious bone changes in both pre- and post-menopausal women after surgery.
"There are no standardized guidelines for the management of bone health in this population after surgery,"
"Given the important role of estrogen in maintaining various physiological functions, including bone health, this rate of hormone therapy use is far too low," the researchers stated, suggesting that the "mitigating effects" of hormone therapy use in this population should be noted in future clinical practice guidelines.
...suggested recommending enough calcium intake for this population, as well as engaging in weight-bearing exercise and exogenous hormone use for those for whom it is not contraindicated.
future studies with a longer follow-up period are needed to truly estimate the impact of prophylactic bilateral salpingo-oophorectomy on fracture risk in this high-risk population of women.
Primary Source
JAMA Network Open
-
Patients with cancer- or treatment-related fatiguemight want to check out Untire, a free fatigue management app available from England's National Health Service.
https://www.nhs.uk/apps-library/untire-beating-cancer-fatigue/
{I haven't tried this. Please share your expereince if you do.}
-
Validation of Microsatellite Instability Detection Using a Comprehensive Plasma-Based Genotyping Panel
Another liquid biopsy showed good correlation with tissue biopsy, this time for detection of microsatellite instability, which can influence treatment decisions for multiple types of cancer. (American Association for Cancer Research)
Conclusions: cfDNA-based MSI detection using Guardant360 is highly concordant with tissue-based testing, enabling highly accurate detection of MSI status concurrent with comprehensive genomic profiling and expanding access to immunotherapy for patients with advanced cancer for whom current testing practices are inadequate.
https://www.aacr.org/Newsroom/Pages/News-Release-Detail.aspx?ItemID=1328
https://clincancerres.aacrjournals.org/content/early/2019/08/02/1078-0432.CCR-19-1324#
DOI: 10.1158/1078-0432.CCR-19-1324
{Lots of breaking news on liquid biopsies. I don't believe that this one has been posted before.}
-
England's healthcare cost-effectiveness agency, NICE, also had a busy week, approving.....neratinib (Nerlynx) for certain patients with HER2-positive breast cancer...
-
New 'don't eat me' signal may provide basis for cancer therapies
Cancer cells are known to protect themselves using proteins that tell immune cells not to attack them. Stanford researchers have discovered a new "don't eat me" signal, and blocking it may make cancer cells vulnerable to attack by the immune system.
... they implanted human breast cancer cells in mice. When CD24 signaling was blocked, the mice's scavenger macrophages of the immune system attacked the cancer.
Of particular interest was the discovery that ovarian and triple-negative breast cancer, both of which are very hard to treat, were highly affected by blocking the CD24 signaling. "This may be a vulnerability for those very dangerous cancers,"
-
Association between meat consumption and risk of breast cancer: Findings from the Sister Study
Meat consumption has been postulated to increase the risk of breast cancer, but this association has not been consistently seen.
We examined the association between consumption of different types of meat, meat mutagens and incident invasive breast cancer .
In a substitution model with combined red meat and poultry consumption held constant, substituting poultry for red
meat was associated with decreased invasive breast cancer risk. No associations were observed for cooking practices, estimated heterocyclic amines or heme iron from red meat consumption with breast cancer risk. Red meat consumption may increase the risk of invasive breast cancer, whereas poultry consumption may be associated with reduced risk. Substituting poultry for red meat could reduce breast cancer risk.
{Cannot locate a DOI - sorrry}
-
Medicare to Cover Pricey Cancer Tx Nationwide
Ups reimbursement to 65% and allows for guideline-recommended off-label use
The Centers for Medicare & Medicaid Services (CMS) on Wednesday announced nationwide coverage of an exciting but also very expensive new cancer treatment -- chimeric antigen receptor (CAR) T-cell therapy -- for Medicare recipients with certain types of lymphoma and for any expanded indications down the round.
Prior to the decision, coverage for CAR-T therapy carried uncertainty and was decided by regional Medicare administrators.
{Complicationg factor:} CMS has now put providers in a difficult position.
"They are required to provide this therapy, but the Administration is providing very little help to cover its high costs," Silverstein said. "The Administration's final inpatient rule, announced last week, does not do enough to adequately reimburse institutions for the cost of care or the cost of the product."
{This article reminded me of Judy Perkins, the stage 4 breast cancer patient who remains cancer free 2 years after treatment with a new, experimental treatment. It is my understanding that that therapy used her T-calls but was a different technique. "CAR-T only works in blood cancers.... A different tactic is needed for solid tumors, such as breast cancer. And even though it is very expensive and very complicated, CAR-T can be successful, he noted. "It's a whole different way of thinking about cancer treatment," It is encouraging that CAR-T is now being covered by Medicare.}
{quote from https://www.nbcnews.com/health/health-news/highly-personalized-treatment-saves-breast-cancer-patient-n879841}
-
Air pollution is linked to poor survival after breast cancer diagnosis
The effect of atmospheric particulate matter on survival of breast cancer among US females
Results showed that patients living in counties with high levels of PM had an increased risk of early mortality. The risk of early mortality was increased by 33% for patients living in counties with increased pollution levels of large particles, and increased by 40% for patients living in counties with increased pollution levels of small particles. These results remained significant even after researchers accounted for social and economic differences between counties. Air pollution was related to increased risk of early mortality especially in early-stage cancer patients, and to a lesser degree in advanced-stage cancer patients.
https://link.springer.com/article/10.1007%2Fs10549-013-2527-9
DOI https://doi.org/10.1007/s10549-013-2527-9
{Egad! The pollution is going to kill us, too! With effects that large, makes you wonder if it is cause the problem to begin with.}
-
This isn't new, but it's an interesting video on how macrophages, supposedly some of our immunity good guys, can actually help the bad guy cancer cells to spread.
-
Thanks Lumpie and Santabarbarian, I'll look for resveratrol capsules from a good source. I'll report back if they help.
-
Calcium channel blocker and risk of lymphedema among breast cancer patients: nested case control study
Amanda J Stolarz, Mrinmayee Lakkad, V Suzanne Klimberg and Jacob T Painter
https://cebp.aacrjournals.org/content/early/2019/08/09/1055-9965.EPI-19-0448
-
Lumpie - thank you. Now I know what to call it. Contralateral Lymphedema. Google now finds what I am looking for instead of reminders to do BP and other constricting things on the opposite side. The left side healed a lot better than right, where there is a pronounced scar. I guess I should not have shoveled snow that winter. I asked the lymphatic therapist whether that might contribute, and she did not think so, that she had seen much heavier scarring. I think the surgeon was a good one, and did not compromise the non-cancer side. The oncologist ordered a CT scan, expect results in another week or so. Both the oncologist and therapist think it is very unusual, but for now, the treatment seems to be the same. Lymphatic sleeve and glove, and self-massage at home. The therapist also uses a sleeve which pumps the arm gently. Has anyone figured out an easy way to do the measurements? Even when I tape the tape measure to the arm , it is clumsy, and not very reliable. Looking at my arms I see everything from improvement, to getting worse, to no change. Perception can be deceiving. At first it went down, very slightly, then went back up. But it is definitely not as tight as it used to be.
2009 ER+ left breast. 52 yrs. Lumpectomy, Sentinel node removal, negative. Radiation 6 weeks, tamoxifen 5 years. Dense lumpy left breast, normal right. Acupuncture offered at facility as part of integrative medicine. It really helped with anxiety/stress during radiation treatment.
2016 ER+ left breast. Probably a new cancer, but unknown. 4 rounds TC Aug-Oct 2016, Bi-lateral (my choice) Nov 2016, no reconstruction. 2 sentinel nodes remove, negative. Cold Capping using Chemo Cold Caps (DIGNICAP not available). Anastrozole 1 mg starting May 2017. Joint issues noticed immediately. Stopped Anastrozole after 3-4 months due to joint stiffness in. After several months of no AIs, fingers were feeling better. Started tamoxifen March 2018
10/2018 noticed stiffness and some trigger finger again. Was eating meat a lot more (daily) than normal. Usually 1-2 /wk. Have cut way back on the meat, seems to help, but one finger still very prone to trigger finger. Trigger finger seemed to be getting better, but now 4/2019 seems worse, is it the break from added turmeric to meals?
7/19/2019 - swelling in R-arm, opposite side from where lymph nodes removed (contralateral lymphedema). Noticed 6/18/2019. Could have been swelling earlier but wearing long sleeves. Trip to urgent care. They did ultrasound, concerned that there might be a clot, there was not. Started seeing lymphatic therapist 7/2/2019.
-
Blue Girl: If no one has yet shared this site, it is a wealth of information about LE. Several of our BCO members helped get it going.
-
I tried the Untire App as part of a university research study. Unfortunately, I very quickly got bored and found it was too generic i.e. not personalised enough for me. Just my opinion of course, others may want to have ago and pitch in with their thoughts
-
Ladies: I follow this thread with great interest. Thank you for all the work and research done to bring this information to light.
I have a question regarding BC research and collection of outcome data in general. I was wondering if all of our data is swept into large databases anonymously so that these large studies can be done. So, when results for risk models and prediction calculators are published, they include the thousands of data points that we all represent (and that our doctors rely upon). It just seems logical that all these patient outcomes would be collected and analyzed somewhere.
Did I sign something when I was diagnosed that allows my doctors to contribute my data to the collective data monster? How we each fare on our various treatment plans and whether we have recurrences on those plans, is someone collecting that data (hopefully, anonymously)? I actually hope my data IS used along with thousands of others, because it would seem to make treatment and diagnosis decisions better each year for every new patient. But I've never asked my docs about this.
I would be very interested to know. -
Diveslikeagirl: I am not an expert on cancer databases but I know a little. Cancer statistics are collected in the SEER database. It is part of NIH and NCI. I believe that providers are not required to collect an authorization to report health information because reporting is government mandated. Frankly, I don't know the details of anonymity but researcher-users are required to sign a pledge not to reveal or seek to personally identify individuals in the database. You can read more about SEER here:
Additionally, many cancer centers/large medical centers maintain their own database for research purposes. If you are treated at such a center, you might ask about their data collection practices and how they facilitate research. People who specialize in maintaining these databases are "cancer registrars."
People have numerous opinions on and criticisms of the maintenance of these databases. For example, I know that, historically, SEER has only tracked one's first breast cancer diagnosis. They have not tracked later development of metastasis so the data on metastatic cancer is woefully lacking. There has been a great deal of advocacy around this issue - including a push to require collection of information related to any stage 4 diagnosis which follows an early stage breast cancer diagnosis.
Many of us agree that we would very much like for our experiences, including diagnosis and treatment, to be documented if that information may improve outcomes of others who develop cancer in the future.
-
Results From the First Multicenter, Open-label, Phase IIIb Study Investigating the Combination of Pertuzumab With Subcutaneous Trastuzumab and a Taxane in Patients With HER2-positive Metastatic Breast Cancer (SAPPHIRE)
The primary objective of this study was to assess the safety and tolerability of combination pertuzumab, subcutaneous trastuzumab (Herceptin), and investigator's choice of taxane chemotherapy in previously untreated patients with human epidermal growth factor receptor 2-positive metastatic breast cancer. Efficacy was a secondary objective.
This study was an open-label, non-randomized study of patients with human epidermal growth factor receptor 2-positive metastatic breast cancer who had no previous systemic non-hormonal anti-cancer therapy for metastatic disease. The primary endpoints included adverse events (AE), serious AEs, and cardiac AEs. Secondary endpoints included overall response rate, progression-free survival, and overall survival. Patients were treated with pertuzumab and subcutaneous trastuzumab in 3-weekly cycles with taxane chemotherapy until disease progression, unacceptable toxicity, or withdrawal of consent and followed for a minimum of 24 months from initiation of study treatment.
Subcutaneous trastuzumab in this combination has an acceptable safety and tolerability profile, including cardiac safety profile. Safety and efficacy appear similar to previous studies of intravenous trastuzumab in this combination.
https://www.clinical-breast-cancer.com/article/S1526-8209(18)30696-7/fulltext
-
Pay-to-Play Clinical Trials
Federal regulators are paying more attention to "pay-to-play" clinical trials that offer admission for a price, STAT reports.
The FDA confirmed to STAT that it asked an advisory committee to consider how the research community should think about these kinds of trials, and the panel is now drafting recommendations, according to the story. The National Institutes of Health has asked the committee to assess whether its existing guidance to patients considering a clinical trial would apply in this situation.
Both groups' actions follow the HHS Secretary's Advisory Committee on Human Research Protections' (SACHRP) consideration of pay-to-participate trial guidance. SACHRP is expected to release guidelines at its next meeting in December, or the following one in March. It took an interest in the subject last year following a plan in Florida to charge seniors a fee -- as high as $285,000 -- to enroll in a trial of "young blood" infusions for preventing aging.
There are no data on whether or not these types of trials are increasing, but more examples have cropped up recently, including another trial of "young blood" that charged about 80 people $8,000 each for infusions, and a clinic in Panama enrolled 20 autistic children in a stem cell trial that charged parents $7,200, STAT reports.
While FDA regulations permit a clinical trial "entry fee" in certain situations, the concern is that this could serve as a rouse for an entity looking to profit from desperate patients.
-
Tracking Candida auris
Candida auris is an emerging fungus that presents a serious global health threat. C. auris causes severe illness in hospitalized patients in several countries, including the United States. Patients can remain colonized with C. auris for a long time and C. auris can persist on surfaces in healthcare environments. This can result in spread of C. auris between patients in healthcare facilities.
Most C. auris cases in the United States have been detected in the New York City area, New Jersey, and the Chicago area. Strains of C. auris in the United States have been linked to other parts of the world. U.S. C. auris cases are a result of inadvertent introduction into the United States from a patient who recently received healthcare in a country where C. auris has been reported or a result of local spread after such an introduction.
Candida auris was made nationally notifiable at the 2018 Council for State and Territorial Epidemiologists (CSTE) Annual Conference. For the updated case definition and information on the nationally notifiable condition status, please see the 2018 CSTE position statement.
CDC encourages all U.S. laboratories that identify C. auris to notify their state or local public health authorities and CDC at candidaauris@cdc.gov. CDC is working closely with public health and healthcare partners to prevent and respond to C. auris infections. The CDC-sponsored Antibiotic Resistance Laboratory Network (ARLN) will help improve detection and response to C. auris nationwide.
{This is rather technical but strains of multi-drug resistant C. auris have been identified in the U.S. The public should be aware and those with compromised immune systems may wish to take note.}
https://www.cdc.gov/fungal/candida-auris/tracking-c-auris.html
https://www.cdc.gov/fungal/candida-auris/index.html
https://www.cdc.gov/drugresistance/solutions-initiative/stories/cdc-response-to-global-threat.html
-
Advanced HER2-Positive Breast Cancer: All Eyes on These Novel Agents
NEW AGENTS for the treatment of advanced HER2-positive breast cancer should be coming soon to your clinic... Clinicians can expect new agents soon. "The landscape may change in a year or 2," Dr. Hurvitz predicted at the 2019 Miami Breast Cancer Conference.1 "There are some very promising agents that may become available for later lines and may actually challenge the treatment paradigm we currently follow."
{This is from April but I don't beleive that the link has been posted.}
-
AZ announces Phase I DS-8201 results
AstraZeneca has announced two Lancet Oncologypublications of its Phase I dose-expansion results of DS-8201 (trastuzumab deruxtecan) in HER2-positive metastatic breast and gastric cancer.
The breast cancer trial found a confirmed objective response rate of 59.5% and a disease control rate of 93.7% at a recommended expansion dose of 5.4 or 6.4 mg/kg. There was also a 20.7 months median duration of response in HER2-positive metastatic breast cancer patients previously treated with trastuzumab emtansine... Patients enrolled in this part of the trial had a median of seven prior lines of treatment, including trastuzumab and trastuzumab emtansine, and in 86% of cases, pertuzumab.
"For patients with HER2-positive metastatic breast cancer that progresses after trastuzumab, pertuzumab, and trastuzumab emtansine, optimal treatment is not clearly defined and choices may be limited. These results demonstrate preliminary clinically-meaningful response rates with an impressive duration of response, supporting further development and suggesting a potential role for trastuzumab deruxtecan as a HER2-targeted therapy option in this setting,"
-
About cancer databases: A month or two ago, I received an invitation by mail to participate in a survey of breast cancer patients from a certain demographic. The letter was from a local NCI cancer center in partnership with my state's health dept. The letter explained that my name was obtained from the state cancer database. I was a bit surprised, because I was also unaware that my personal information was being stored in a state database. I have no idea if paperwork I have signed revealed this. I would have signed anything to make the treatment begin when I was first diagnosed. And, they have those electronic signature deals at my cancer center, where you don't really get to read everything before they give you the pad & pen to sign.
I have since found out that my state also participates in SEER. I wonder how much information is disclosed to them. Yes, I do want to be counted and have my data used in research but how much personal identifying information about me is being stored and distributed?
On another note - this thread is so fantastic! Big thank you to Lumpie and others who regularly contribute. What an amazing gold mine of information you ladies have created!
-
Long-Term Comparison of Aesthetical Outcomes After Oncoplastic Surgery and Lumpectomy in Breast Cancer Patients
Lumpectomy may result in major deformities and asymmetries in approximately one-third of patients. Although oncoplastic surgery (OP) could be a useful alternative to avoid them, lack of strong data is causing some debate. The purpose of this study was to compare aesthetic outcomes in patients undergoing OP versus lumpectomy using three different assessment methods.
Methods
A total of 122 patients were included in this cross-sectional multicentric study; 57 underwent OP (46.7 %), and 65 underwent lumpectomy (53.3 %). Two breast surgeons and two plastic surgeons from different institutions using the Garbay scale independently evaluated aesthetic outcomes. BCCT.core software was applied in both groups, and the patients evaluated their aesthetic outcomes answering a questionnaire about their satisfaction rate.
Results
OP group had a higher proportion of excellent aesthetic results according to the BCCT.core software analysis (p = 0.028) and the specialists (p = 0.002). Multifactorial analyses showed that age ≥70 years (RP = 6.02; 95 % confidence interval [CI] 1.73–21.0; p = 0.005), tumors in the medial, inferior, and central quadrants (RP = 4.21; 95 % CI 1.88–9.44; p < 0.001), and large breasts (RP = 7.55; 95 % CI 2.48–23.0; p < 0.001) were significant risk factors for poor aesthetic outcomes after lumpectomy. The patients classified their results as better than those by the specialists and by the software, with no statistical difference between the groups.
Conclusions
Excellent aesthetic results were more frequent in the OP group according to BCCT.core software analysis and specialists. In addition, some clinical conditions and tumor locations in the breast can be considered risky factors for poor aesthetic outcomes in lumpectomy.
https://link.springer.com/article/10.1245%2Fs10434-014-4301-6#citeas
-
Flavonoids in Plants May Help Protect Against Major Killers
August 19, 2019 4:58 pmConsuming flavonoids, a large class of nutrients found in plant foods, may reduce the risk for cancer and cardiovascular death.
Researchers used data on 56,048 Danes, following their diet and health prospectively for 23 years. During that time, 14,083 of them died. The study is in Nature Communications.
After controlling for smoking, hypertension, cholesterol and many other health and dietary factors, they found that compared with people in the lowest one-fifth for flavonoid intake, those in the highest one-fifth had a 17 percent reduced risk for all-cause mortality, a 15 percent reduced risk for cardiovascular disease death, and a 20 percent reduced risk for cancer mortality. The association peaked at about 500 milligrams of flavonoids a day, and was stronger for smokers, heavy drinkers and the obese.
Good sources of flavonoids include tea, chocolate, red wine, citrus fruits, berries, apples and broccoli. One cup of tea, one apple, one orange, and three-and-a-half ounces each of blueberries and broccoli would supply more than 500 milligrams of total flavonoids.
"Participants with a higher flavonoid intake also tended to have a healthier diet over all," said the lead author, Nicola P. Bondonno, a postdoctoral fellow at Edith Cowan University in Perth, Australia. "But flavonoids were still associated with a lower risk of death after adjusting for other dietary components, as well as within the group of participants with the highest fruit and vegetable intakes."
Source: NYT
-
Daiichi Sankyo Confirms Plans to Accelerate BLA Submission to U.S. FDA for [Fam-] Trastuzumab Deruxtecan (DS-8201) in HER2 Positive
(March 28, 2019) – Daiichi Sankyo Company, Limited (hereafter, Daiichi Sankyo) today announced plans to accelerate filing of the Biologics License Application (BLA) with the U.S. Food and Drug Administration (FDA) for [fam-] trastuzumab deruxtecan (DS-8201), an investigational HER2 targeting antibody drug conjugate (ADC), in patients with HER2 positive metastatic breast cancer previously treated with ado trastuzumab emtansine
(T-DM1). Submission of the application, which was originally planned for 2020, is now scheduled for the first half of fiscal year 2019.
{Not super new but interesting. I gather that this application may have been delayed to fall 2019.}
https://www.daiichisankyo.com/media_investors/media_relations/press_releases/detail/006986.html
-
-
About next-gen cell-based cancer therapies, and the clinical and economic challenges they pose. "But the patient who enters the operating room for a mastectomy, or is infused with CAR-T cells, emerges permanently changed, anatomically, physiologically, or genetically. And she is, in a way, a collaborator in the treatment as well as its subject."
https://www.newyorker.com/magazine/2019/07/22/the-promise-and-price-of-cellular-therapies
-
Researchers convert pro-tumor macrophages into cancer killers
(Research on pancreatic and lung cancer but most bc is epithelial)
Epithelial cancers, such as cancers of the lung and pancreas, use the ανβ3 molecule to gain drug resistance to standard cancer therapies and to become highly metastatic. In a paper published in Cancer Research, University of California San Diego School of Medicine researchers identified a new therapeutic approach in mouse models that halts drug resistance and progression by using a monoclonal antibody that induces the immune system [tumor-associated macrophages (TAMs)] to seek and kill ανβ3-expressing cancer cells...
During the study period, no tumor progression or drug resistance was detected while untreated animals developed tumor growth and metastasis...
The antibody prompts these macrophages to begin killing tumor cells through a mechanism known as antibody-dependent cytotoxicity (ADCC).
"These results were initially unexpected since macrophages usually destroy cells via phagocytosis... The therapeutic antibody we are utilizing is bridging the macrophage to the ανβ3-expressing tumor cell as a target. When this occurs it releases a cytotoxic substance that kills the tumor cell."
The team is currently producing a humanized version of this antibody, which Cheresh hopes will do in humans what LM609 does in mice.
Article https://www.sciencedaily.com/releases/2019/08/190821125527.htm
Study at https://cancerres.aacrjournals.org/content/early/2019/08/15/0008-5472.CAN-19-1246
-
Researchers Find Full Chemotherapy Dose Is Best for Common Type of Breast Cancer
Researchers looked at the impact of reducing chemo doses after breast surgery (called adjuvant therapy) using a combination of four different drugs: 5-fluorouracil, epirubicin, cyclophosphamide, and docetaxel (FEC-D). The drugs were given in four to six treatments cycles.
The study found that both the overall and 5-year disease-free survival rate was worse in those who received less than 85 percent of the recommended chemotherapy dose over six treatment cycles.
"What surprised us the most was how dramatically early reductions in chemotherapy affect survival compared to later modifications," said Dr. Zachary Veitch, from the department of oncology in the University of Calgary Tom Baker Cancer Centre, in a statement...
Although, when researchers split the lower-dose group in two based on dose reduction during the first three cycles versus the last three, they found the outcomes weren't worse when doses were reduced during the later cycles.
"The majority of cancer cells that are sensitive to chemotherapy may be killed in the first few treatments, rather than in the later treatments. Thus, reducing the dose late may not have as much of an impact," Veitch speculated in the statement.
Article: https://www.healthline.com/health-news/high-doses-of-chemotherapy-best-for-certain-breast-cancers
More detailed article: https://www.newswise.com/articles/maintaining-full-doses-of-chemotherapy-can-be-key-for-breast-cancer-survival-according-to-new-research-in-jnccn/sc-mwhr
Study: https://jnccn.org/view/journals/jnccn/17/8/article-p957.xml
-
Timelines Matter in the Treatment of Breast Cancer
Patients who received chemotherapy more than 120 days after being diagnosed with breast cancer had significantly worse overall survival compared with those who received chemotherapy within 120 days, reported a large retrospective analysis in the Annals of Surgical Oncology...
The analysis showed that regardless of surgery type, patients who started chemotherapy beyond 120 days from the time of diagnosis had worse overall survival compared with patients who started chemotherapy within 120 days (hazard ratio [HR]=1.29; 95% CI, 1.22–1.37; P<0.001).
The association of worse survival and chemotherapy treatment delays was consistent across tumor subtypes evaluated, with HER2-positive disease most affected (HR=1.47; 95% CI, 1.29–1.68), followed by triple-negative breast cancer (HR=1.23; 95% CI, 1.10–1.38) and hormone receptor-positive and HER2-negative disease (HR=1.23; 95% CI, 1.13–1.34).
"The take-home message is try to get your chemotherapy in as early as possible," Shapiro said.
Article: https://www.cancernetwork.com/news/timelines-matter-treatment-breast-cancer
Study: https://link.springer.com/article/10.1245%2Fs10434-019-07566-7
-
New St. Gallen International Breast Cancer Guidelines Recommend Oncotype DX Breast Recurrence Score® Test to Guide Chemotherapy for Node-negative and Node-positive Early-stage Breast Cancer
...In particular, the panelists recognized the value of the landmark TAILORx study results and noted that women with node-negative cancers and Recurrence Score® results ≤25 do not need chemotherapy.3 This group represents up to about 80% of patients who may be safely spared chemotherapy. The Breast Recurrence Score test also identifies those patients (with results of 26 to 100) who may receive a life-saving benefit from chemotherapy...
The new St. Gallen International Consensus guidelines, "Estimating the benefits of therapy for early stage breast cancer," were recently published online in the Advance Access section of Annals of Oncology and will appear in a future print issue...
Over the last several months, results of the TAILORx study have influenced positive treatment guideline updates distinguishing the Oncotype DX Breast Recurrence Score test from prognostic-only tests based on clinical evidence and the critical importance of predicting chemotherapy benefit. This includes the recent update to ASCO guidelines, which increased the proportion of women who can be effectively treated without chemotherapy based on the Recurrence Score results, highlighting the importance of testing all medically eligible early-stage breast cancer patients with the Breast Recurrence Score test. The National Comprehensive Cancer Network (NCCN) updated its guidelines in 2018 to categorize the Breast Recurrence Score test as the only "preferred" test for chemotherapy treatment decision-making for patients with node-negative, early-stage breast cancer. NCCN also classified the Breast Recurrence Score test as the only test that is predictive of chemotherapy benefit.
Article: https://finance.yahoo.com/news/st-gallen-international-breast-cancer-120000449.html
-
Are there any benefits to continuing trastuzumab after disease progression in patients with HER2+ metastatic breast cancer?
A Pooled Analysis of 2618 Patients Treated With Trastuzumab Beyond Progression for Advanced Breast Cancer
In HER2+ MBC, continuing trastuzumab (T) after the progression during a first-line T-based regimen, represents 1 of the possible strategies, even if few data from randomized trials exist in this setting.A total of 29 studies (4 randomized controlled phase III trials, 2 observational studies, 8 prospective nonrandomized trials, and 15 retrospective case series) were retrieved for a total of 2618 patients. All were treated with a second-line, T-based treatment beyond progression with a first-line T-based chemotherapy. Overall, the median RR, TTP, and OS obtained from the selected articles were 28.7%, 7, and 24 months.Conclusions: This pooled analysis confirms that continuing T beyond the first progression continues to be 1 of the effective and preferred choices in HER2+ MBC, failing a (T-based) first-line regimen.Clinical Breast Cancer Volume 13, Issue 2, April 2013, Pages 81-87{NOTE: This is OLD research but it is interesting and I had never read it before....and it came out in a news blast for some reason. An oncologist was mentioning to me recently that, especially if there is a solitary lesion that progresses, it is possible that only that lesion has morphed into a different type of cancer and that the Herceptin (&/or Perjeta) is still controlling the HER2+ cancer.} -
How diabetes can increase cancer risk
"It's been known for a long time that people with diabetes have as much as a 2.5-fold increased risk for certain cancers," says John Termini, Ph.D., who is presenting the work at the [American Chemical Society (ACS) Fall 2019 National Meeting & Exposition]. These cancers include ovarian, breast, kidney and others...
He wondered if the elevated blood glucose levels seen in diabetes could harm DNA, making the genome unstable, which could lead to cancer. So Termini and colleagues looked for a specific type of damage in the form of chemically modified DNA bases, known as adducts, in tissue culture and rodent models of diabetes. Indeed, they found a DNA adduct, called N2-(1-carboxyethyl)-2'-deoxyguanosine, or CEdG, that occurred more frequently in the diabetic models than in normal cells or mice. What's more, high glucose levels interfered with the cells' process for fixing it. "Exposure to high glucose levels leads to both DNA adducts and the suppression of their repair, which in combination could cause genome instability and cancer," Termini says...
They wanted to determine the molecular reasons why the adducts weren't being fixed properly by the cells. They identified two proteins that appear to be involved: the transcription factor HIF1α and the signaling protein mTORC1, which both show less activity in diabetes...
According to Termini, several drugs that stimulate HIF1α or mTORC1 already exist. The researchers plan to see if these drugs decrease cancer risk in diabetic animal models, and if so, they will test them in humans. Termini notes that metformin, a common diabetes medication that helps lower blood glucose levels, also stimulates DNA repair. "We're looking at testing metformin in combination with drugs that specifically stabilize HIF1α or enhance mTORC1 signaling in diabetic animal models," he says.
Article: https://medicalxpress.com/news/2019-08-diabetes-cancer.html
-
Oh no!
Menopause. 2016 May;23(5):584-6. doi: 10.1097/GME.0000000000000593.
Yoga increased serum estrogen levels in postmenopausal women-a case report.
Abstract
OBJECTIVE:
This case report aimed to evaluate 4 months of yoga practice on the quality of life (QOL) and estradiol levels of two postmenopausal women.
METHODS:
Participants were clinically healthy postmenopausal women, with follicle-stimulating hormone levels greater than or equal to 30 mIU/mL and a body mass index lower than 30 kg/m. The participants practiced yoga for 4 months in two 1-hour sessions per week.
RESULTS:
The participants exhibited an abnormal estrogen-level increase after 4 months of yoga practice and showed QOL improvements.
CONCLUSIONS:
In some cases, yoga practice can affect the female neuroendocrine system, increasing estrogen and improving QOL.
- PMID:
- 26926324
- DOI:
- 10.1097/GME.0000000000000593
- [Indexed for MEDLINE]
-
debbew, that's very interesting. I've been wondering if there is something magical about metformin in reducing risk, or if the magic is in controlled glucose levels. "Exposure to high glucose levels leads to both DNA adducts and the suppression of their repair, which in combination could cause genome instability and cancer," Termini says... So it sounds like the magic of metformin is in the control, and not necessarily otherwise. If you can control your glucose with diet and exercise, that might be enough to reduce risk.
Feel free to correct me if I didn't interpret this correctly.
-
MountainMia, I'm no expert at any of this, but I'm also interested in the benefits of controlling glucose levels and/or the benefits of metformin. The article exposed a new mechanism of action by which controlling glucose by any means (e.g. diet and exercise) should reduce cancer risk (less DNA damage, better repair). This may be in addition to other potential mechanisms (e.g. less insulin stimulating growth).
I think the researcher mentions metformin as one possible intervention to study for controlling glucose but mentions in passing that metformin "also stimulates DNA repair." I don't think that undermines the possible benefit of controlling glucose through other means. But metformin may also have some additional "magic." Several potential anti-aging effects of metformin are currently being studied in the TAME trial: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5943638/
-
Identifying Women at High Risk of Advanced Breast Cancer for Discussion of Supplemental Imaging
- JAMA internal medicine In this study, the authors prospectively assessed 638,856 women between 40 and 74 years of age undergoing routine screening to identify those at high risk of advanced breast cancer. The rates of advanced cancer were higher among women with heterogeneously dense breasts and with a 5-year BCSC breast cancer risk of ≥2.5%. The rate of advanced cancer was also higher among women with extremely dense breasts and a 5-year BCSC breast cancer risk of ≥1%.The authors suggest that breast density notification should go out with the notification of breast cancer risk to women at highest risk fo advanced disease, winnowing out women who do not need supplemental imaging, and serving as an effective platform upon which to base a discussion regarding supplemental imaging among women who do.https://www.practiceupdate.com/C/86192/56?elsca1=emc_enews_topic-alerthttps://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2737320doi:10.1001/jamainternmed.2019.1758
-
Docs Brace for Medicare 'Appropriate' Imaging Rule
With deadline just 4 months away, fears of unreadiness and unintended consequences abound
As the medical community braces for implementation of the Protecting Access to Medicare Act (PAMA) by the Jan. 1, 2020 deadline, some wonder if it's even feasible or if another program delay is on the horizon.
The policy, aimed at reducing unnecessary testing, mandates that all advanced diagnostic imaging orders go through an algorithm that provides key confirmation codes required when Medicare is billed later on for the service.
Dubbed a "clinical decision support mechanism" (CDSM), this software processes each CT, MRI, nuclear medicine, and PET order before spitting out its verdict to the ordering professional: "appropriate," "maybe appropriate," or "rarely appropriate," according to a certain set of appropriate use criteria (AUC).
...the CDSM confirmation code provides proof that the ordering physician consulted AUC. Eventually, Medicare will not pay claims or advanced imaging without these codes.
-
Mountain Mia if you look at Jane McClelland's book "How to starve cancer" Metformin interferes with multiple pathways by which cancer cells manage to eat. Not just glucose, but also glutamine and Fatty Acid pathways. It has more than one beneficial effect.
-
"Diagnosis," new Netflix series
{I received this message about a new Netflix series. Since some of us have encountered "complexities" with getting an accurate diagnosis, I thought that this might be of interest.}
Doctors always hope for an easy diagnosis. It means we can provide the right treatment and a hopeful path to recovery. But human bodies are complicated. Debilitating fatigue on top of a full-body rash? Sometimes symptoms don't point to a clear diagnosis.
That's when we approach medicine like detectives. We have to understand a patient's story, uncover clues and solve the mystery of the illness. Then, we can get the patient's life back on track.
In my 17 years writing for The New York Times Magazine, I've described some fascinating cases. I'm thrilled to bring more cases to life in a new Netflix series "Diagnosis." In each episode, we meet a patient and harness the power of readers like you to help arrive at a diagnosis.
My hope is that the series will give viewers a sense of the obstacles we face in medicine, and how we overcome them — because no patient should ever struggle alone.
Thanks for reading (and watching).
Lisa Sanders, M.D., contributing writer for The New York Times Magazine and associate professor at the Yale University School of Medicine.
Link to trailer here:
https://www.nytimes.com/2019/07/22/magazine/diagnosis-tv-netflix-lisa-sanders.html?smid=rd
-
Lumpie: Thanks for the imaging parameters article. I'm going to push even harder for an MRI before year end based on my specific circumstances.
-
Photobiomodulation therapy for the management of radiation-induced dermatitis : A single-institution experience of adjuvant radiotherapy in breast cancer patients after breast conserving surgery.
https://reference.medscape.com/medline/abstract/28243723
-
Bioengineering (Basel). 2018 Jun 9;5(2). pii: E44. doi: 10.3390/bioengineering5020044.
Photobiomodulation Therapy (PBMT) in Peripheral Nerve Regeneration: A Systematic Review.
Abstract
Photobiomodulation therapy (PBMT) has been investigated because of its intimate relationship with tissue recovery processes, such as on peripheral nerve damage. Based on the wide range of benefits that the PBMT has shown and its clinical relevance, the aim of this research was to carry out a systematic review of the last 10 years, ascertaining the influence of the PBMT in the regeneration of injured peripheral nerves. The search was performed in the PubMed/MEDLINE database with the combination of the keywords: low-level laser therapyAND nerve regeneration. Initially, 54 articles were obtained, 26 articles of which were chosen for the study according to the inclusion criteria. In the qualitative aspect, it was observed that PBMT was able to accelerate the process of nerve regeneration, presenting an increase in the number of myelinated fibers and a better lamellar organization of myelin sheath, besides improvement of electrophysiological function, immunoreactivity, high functionality rate, decrease of inflammation, pain, and the facilitation of neural regeneration, release of growth factors, increase of vascular network and collagen. It was concluded that PBMT has beneficial effects on the recovery of nerve lesions, especially when related to a faster regeneration and functional improvement, despite the variety of parameters.
KEYWORDS:
low-level laser therapy; nerve regeneration; peripheral nerve repair; photobiomodulation therapy; tissue regeneration
- PMID:
- 29890728
- PMCID:
- PMC6027218
- DOI:
- 10.3390/bioengineering5020044
-
Diverse immune cell profiles and roles found in breast cancer resistance to immunotherapy
With the goal of better understanding the role immune cells within tumors play in tumor growth and in response to therapy, Zhang and his colleagues conducted a series of analyses to characterize the immune cell composition of tumor microenvironments in eight murine models and in clinical datasets of triple negative breast cancers...
The researchers found large diversity in the frequency of neutrophils and macrophages among the tumor samples, including some tumors that preferentially attracted macrophages, while others attracted more neutrophils. The predominance of one cell type over the other can be explained in part by the type of molecules produced by the tumor. As Zhang explained, some tumors secrete molecules that attract macrophages, while other tumors produce other molecules that lure neutrophils to the tumor site...
Exploring the roles macrophages and neutrophils play in tumor growth revealed that in some tumors macrophages favored tumor growth, while in others they helped control it. Neutrophils, on the other hand, tended to promote tumor growth.
"These findings are just the beginning. They highlight the need to investigate these two cellular types deeper. Under the name 'macrophages' there are many different cellular subtypes and the same stands for neutrophils," Zhang said. "We need to identify at single cell level which subtypes favor and which ones disrupt tumor growth taking also into consideration tumor heterogeneity as both are relevant to therapy."
Article: https://medicalxpress.com/news/2019-08-diverse-immune-cell-profiles-roles.html
-
DEPRESSION, ANXIETY LINKED TO OPIOID USE IN OLDER WOMEN WITH BREAST CANCER
Elderly women battling breast cancer who have anxiety, depression or other mental health conditions are more likely to use opioids and more likely to die, a new study led by the University of Virginia School of Medicine has found.
https://news.virginia.edu/content/depression-anxiety-linked-opioid-use-older-women-breast-cancer?
Mental Health Comorbidities and Elevated Risk of Opioid Use in Elderly Breast Cancer Survivors Using Adjuvant Endocrine Treatments
Journal of Oncology Practice Published online July 19, 2019
CONCLUSION:
The presence of mental health comorbidity in breast cancer survivors significantly increases the risk of opioid use and mortality, which highlights the need for better management of comorbid mental health conditions.
https://ascopubs.org/doi/10.1200/JOP.18.00781
{Thanks to Ingerp for sharing this article.}
-
Fake news? I don’t trust the opioid and elderly women article just posted. Exactly howmany breast cancer patients overdose on opioids? And since when do doctors acknowledge that breast cancer CAUSES anxiety? Another way to take pain treatment away from those who seriously need it.
Last paragraphs say
The researchers noted potential limitations to their study such as a lack of information on the opioids used and a lack of details on the patients' pain assessments. They also suggest that mental health conditions such as depression may be underdiagnosed and that, as a result, the research may underestimate the percentage of patients with those conditions.
Tan disclosed potential conflicts of interest including owning stock in and receiving compensation from biopharmaceutical company Merck. Balkrishnan disclosed that he has done consulting or advising for Merck.
To keep up with the latest medical research news from UVA, subscribe to the Making of Medicine blog.
-
Novel therapy studied for inherited breast cancer
A tiny molecule called microRNA (miR) 223-3p prevents normal cells from making mistakes while repairing their DNA. However, cancers with BRCA1 mutations repress miR223-3p to permit their cells to divide. Adding back miR223-3p forces the BRCA1-mutant cancer cells to die, said study co-author Patrick Sung...
There is evidence that restoring miR223-3p before cells convert to cancer can even prevent BRCA1-related disease, he said.
Article: https://www.sciencedaily.com/releases/2019/08/190827153106.htm
-
FDA: Men Should Be Included in Breast Cancer Clinical Trials
"Less than 1 percent of all breast cancer cases occur in men, but men are more likely to be diagnosed at an older age and have a more advanced stage of disease. As breast cancer in men is rare, they have typically not been included in clinical trials for breast cancer treatment," according to an FDA news release. "This has led to a lack of data, so their treatment is generally based upon studies and data collected in women. While some FDA-approved treatments are gender-neutral in their indication, many therapies are only approved for women and further data may be necessary to support labeling indications for men."
The public comment period for the draft guidance ends Oct. 26 {2019}
https://www.practiceupdate.com/C/88648/56?elsca1=emc_enews_topic-alert
-
A PoEM on breast cancer metastasis [newly identified macrophage induces metastasis]
When breast cancer cells spread through the body, they do so mainly through the lymph system that normally removes excess fluid and waste products from our tissues. Now, scientists from the group of Professor Massimiliano Mazzone (VIB-KU Leuven Center for Cancer Biology) identified a novel subset of immune cells, called Podoplanin-expressing macrophages (PoEMs), that change the tissues near a tumor in a way that promotes the spreading of cancer cells. Getting rid of these PoEMs in a mouse model strongly reduced the ability of breast cancer cells to move to other parts of the body...
These findings provide supportive evidence to targeting PoEMs in humans. With the help of clinicians and pathologists from KU Leuven and UZ Antwerpen, the researchers further tested their findings in human cancer samples. Pawel Bieniasz-Krzywiec provides more details: "On top of the mice results, human breast cancer sample testing revealed a positive correlation between the presence of PoEMs around tumor lymph vessels and lymph node involvement as well as organ metastasis. These observations pave the road towards the use of PoEM blockers in cancer therapy, specifically targeting the cancer-associated lymphatic vessels, without triggering lymphedema associated with current strategies."
Article: https://medicalxpress.com/news/2019-08-poem-breast-cancer-metastasis.html
Study: https://www.sciencedirect.com/science/article/abs/pii/S1550413119304280?via%3Dihub
-
Turbocharging the body's natural killer cells to defeat cancer
The scientists found that a protein -- called Activin-A -- which is found naturally in both healthy human cells and cancer cells, directly disables the NK cell's capacity to halt cancer growth.
Importantly, they were able to block Activin-A in preclinical models, using human and mouse NK cell models, with the hormone Follistatin.
According to Professor Huntington, "these findings may open the door to novel immune-therapy drugs which provide a deeper and more durable way to overcome the immune suppression seen in cancer, improving patient outcomes."
Mentioned in the study:
In breast and ovarian cancer cells, activin-A signaling induces the epithelial-mesenchymal transition (EMT), a malignant cellular reprogramming that is characteristic of TGF-β signaling (28, 29). In addition, activin-related genes are increased in expression during breast cancer cell EMT (30).
Article: https://www.sciencedaily.com/releases/2019/08/190827145734.htm
-
Lumpie, The FDA encouraging men to be included in trials and studies is a huge thing.
Here's another link to an article that quotes my view:
https://www.forbes.com/sites/victoriaforster/2019/...
-
High Marks for Proton-Beam RT in Breast Cancer
-
High Marks for Proton-Beam RT in Breast Cancer
No grade 3 radiation toxicity, good disease control and survival at 5 years
Women with locally advanced breast cancer requiring regional lymph node irradiation had similar disease control with less toxicity with proton-beam radiation therapy (RT) as compared with historical patients treated with conventional radiotherapy, investigators in a small prospective study reported.
PURPOSE
To evaluate the safety and efficacy of proton beam radiation therapy (RT) for patients with breast cancer who require regional nodal irradiation.
CONCLUSION
Proton beam RT for breast cancer has low toxicity rates and similar rates of disease control compared with historical data of conventional RT. No early cardiac changes were observed, which paves the way for randomized studies to compare proton beam RT with standard RT.
https://ascopubs.org/doi/abs/10.1200/JCO.18.02366?journalCode=jco
DOI: 10.1200/JCO.18.02366 Journal of Clinical Oncology
Published online August 26, 2019.
{Mysticalcity: how funny. We seem to have been reading the same article at the same time!}
-
Pyrotinib or Lapatinib Combined With Capecitabine in HER2–Positive Metastatic Breast Cancer With Prior Taxanes, Anthracyclines, and/or Trastuzumab: A Randomized, Phase II Study
PURPOSE
Pyrotinib, an irreversible pan-ErbB inhibitor, showed promising antitumor activity and acceptable tolerability in a phase I trial. We assessed the efficacy and tolerability of pyrotinib versus lapatinib, both in combination with capecitabine, in women with human epidermal growth factor receptor 2 (HER2)-positive metastatic breast cancer in an open-label, multicenter, randomized phase II study.
CONCLUSION
In women with HER2-positive metastatic breast cancer previously treated with taxanes, anthracyclines, and/or trastuzumab, pyrotinib plus capecitabine yielded statistically significant better overall response rate and progression-free survival than lapatinib plus capecitabine in this randomized phase II trial.
https://ascopubs.org/doi/abs/10.1200/JCO.19.00108
DOI: 10.1200/JCO.19.00108 Journal of Clinical Oncology
Published online August 20, 2019.
-
Regarding proton beam therapy, I was just reading an article a few days ago about carbon ion therapy, which was initiated in the U.S. but is now available only in Asia and Europe.
"Carbon ion therapy is similarly precise [to proton therapy], but because carbon ions are heavier, they deliver more cancer-killing power than protons do. Carbon centers have reported impressive survival rates, particularly for hard-to-treat bone and soft-tissue cancers such as spinal tumors."
https://www.wired.com/story/why-a-promising-potent-cancer-therapy-isnt-used-in-the-us/
-
Hormone Therapy and Breast Cancer: Yes, There Is Risk
But how big, and how important for individual women, is thornier question
Menopausal hormone therapy (MHT) was tied to increased breast cancer risk in a global study -- but implications for individual patients are less clear.
...those who reported ever using MHT had a 26% higher relative risk for developing breast cancer compared with never-users (RR 1.26, 95% CI 1.24-1.28), reported the Collaborative Group on Hormonal Factors in Breast Cancer.
the findings are definitely concerning, ... "Clinicians must heed the message of this study but also take a rational and comprehensive approach to the management of menopausal symptoms, with careful consideration of the risks and benefits of initiating MHT for each woman."
"This might be dependent on severity of the symptoms, contraindications for MHT (i.e., breast cancer, cardiovascular disease, and stroke), and BMI, and could take into account patient preference," she continued. "For likely candidates, MHT (preferably estrogen alone) should be initiated around the time of natural menopause and ideally limited to 5 years of use."
Primary Source
The Lancet
Source Reference: Collaborative Group on Hormonal Factors in Breast Cancer "Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence" Lancet 2019; DOI: 10.1016/S0140-6736(19)31709-X.Secondary Source
The Lancet
Source Reference: Kotsopoulos J "Menopausal hormones: definitive evidence for breast cancer" Lancet 2019; DOI: 10.1016/S0140-6736(19)31901-4.
-
Positive Breast Cancer Data for PD-1/L1 Inhibitors
Higher pCR rate in neoadjuvant setting follows success in metastatic triple-negative disease
Adding a PD-L1 inhibitor to neoadjuvant chemotherapy increased the rate of pathologic complete response (pCR) in triple-negative breast cancer (TNBC), particularly when the immunotherapy was started first, a placebo-controlled trial showed.
Patients who received durvalumab (Imfinzi) in addition to chemotherapy had a pCR rate of 53.4% versus 44.2% with placebo and chemotherapy. The difference did not attain statistical significance, except in a subgroup of patients who started the PD-L1 inhibitor 2 weeks before chemotherapy. In that subgroup, the odds of achieving pCR more than doubled with durvalumab.
The results added to evidence from a previous study that showed significant improvement in pCR with the addition of pembrolizumab (Keytruda) to chemotherapy for patients with newly diagnosed TNBC.
"We now have an approved indication in breast cancer, and I think that represents real progress,"
Primary Source
Annals of Oncology
-
New clues to the cause of permanent hair loss caused by chemotherapy.
Priming mobilization of hair follicle stem cells triggers permanent loss of regeneration after alkylating chemotherapy
The maintenance of genetic integrity is critical for stem cells to ensure homeostasis and regeneration. Little is known about how adult stem cells respond to irreversible DNA damage, resulting in loss of regeneration in humans. Here, we establish a permanent regeneration loss model using cycling human hair follicles treated with alkylating agents: busulfan followed by cyclophosphamide. We uncover the underlying mechanisms by which hair follicle stem cells (HFSCs) lose their pool. In contrast to immediate destructive changes in rapidly proliferating hair matrix cells, quiescent HFSCs show unexpected massive proliferation after busulfan and then undergo large-scale apoptosis following cyclophosphamide. HFSC proliferation is activated through PI3K/Akt pathway, and depletion is driven by p53/p38-induced cell death. RNA-seq analysis shows that HFSCs experience mitotic catastrophe with G2/M checkpoint activation. Our findings indicate that priming mobilization causes stem cells to lose their resistance to DNA damage, resulting in permanent loss of regeneration after alkylating chemotherapy.
https://www.nature.com/articles/s41467-019-11665-0
- Published: 27 August 2019
- Nature Communicationsvolume 10, Article number: 3694 (2019)
{This article is extremely technical but the matter will undoubtedly be of interest to some.} -
Trastuzumab Biosimilar vs Reference Trastuzumab in the Neoadjuvant Setting for HER2-Positive Breast Cancer
- The authors of this report provide 3-year follow-up data from a phase III study of a trastuzumab biosimilar versus reference trastuzumab in the neoadjuvant management of HER2+ breast cancer. Cardiotoxicity was rare, with similar rates between groups. The 3-year event-free survival was better in the biosimilar group compared with the reference trastuzumab group (91.9% vs 85.2%).
- The rate of event-free survival at 3 years was better with a trastuzumab biosimilar than with reference trastuzumab, and cardiotoxicity was rare in both cohorts.
{It has been noted that this study investigated only one of 5 available biosimilars; nonetheless, it may be reassuring to some that biosimilars are not simply inferior.} -
Safety and Efficacy of T-DM1 Plus Neratinib in Patients With Metastatic HER2-Positive Breast Cancer
- The authors of this 3 + 3 dose-escalation study enrolled 27 patients with metastatic HER2-positive metastatic breast cancer who had progressed on dual-antibody therapy (trastuzumab, pertuzumab) and a taxane. They were treated across four dose levels of neratinib in combination with ado-trastuzumab emtansine (T-DM1). An objective response was evident in 63% of evaluable patients. The responses were deeper and more durable in patients with cell-free DNA ERBB2 amplification. Dose-limiting toxicities included diarrhea and nausea.
- The recommended phase II dose for neratinib was 160 mg/day for this combination. Loss of the HER2 receptor and high expression of p95HER2 may explain the resistance to HER2 antibodies.
DOI: 10.1200/JCO.19.00858 Journal of Clinical Oncology -
Pyrotinib vs Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer With Prior Taxanes, Anthracyclines, and/or Trastuzumab
- The authors of this randomized phase II trial evaluated capecitabine plus either lapatinib or pyrotinib, an irreversible pan-ErbB inhibitor, in 128 patients with HER2-positive relapsed or metastatic breast cancer previously treated with taxanes, anthracyclines, and/or trastuzumab. The overall response rate was significantly better with pyrotinib (78.5%) than with lapatinib (57.1%). The median progression-free survival was also superior at 18.1 versus 7 months (HR, 0.36; P<.001) for the pyrotinib and lapatinib arms, respectively.
- A randomized phase III trial is ongoing to confirm these encouraging results.
- https://www.practiceupdate.com/C/88420/56?elsca1=emc_enews_topic-alert
- https://ascopubs.org/doi/10.1200/JCO.19.00108
- DOI: 10.1200/JCO.19.00108 Journal of Clinical Oncology
-
Good News on Nipple-Sparing Breast Surgery
Korean study examined recurrence rates
Incidence of breast cancer recurrence in the nipple-areola complex (NAC) following nipple-sparing mastectomy (NSM) and immediate breast reconstruction was extremely limited over the long term, Korean investigators found, and cancers that did recur did not increase risk of distant metastases or compromise overall survival.
The findings suggest that biological features of the breast cancer tumor should be considered when planning nipple-sparing mastectomy.
https://jamanetwork.com/journals/jamasurgery/article-abstract/2749070
Wu Z, Kim H, Lee J, et al. Breast Cancer Recurrence in the Nipple-Areola Complex After Nipple-Sparing Mastectomy With Immediate Breast Reconstruction for Invasive Breast Cancer. JAMA Surg. Published online August 28, 2019. doi:10.1001/jamasurg.2019.2959
-
New drug approval by the FDA -- can be used in breast cancer
https://www.practiceupdate.com/c/88121/3/1/?elsca1...
-
{I looked up the article BevJen posted and thought I would add some highlights. Thx BevJen!}
FDA Approves Third Oncology Drug That Targets a Key Genetic Driver of Cancer, Rather Than a Specific Type of Tumor
The U.S. Food and Drug Administration today granted accelerated approval to Rozlytrek (entrectinib), a treatment for adult and adolescent patients whose cancers have the specific genetic defect, NTRK (neurotrophic tyrosine receptor kinase) gene fusion and for whom there are no effective treatments.
This is the third time the agency has approved a cancer treatment based on a common biomarker across different types of tumors rather than the location in the body where the tumor originated.
The ability of Rozlytrek to shrink tumors was evaluated in four clinical trials studying 54 adults with NTRK fusion-positive tumors. The proportion of patients with substantial tumor shrinkage (overall response rate) was 57%, with 7.4% of patients having complete disappearance of the tumor. Among the 31 patients with tumor shrinkage, 61% had tumor shrinkage persist for nine months or longer. The most common cancer locations were the lung, salivary gland, breast, thyroid and colon/rectum.
Rozlytrek was granted accelerated approval. This approval commits the sponsor to provide additional data to the FDA. Rozlytrek also received Priority Review, Breakthrough Therapy and Orphan Drug designation. The approval of Rozlytrek was granted to Genentech, Inc.
-
Checkpoint Inhibitors in the Neoadjuvant Treatment of Triple-Negative Breast Cancer
- Interview with Heather Lynn McArthur MD nterview by Farzanna S Haffizulla MD, FACP, FAMWA
- Discussion of new approaches to treating triple-Negative Breast Cancer
- September 02, 2019
- video and transcript - no charge, but sign in may be required.
- https://www.practiceupdate.com/C/84601/56?elsca1=emc_enews_topic-alert
-
Appreciate the additional info Lumpie, and also Bevgen signposting
-
New Target for Slowing Breast Cancer's Spread to Brain
scientists have identified a protein that plays a role in the metabolic reprogramming of some breast cancer cells, allowing them to survive when they spread to the brain... disabling this protein may represent a novel strategy to prevent and treat breast cancer brain metastases... The spread of breast cancer cells to the brain is correlated with the overexpression of human epidermal growth factor receptor 2 (HER2) in cancer cells, but the mechanisms driving this correlation were unknown. scientists combed through publicly available genomic databases, discovering that increased levels of the fatty acid-binding protein 7 (FABP7), a lipid-binding protein in the brain, correlated with lower survival and higher incidence of brain metastases in HER2-positive breast cancer patients. Notably, FABP7 is not found in elevated levels in the primary HER2-positive breast tumors, instead only found in tumor cells growing in the brain... In mouse models, the investigators found that disabling FABP7 prevented HER2-positive breast cancer metastasizing into the brain. FABP7 could be used in the future as a biomarker or therapeutic target for breast cancer patients. If high levels of FABP7 were detected in breast cancer patients, it might signal the patient is at risk for cancer spreading to their brain, and targeting or disabling FABP7 could be a promising strategy to prevent or treat breast cancer brain metastasis.
-
Total Chemo Dose Still Matters in Breast Cancer
Worse survival with cumulative dose <85% of planned
August 20, 2019
- Failure to achieve a threshold cumulative dose of adjuvant chemotherapy for early breast cancer correlated with worse survival, particularly when dose reductions occurred early in treatment, a retrospective review of 1,300 patients showed.Patients who received less than 85% of the planned total cumulative dose (TCD) had significantly worse 5-year disease-free survival (DFS, P=0.025) and overall survival (OS, P<0.001), as compared with patients who received 85% or more of the planned TCD. "What surprised us the most was how dramatically early reductions in chemotherapy affect survival compared to later modifications," ... "This became even more apparent when patients were further separated based on chemotherapy dose cutoffs. Often the first cycle of chemotherapy can be difficult for patients, and oncologists must convey the need for maintaining initial dose intensity, while using other medications to control side effects and manage comorbidities."
- https://www.medpagetoday.com/hematologyoncology/chemotherapy/81721
- Primary Source Journal of the National Comprehensive Cancer Network Source Reference: Veitch Z, et al "Impact of cumulative chemotherapy dose on survival with adjuvant FEC-D chemotherapy for breast cancer" J Natl Compr Canc Netw 2019; 17: 957-971.
-
{I generally refrain from posting alarmist, non-cancer-specific articles, but this is truly distressing, IMO, and not from flaky sources.}
How to Eat Less Plastic
Your food and water are contaminated with plastic. Here's why it's in the food system and how it could affect your health.
A recent study indicates that the average person consumes a credit card-sized amount of microplastics — the tiny particles of plastics we ingest by eating, drinking, and breathing — every week. The chemicals found in these plastics are linked to harmful health effects, like various cancers, weakened immune systems, and reproductive problems. Find out 6 ways you can reduce unnecessary exposure to potentially harmful plastics.
https://doi.org/10.1021/acs.est.9b01517
https://pediatrics.aappublications.org/content/142/2/e20181410
PubMed 30037972
https://cues.rutgers.edu/2019-microplastics-conference/2019-mpc-dwnld.html
https://www.consumerreports.org/food-safety/gras-hidden-ingredients-in-your-food/
-
[Discovery of] A molecule that regulates the development of cancer in a variety of human tumors [including breast]
Sonia Guil, leader of the Regulatory and Chromatin RNA group of Josep Carreras Leukemia Research Institute, and Lourdes Farré of ProCURE (Idibell) have discovered an intermediate molecule expressed from a region of the non-coding genome that is key to the development and differentiation of cells, and for the expansion of tumor cells...
The non-coding sequence that originates RPSAP52, is just "in front" of HMGA2. It has been discovered that it regulates the chain of events responsible for the increase in the number of tumor cells and the expansion of cancer tissues...
The study was carried out by combining in vitro approaches with in vivo studies on animal models. The tumorigenic role of RPSAP52 in breast and sarcoma tumors has been confirmed, and it can also have predictive value as a biomarker...
"For translational research, the findings are significant because these types of molecules are often present at low levels. Therefore they can be attacked and eradicated more easily than the coding genes," says Guil.
The next steps to move forward in this line of research will focus on generating in vivo tumor models and test small molecules that destroy RPSAP52 to study its effect on tumor growth.
Article: https://medicalxpress.com/news/2019-09-molecule-cancer-variety-human-tumors.html
-
Is there a reliable site for finding out about clinical trials as well as alternative treatments. I guess my onciologist should know about clinical trials. I may be facing round 3, and just do not think I can go through traditional treatment. For me it does not seem to work. 2009 lumpectomy, radiation, 2 nodes removed; tamoxifen for 5 years; 2016 bi-lateral, 2 nodes removed, cancer only on left side, I opted for bi-lateral, chemotherapy, started with arimidex and stopped after several months due to SE, several months later started tamoxifen. Now it looks like there might be something in the right axilla. The radiologist I just saw said she went through the notes and had been the one to examine the tissue fomr the bi-lateral, and the R-side was clean at that time. One problem with clinical trials, you do not know if you get the placebo or not.
-
I like this site for breast cancer clinical trials:
You can also go to
https://clinicaltrials.gov/ct2/home
Unless you are at a major research center or your MO has an interest in research, there is a good chance that s/he will not know about specific trials. MO's usually have a lot to keep up with and keeping tabs on the current recruitment status of hundreds of clinical trials may not be their thing. If you find one that you think may be suitable, you can always contact the trial for more info and/or ask your MO about it.
Please note, for stage IV clinical trials you should NEVER be given a placebo! Depending on the phase of study, you would either definitely be given the trial drug or you may be in a study comparing standard of care (or "physician's choice") to a new therapy. It is not an ethical practice to deprive stage IV patients of treatment.
Here's a link for more clinical trial info:
https://www.mbcalliance.org/mbc-alliance-cted This site provides links to additional good resources on clinical trials.
I don't do that much research on alternative treatments, but if I wanted to investigate, I would start with the web site for the National Associations for Naturopathic Doctors
https://aanmc.org/national-associations/
and look for info for the public on Basyr's site:
Also peer reviewed journals and nursing research may provide good information. Good luck!
-
Just reiterating Lumpie's point on stage IV trial patients.....at no point should a stage IV patient be given a placebo.... if that is even suggested bin the trial.
-
Breast cancer: Hormone therapy may only put some cells to 'sleep'
Published Tue 3 Sep 2019
https://www.medicalnewstoday.com/articles/326226.p... -
Proton Beam Radiation in Patients With Breast Cancer Requiring Regional Nodal Irradiation
- The authors of this phase II trial provide the first prospective evaluation of proton beam radiotherapy (RT) in breast cancer, evaluating proton beam RT in 70 patients with nonmetastatic breast cancer who required postoperative RT to the breast/chest wall and regional lymphatics but were considered suboptimal candidates for conventional RT. This approach was associated with low toxicity and similar rates of disease control compared with historical conventional radiotherapy data.
- With better awareness of cardiac morbidity in this patient population, confirmation of these findings in a randomized phase III trial (RadCOMP Consortium Trial) will be important.
CONCLUSION: Proton beam RT for breast cancer has low toxicity rates and similar rates of disease control compared with historical data of conventional RT. No early cardiac changes were observed, which paves the way for randomized studies to compare proton beam RT with standard RT.
https://www.practiceupdate.com/C/88796/56?elsca1=emc_enews_topic-alert
https://ascopubs.org/doi/10.1200/JCO.18.02366
DOI: 10.1200/JCO.18.02366 Journal of Clinical Oncology
-
More targeted, less toxic: The golden future of cancer treatment
Researchers have engineered gold-based molecules that target cancer cells and leave healthy cells unharmed, in a critical step towards precision cancer drugs with fewer toxic side effects. Pre-clinical studies have shown the molecules were up to 24 times more effective at killing cancer cells than the widely used anti-cancer drug cisplatin and were also better at inhibiting tumour growth...
Significantly, the synthetic molecules are built with resistance-fighting features to keep them effective over time, unlike current chemotherapies.
The study by researchers at RMIT University, detailing four new bio-active molecules and their effectiveness against five types of cancer cells [prostate, breast, cervical, melanoma and colon cancer], is published in Chemistry—A European Journal...
In addition, the molecules have strong anti-inflammatory properties, giving them a dual therapeutic effect and potential application in the treatment of chronic inflammatory conditions like arthritis...
The research team has completed successful in vitro and in vivo pre-clinical studies and is seeking funding to support the next stage of the research—clinical studies and regulatory approval.
Article: https://medicalxpress.com/news/2019-09-toxic-golden-future-cancer-treatment.html
Study: https://onlinelibrary.wiley.com/doi/abs/10.1002/chem.201903388
-
Opinion: Are 71 NCI-Designated Cancer Centers Too Many?
In an opinion piece in The Scientist, David Rubensen argues that the National Cancer Institute (NCI) designated cancer center program "has evolved into a nationwide branding exercise, mostly signifying grant-writing endurance and adherence to metrics that skew scientific priorities and place centers in organizational straight jackets." He suggests questions that he believes should be addressed about the future of the program.
-
Durvalumab in Combination With Trastuzumab in HER2‐Positive Metastatic Breast Cancer - no clinical activity
- This phase Ib trial was designed to evaluate the toxicity and activity of durvalumab in combination with trastuzumab among 14 patients with previously treated HER2-positive metastatic breast cancer (MBC). There was no significant activity observed with this regimen among HER2-positive, PD-L1–negative patients; 29% of patients experienced stable disease at 6 weeks.
- Durvalumab in combination with trastuzumab demonstrated no clinical activity among patients with heavily pretreated HER2‐positive PD‐L1–negative MBC.
doi:10.1634/theoncologist.2019-0321 -
Metronomic Chemotherapy for Advanced Breast Cancer
Metronomic chemotherapy (mCHT) refers to the minimum biologically effective dose of a chemotherapy agent given as a continuous dosing regimen, with no prolonged drug-free breaks, that leads to antitumor activity. Aim of the present study is to describe the use of mCHT in a retrospective cohort of metastatic breast cancer (MBC) patients in order to collect data regarding the different types and regimens of drugs employed, their efficacy and safety.
- This retrospective study is a real-world analysis of metronomic chemotherapy for patients with metastatic breast cancer. The highest overall response rate was observed among patients receiving vinorelbine-based regimens. The median time to treatment failure was 6.28 months. The longest median progression-free survival was observed with vinorelbine-based regimens (9.5 months) and capecitabine as a single agent (10.7 months).
- The authors provide real-world data to inform the use of metronomic chemotherapy among patients with metastatic breast cancer.
-
One MO doing this is Dr Keith Block in the Chicago area. He is able to treat people who other MOs think have had too much chemo or are too weak for more, by giving a low dose over 24 hours from a fanny pack. (And other innovative deliveries.) Also the chemo can be pulsed when it is most bioavailable/when the cancer is the most active in the 24 hour circadian clock aka "chronomodulation." I actually found out that Taxotere is most bioactive at 5-6 am and carboplatin at 4 pm. (I emailed a researcher in London to find this out.) So I got my Taxotere at 8 am and my carboplatin at 4 pm. They just taped me off in between.
-
santabarbarian: Thanks for sharing your experience. This is an interesting approach and I suspect that it may allow those not otherwise able to tolerate chemo to benefit from this therapy. I have known patients who received low(er?) dose continuous infusion, namely, pregnant women, and have wondered if alternative approaches to the more "usual" infusion schedules had been studied in others.
-
I would like to contribute a bit, my first try here among all these incredibly helpful posts... I hope this may be interesting...
There is a promising agent being tested here in the EU, called MitoTam, which is a mitochondrialy targeted Tamoxifen. It has just entered phase II trials
https://cancerres.aacrjournals.org/content/79/4_Supplement/P6-18-20
Mentioned in this article: Mitochondrial Flexibility of Breast Cancers: A Growth Advantage and a Therapeutic Opportunity
-
Study confirms low fat diets benefit women's health
Published Mon 9 Sep 2019
By Ana Sandoiu
Fact checked by Gianna D'Emilio
New research spanning over almost 2 decades finds that a low fat diet benefits women's health.
A low fat diet that includes lots of fruits and vegetables benefits women's health in the long run, according to new research.
Older studies in rats and mice have found that rodents on a high fat diet develop more tumors than those on a low fat diet.
Some of these studies referred to colorectal cancer in particular, while othersshowed that high fat diets boosted tumor growth in mouse models of breast cancer.
More recently, studies in humans have suggested that following a low fat dietary plan could improve the health and lifespan of women who have received a diagnosis of breast cancer.
Read more athttps://www.medicalnewstoday.com/articles/326286.p...
-
Axillary dissection in patients with preoperative positive nodal cytology: Genuine need or overtreatment?
- This retrospective study was designed to characterize nodal burden among breast cancer patients with axillary nodal metastases detected by ultrasound‐guided fine‐needle aspiration cytology (US‐FNAC) undergoing axillary dissection. Patients with one or two nodes had favorable pathologic characteristics, including a smaller primary tumor, a lower proportion of grade 3 invasive lobular disease, and a high proportion of low-Ki67 tumors. The median number of metastatic nodes was five. Among patients with clinically negative axilla, 50% had four or more metastatic nodes and 31% had fewer than three metastatic axillary nodes.
- Approximately one-third of patients with clinically negative axilla with positive axillary US-FNAC performed due to imaging results have fewer than three metastatic axillary nodes and hence could avoid axillary dissection, per the current guidelines.
https://www.practiceupdate.com/C/88865/56?elsca1=emc_enews_topic-alert
DOI: 10.1111/tbj.13479
-
Thanks JaBoo. That sounds encouraging.
-
Why Aren't Cancer Drugs Better? The Targets Might Be Wrong
Drugs can stop cancer cells if they attack the right proteins. But many of these targets were chosen with dated, imprecise technology, a new study suggests.
{NYT generally allows access to a limited number of articles per month without a subscription.}
-
Scientists have determined a new way to protect the hair follicle from [taxane] chemotherapy in an effort to prevent hair loss as a result of cancer treatments.
...we found that CDK4/6 inhibitors can be used temporarily to halt cell division without promoting additional toxic effects in the hair follicle. When we bathed organ-cultured human scalp hair follicles in CDK4/6 inhibitors, the hair follicles were much less susceptible to the damaging effects of taxanes..."
The team hope that their work will support the development of externally applicable medicines that will slow or briefly suspend cell division in the scalp hair follicles of patients undergoing chemotherapy to mitigate against chemotherapy-induced hair damage. This could complement and enhance the efficacy of existing preventive approaches i.e. scalp cooling devices.
Article: https://www.sciencedaily.com/releases/2019/09/190912120535.htm
Reference: https://www.embopress.org/doi/full/10.15252/emmm.201911031
-
Breast cancer cells 'stick together' to spread through the body during metastasis
"The good news," he says, "is that our study reveals that the process of metastasis, even in ideal laboratory settings, appears to be exceedingly inefficient." Research suggests that about 99% of cells that leave primary tumors die and never form new tumors.
https://www.sciencedaily.com/releases/2019/09/1909... -
Breast cancer cells 'stick together' to spread through the body during metastasis
"The good news," he says, "is that our study reveals that the process of metastasis, even in ideal laboratory settings, appears to be exceedingly inefficient." Research suggests that about 99% of cells that leave primary tumors die and never form new tumors.
https://www.sciencedaily.com/releases/2019/09/1909... -
How breast cancer uses exosomes to metastasize to the brain
...In the case of cancer cells, EVs [extracellular vesicles, a.k.a. exosomes] carry factors that help create a more hospitable environment for both the primary tumor and its metastases, as Moses and Morad detailed recently in a review article. Primary tumors can secrete EVs into the circulation, allowing them to travel to distant organs and help spread the cancer.
"The main question we had was, how can EVs reach the brain in the first place?" says Morad. "The blood brain barrier doesn't allow anything larger than 400 daltons to passively get into brain tissue. Exosomes are more than two thousand times larger than the size cutoff limit."
...Bottom line, Morad and Moses showed, for the first time, that rather than squeezing in between the cells in the BBB to get into the brain, the EVs trick the endothelial cells into taking them up. Using a standard biological pathway called transcytosis, the cells simply engulfed the EVs, bringing them inside and releasing them into brain tissue like so many Trojan horses...
Having discovered what EVs do to help breast cancer metastasize to the brain, the Moses Lab hopes to turn the tables -- and use EVs (or synthetic versions) to deliver anticancer drugs that home to the metastatic site.
Article: https://www.sciencedaily.com/releases/2019/09/190912153454.htm
Reference: https://pubs.acs.org/doi/10.1021/acsnano.9b04397
-
Gaps Exist In Understanding of Genomic Tests
A majority of cancer patients don't understand key aspects of the genomic test results they receive as participants in biomarker-driven clinical trials, according to a first-of-its-kind pilot study...
September 9, 2019
-
Study backs genetic testing for all metastatic breast cancer patients
Genetic testing for all metastatic breast cancer patients may be an optimal strategy for identifying additional patients with increased risk as well as response to targeted therapies, according to research published Aug. 29 in JAMA Oncology.
In the study, 100 patients were tested regardless of whether they met the current National Comprehensive Cancer Network (NCCN) guidelines. Among the 14 patients who did test positive for a pathogenic or likely pathogenic variant, 43% (six patients) did not meet the NCCN guidelines.
The study has clinical significance because of the recent approval of a PARP inhibitor for patients with HER2/ERBB2 negative breast cancer with germline BRCA1 and BRCA2 pathogenic variants.
The U.S. Food and Drug Administration in October 2018 approved the PARP inhibitor talazoparib for that breast cancer.
"We found almost twice as many mutations than what we would have found if we adhered to NCCN guidelines, and some of those patients could go on clinical trials that could therapeutically help their disease,"Participants in the study included 76 white patients, 12 black patients, six Asian patients, three Hispanic patients and three of other racial/ethnic identification. Two of the patients were male.
Sep. 5, 2019
-
Liquid biopsies reveal genetic alterations linked to cancer drug resistance
A clinical study comparing liquid and tissue biopsies finds multiple resistance mechanisms in individual patients, which could explain why targeted therapies often fail.
Many patients see their tumors shrink in response to a drug, only to have them come back with a vengeance as they evolve to fend off the treatment. Oncologists want to be able to quickly detect cancer drug resistance as it emerges in their patients and identify another drug the tumors will still respond to.
"This study is the largest to date to directly compare liquid biopsy to tumor biopsy in the setting of cancer resistance," said Corcoran. "Our findings suggest that liquid biopsy may be the preferred clinical modality for assessing how patients' tumors have evolved after they've become resistant to therapy."
Although this new study turned up some tantalizing findings, the authors emphasize that larger, more comprehensive efforts are needed to fully understand cancer drug resistance. "To really map out the full landscape of cancer resistance mechanisms, we need much larger studies that span a variety of drugs and cancer types,"
https://www.broadinstitute.org/news/liquid-biopsie...
https://www.nature.com/articles/s41591-019-0561-9
Nature Medicine volume 25, pages1415–1421 (2019)
DOI -
Many Cancer Drugs Don't Work Like Scientists Say They Do, New Study Suggests
Cancer therapies often fail to work when tested in clinical trials. As a result, a startling 97 percent of drugs designed for specific cancer treatments do not receive approval from the Food and Drug Administration. Now researchers say they may have figured out part of the reason why.
Drugs may not do what we think they do
The majority of proposed anticancer treatments do not succeed in advancing to clinical use because of problems with efficacy or toxicity, often for unclear reasons. Lin et al. discovered that a drug candidate in clinical development was effective at killing cancer cells even when its target protein was knocked out, suggesting that its proposed mechanism of action was incorrect. The researchers then identified multiple drugs with similar problems and also discovered the correct target for one of them, suggesting that more research and more stringent methods are needed to verify the targets of potential drugs before advancing them to the clinic.
http://blogs.discovermagazine.com/d-brief/2019/09/...
https://stm.sciencemag.org/content/11/509/eaaw8412
DOI: 10.1126/scitranslmed.aaw8412
-
Bias against single people affects their cancer treatment
New research reveals the dangerous bias that's been buried in the fine print of academic and medical journals for more than 30 years. Unmarried patients with cancer are less likely to get potentially life-saving surgery or radiotherapy than their married counterparts, as medical providers may rely on stereotypes that discount sources of social support other than a current spouse.
Although this disparity has been attributed in studies to such factors as patients' treatment preferences or a weaker will to live among unmarried people, DelFattore found that those speculations are not only unsupported by data but actually conflict with extensive research findings. Rather, her article suggests that cultural stereotypes inappropriately influence the treatments recommended for unmarried patients with cancer.
it's been known since at least 1987 that cancer patients with a current spouse are more likely to get surgery or radiotherapy than those who are divorced, separated, widowed or never married.. It's about asking people to examine their assumptions -- in this case, with respect to potentially life-or-death decisions. Medicine has to evolve, not only in science and technology, but also with respect to an evolving society."
https://www.sciencedaily.com/releases/2019/09/1909...
Joan DelFattore. Death by Stereotype? Cancer Treatment in Unmarried Patients. New England Journal of Medicine, 2019; 381 (10): 982 DOI: 10.1056/NEJMms1902657
-
FDA: Novel Breast Ca Drugs Linked to Severe Lung Illness
Reports of ILD, pneumonitis in patients on CDK4/6 inhibitors
The FDA issued a warning Friday that CDK4/6 inhibitors for advanced breast cancer may cause rare but severe lung inflammation, and said fatalities had been reported. Package warnings have been added to the three approved agents in the class -- palbociclib (Ibrance), ribociclib (Kisqali), and abemaciclib (Verzenio) -- and breast cancer patients taking these agents should be monitored for pulmonary symptoms indicative of either pneumonitis or interstitial lung disease (ILD).
https://www.medpagetoday.com/hematologyoncology/br...
https://www.fda.gov/drugs/drug-safety-and-availabi...
-
Docs Want Say in How Prior Authorizations Work
"You would have much greater buy-in from physicians," House panel told
Practicing doctors should have input when it comes to deciding how prior authorization processes should work, an expert told members of a House committee on Wednesday. "Instead of pharmacy benefit managers deciding on how best to administer prior authorizations, have the physicians who are at the point of the spear weigh in," "The American Academy of Dermatology would love to have seat at the table in terms of defining what's reasonable in terms of different treatment algorithms, and you would have much greater buy-in from physicians if we could have that sort of collaborative arrangement." Rogers spoke at a House Small Business Committee hearing on the burdens to physician practices posed by prior authorization and step therapy.
https://www.medpagetoday.com/practicemanagement/re...
-
Lumpie - Interesting comment on DRs wanting more say in how prior authorizations should work. 11 days ago my oncologist ordered a PET scan. The clinic is still waiting for authorization from my health insurance.
-
BlueGirlRedState: That is so frustrating! 11 days! what are they thinking? The article made several other interesting points:
"There are Centers of Excellence that are having 90% of their prior authorization denials overturned on appeal"
Public dissemination of the utilization parameters that insurers use also would help, "since often they're not using national standards,"
"... generics should not have to go through the prior authorization process,"
Physicians who are in alternative payment models should be entirely exempt from prior authorizations... "We're being paid for the quality we deliver and there should be no prior authorization for those practices." {They are not being paid by the service! But insurance still wants to ration and delay care?!?! Who cares what the docs order as long as it is not unethical or dangerous!}
I have heard from many compatriots that their insurance is notorious for failing to pre-auth PET scans. Wishing you good luck with yours!!
-
https://www.yahoo.com/lifestyle/early-breast-cance...
Anyone heard of the iBreastExam?
-
Wow, Bounce, this is the first I've heard of it... how exciting! Comparable sensitivity to mammos without any radiation! The article says that it doesn't pick up microcalcifications, but one could keep one's mammo schedule and add additional scans with the iBreastExam to pick up any lumps earlier.
-
A cohort study of breast cancer risk after 20 years of follow-up of women treated with fertility drugs
Sonia Guleria, Susanne K. Kjaer, Vanna Albieri, Kirsten Frederiksen and Allan JensenDOI: 10.1158/1055-9965.EPI-19-0652Abstract
Background: Using a nationwide cohort of Danish women, we investigated the association between use of fertility drugs and risk of breast cancer. Methods: The study cohort included women aged 20-44 years and living in Denmark between 1 January 1995 and 31 December 2011. Information on fertility status, use of fertility drugs, breast cancer, covariates and vital status was obtained from the Danish Infertility Cohort and various Danish national registers. Cox proportional hazard regression models were applied to estimate hazard ratios (HRs) and 95% confidence intervals (CIs), adjusted for potential confounders. Results: Of the 1,330,852 women included, 96,782 (7.3%) were infertile, and 20,567 (1.5%) were diagnosed with breast cancer during a median follow-up of 20.9 years. Compared with fertile women, infertile women who had used any fertility drugs did not have an increased hazard for breast cancer overall (HR 1.02; 95% CI 0.95-1.10), or for any of the histological types (ductal, lobular or mucinous) of breast cancer. Furthermore, no associations were observed between use of specific types of fertility drugs and breast cancer. Conclusions: No convincing associations between use of fertility drugs and breast cancer were observed after two decades of follow-up. Impact: Our results do not support a marked association between fertility drugs and breast cancer and are therefore reassuring for infertile women treated with fertility drugs.
- Received June 7, 2019.
- Revision received August 12, 2019.
- Accepted September 12, 2019.
-
HER2-Positive Breast Cancer
Fixed-Dose Subcutaneous Pertuzumab Combo Shows Noninferiority in HER2+ Breast Cancer
The fixed-dose subcutaneous injection formulation plus intravenous chemotherapy had noninferior pharmacokinetics versus standard IV infusions of the regimen in patients with HER2-positive early disease.
FDA Accepts sNDA for Neratinib Combo for HER2+ Breast Cancer
Neratinib could become available for use in combination with capecitabine for select pretreated patients with HER2-positive metastatic disease.
Novel Approaches Push the Envelope in HER2+ Breast Cancer
Douglas K. Marks, MD, discusses key developments in the HER2-positive breast cancer space.
Pyrotinib Combo Delays Progression in Heavily Pretreated HER2+ Breast Cancer
A phase III trial is now being conducted to evaluate the efficacy and safety of this regimen compared with lapatinib/capecitabine.
-
VERY IMPORTANT FINDINGS FOR MEN
Poor treatment outcomes, poorer survival.
Question To what extent are clinical characteristics and treatment patterns associated with the survival difference between male and female patients with breast cancer?
Findings In this large cohort study of 16 025 male and 1 800 708 female patients with breast cancer in the United States, the male patients had 19% higher fully adjusted overall mortality compared with their female counterparts. Clinical characteristics and undertreatments were associated with 63.3% of the excess mortality among male patients.
Meaning These results suggest a need for further research into biological features of breast cancer and tailored treatments for men with the disease to mitigate the sex-based disparity in mortality.
https://jamanetwork.com/journals/jamaoncology/article-abstract/2751525
Conclusions and RelevanceThis study found that mortality after cancer diagnosis was higher among male patients with breast cancer compared with their female counterparts. Such disparity appeared to persist after accounting for clinical characteristics, treatment factors, and access to care, suggesting that other factors (particularly additional biological attributes, treatment compliance, and lifestyle factors) should be identified to help in eliminating this disparity.
-
For those who use turmeric, this is worth reading
- Summary:
Turmeric adulteration with lead chromate was assessed in Bangladesh.
- •
Turmeric Pb concentrations exceeded the national limit by up to 500 times.
- •
Evidence of turmeric adulteration was found in 7 of 9 turmeric-producing districts.
- •
Turmeric adulteration was found to be driven by consumer demand for yellow roots.
https://www.sciencedirect.com/science/article/pii/S0013935119305195?via%3Dihub
-
Hardly surprising, but:
Surgical technique helps breast cancer patients avoid repeat surgeries
In breast cancer surgery, taking just a little bit more healthy tissue initially can help patients avoid a return trip to the operating room...
"What we found in the study, by just taking a little more tissue, we could reduce the positive margin rate by 50 percent. It's very exciting," Chagpar said.
-
Interesting and as you say, not surprising. At my hospital, they send the excision for examination DURING surgery. For me, they found they needed to take a bit more and did it right then. So it was one surgery. Takes a bit longer that way but still better than doing repeat surgery.
-
After needing a re-excision in 2016, I told my BS in 2018 to "go big." :-)
-
Before I went under for my excisional biop, I told my surgeon as well to "go big". When I woke up, he told me the margins were "close but clear".
So far so good.
Claire in AZ
-
MIT AI tool can predict breast cancer up to 5 years early, works equally well for white and black patients
MIT's Computer Science and Artificial Intelligence Lab has developed a new deep learning-based AI prediction model that can anticipate the development of breast cancer up to five years in advance. Researchers working on the product also recognized that other similar projects have often had inherent bias because they were based overwhelmingly on white patient populations, and specifically designed their own model so that it is informed by "more equitable" data that ensures it's "equally accurate for white and black women."
https://techcrunch.com/2019/06/26/mit-ai-tool-can-...
{Thanks Ingerp for forwarding this link.}
-
New blood test could detect more than 20 types of cancer
- Laura Donnelly, health editor
Anew blood test could detect more than 20 types of cancer, allowing cases to be identified and treated far earlier.
Experts said the breakthrough - which spots changes in the genes, as disease develops - could be used to improve screening for cancer, allowing treatment much sooner, when it is more likely to succeed.
Crucially, 99.4 per cent cases identified as cancer were correctly spotted - meaning just 0.6 per cent of cases were misdiagnoses of healthy patients.
The test was able to detect one third of patients with stage one disease, and three quarters of those with stage two disease.
Ministers have pledged to speed diagnosis, so that by 2028 three quarters of cancer patients are diagnosed at these two stages. Currently just half of patients can expect to receive a diagnosis before they reach stage three or four.
The advances, by US scientists, look for abnormal patterns of methylation in the DNA, which can indicate different types of cancer.
The study found the new method could even pinpoint the cancer source nearly 90 per cent of the time, including for diseases like ovarian and pancreatic disease, which are some of the most difficult to spot.
Study lead author, Dr Geoffrey Oxnard of Boston's Dana-Farber Cancer Institute, part of Harvard Medical School, said: "Our work indicated that methylation-based assays outperform traditional DNA-sequencing approaches to detecting multiple forms of cancer in blood samples.
"The results of the new study demonstrate that such assays are a feasible way of screening people for cancer."
In the study, researchers analysed cell-free DNA - which enters the bloodstream after becoming detached when its parent cell dies - in more than 3,500 blood samples.
The samples were taken from more than 1,500 cancer patients and more than 2,000 from people without cancer.
The patient samples comprised more than 20 types of cancer, including hormone receptor-negative breast, colorectal, oesophageal, gall bladder, gastric, head and neck, lung, lymphoid leukaemia, multiple myeloma, ovarian, and pancreatic cancer.
The test accurately detected 76 per cent of high mortality cancers.
Within this group, the test accuracy was 32 per cent for patients with stage one cancer; 76 per cent for those with stage two; 85 per cent for stage three; and 93 per cent for stage four.
Dr Oxnard said: "Detecting even a modest percent of common cancers early could translate into many patients who may be able to receive more effective treatment if the test were in wide use."
The research was presented today at the European Society for Medical Oncology Congress in Barcelona, Spain.
Britain is bottom of international league tables for cancer survival, with rates two decades behind some countries for some types of disease.
This week an independent review of NHS cancer screening will warn that "confusion and delays" is costing lives, as it calls for for Public Health England to be stripped of responsibility for the service.
Former cancer tsar Prof Sir Mike Richards was asked to examine the system following a series of scandals and a sharp decline in uptake of checks for breast, bowel and cervical disease.
-
Adjuvant Chemotherapy ± Trastuzumab in Patients With T1, Node-Negative HER2-Positive Breast Cancer
- This retrospective analysis evaluated long-term survival data for patients with T1N0 HER2-positive breast cancer treated with adjuvant chemotherapy with or without trastuzumab. The addition of trastuzumab was found to provide benefit for patients with tumors at least 0.8 cm in size.
- The study authors concluded that adjuvant therapy with trastuzumab may not be required for tumors less than 0.8 cm in size.
https://www.practiceupdate.com/C/89468/56
https://clincancerres.aacrjournals.org/content/ear...
DOI: 10.1158/1078-0432.CCR-19-0463
-
Antibiotic use before cancer treatment cuts survival time – study
Patients live longer if they do not take antibiotics in month before (Checkpoint Inhibitor) immunotherapy
https://www.theguardian.com/society/2019/sep/12/an...
Taking antibiotics in the month before starting immunotherapy dramatically reduces a cancer patient's chances of survival, according to a small but groundbreaking study.
Scientists at Imperial College London believe antibiotics strip out helpful bacteria from the gut, which weakens the immune system. This appears to make it less likely that immunotherapy drugs will boost the body's cancer-fighting capability.
In their study of nearly 200 cancer patients in two NHS hospitals, the researchers found that those who had taken broad-spectrum antibiotics for just a few days for common problems such as chest infections survived for a median of two months after immunotherapy, compared with 26 months for those who had not been on antibiotics.
Study published in the journal Jama Oncology
https://www.theguardian.com/society/2019/sep/12/an...
https://jamanetwork.com/journals/jamaoncology/arti...
doi:10.1001/jamaoncol.2019.2785
{Not breast cancer specific but concerning.}
-
A twice daily helping of onions and garlic could reduce the risk of breast cancer by a massive 67 per cent, a study reveals.
...In their new study, scientists wanted to examine the association between onion and garlic consumption and breast cancer in Puerto Rico.
The researchers, from the University at Buffalo (UB) and the University of Puerto Rico, chose to study a group of Puerto Rican women who eat lots of onions and garlic which are key ingredients in sofrito, stews, and rice dishes.
Lead study author Gauri Desai, a PhD student from the University at Buffalo, said: "We found that among Puerto Rican women, the combined intake of onion and garlic, as well as sofrito, was associated with a reduced risk of breast cancer. "In fact, those who consumed sofrito more than once per day had a 67 per cent decrease in risk compared to women who never ate it.
-
The Big Three Misdiagnosed Cases: Cancers, Vascular Events, & Infections
Recently, a study investigating misdiagnosis-related harms was published in the medical journal, Diagnosis, the official journal of the Society to Improve Diagnosis in Medicine (SIDM)... findings ... were ...presented at a Capitol Hill briefing ...in order to bring awareness and inspire healthcare-related changes when it comes to the serious harms of misdiagnosis.
The study identified "The Big Three" when it comes to misdiagnosis, and more specifically, misdiagnosis-related harms. These Big Three included cancers, vascular events, and infections.
{Findings} suggest that not only are the Big Three common in misdiagnosis situations, but they are also often associated with some of the most serious outcomes... nearly 38% were related to cancers... cancer-related misdiagnosis events were most commonly reported in the outpatient or clinic setting.
The researchers and the SIDM are hoping to use this information to inspire change and targeted initiatives in specific settings to help reduce misdiagnosis and misdiagnosis-related harms. The team of researchers are working on two more follow-up studies...
https://advancedbreastcancer.net/clinical/misdiagn...
-
I wish we could find a cure to debunk this, but it rings terribly true
"Treating cancer with anything that actually works has been entirely outlawed in the United States, where 'healing has become a crime,' say independent observers. The conventional cancer industry isn't interested in curing the disease; it's interested in profiting from its continuation."
-
Kanga the banner ad atop the article tells me this is a dubious source.
-
Thanks Santabarbarian, still I think it’s worth the read to get different perspective - there is a lot of distrust out there of big pharma and how they sway health policy in their favour, rather than the patient’s. Cancer research is profit driven
-
BigPharma conducts financial analyses of any potential new drugs and only pursues the profitable ones (nowadays, primarily by buying out startups rather than conducting early research themselves). That means a lot of promising drugs for cancer and many other diseases languish. But that statement about outlawing cures by "independent observers" was not supported in any way. It's not that I trust BigPharma; companies will do what they can to protect their profits, including ethically iffy tactics like pay-for-delay of generics. We need to try to balance the corporate incentives with publicly funded research.
BTW, I was talking to a semi-retired biotech lawyer last night. He thinks that due to costs in the US and government support in China, most drug development will be conducted in China within the next ten years. Even if that is true, profits for those companies would still drive the selection of potential drugs.
-
Long‐Term Survival of De Novo Stage IV Human Epidermal Growth Receptor 2 (HER2) Positive Breast Cancers Treated with HER2‐Targeted Therapy
Background.
An increasing proportion of human epidermal growth receptor 2 (HER2) positive (HER2+) metastatic breast cancer (MBC) is diagnosed as de novo stage IV disease. We hypothesize that a subset of these patients who achieve no evidence of disease (NED) status after multimodality HER2‐targeted treatments may have prolonged progression‐free survival (PFS) and overall survival (OS).
Materials and Methods.
Patients with de novo stage IV, HER2+ MBC (n = 483) diagnosed between 1998 and 2015 were identified at two institutions (Yale and MD Anderson Cancer Centers). Clinical variables, treatment details, and survival outcomes were compared between those who achieved NED and those who did not.
Results.
All patients received trastuzumab, and 20% also received pertuzumab as first‐line therapy. The median OS was 5.5 years. Sixty‐three patients (13.0%) achieved NED; their PFS and OS rates were 100% and 98%, respectively, at 5 years and remained the same at 10 years. For patients with no NED (n = 420), the PFS and OS rates were 12% and 45% at 5 years and 0% and 4% at 10 years, respectively. NED patients more frequently had solitary metastasis and surgery to resect cancer . In multivariate analysis, NED status and estrogen receptor positive status were associated with prolonged OS.
Conclusion.
Among patients with de novo stage IV, HER2+ MBC, those who achieve NED status have a very high PFS and OS. Further randomized studies are required to fully understand the impact of systemic or locoregional therapy on achieving these excellent long‐term outcomes.
Implications for Practice.
In this retrospective review at two institutions, it was demonstrated that 13% of patients with de novo stage IV, human epidermal growth receptor 2 positive metastatic breast cancer achieved no evidence of disease (NED) status with trastuzumab‐based therapy plus/minus local therapies, and these patients had a very high progression‐free survival (100%) and overall survival (98%) at both the 5‐ and 10‐year time points. Achieving NED status may be an important therapeutic goal. However, further randomized studies are required to fully understand the impact of systemic or locoregional therapy on achieving these excellent long‐term outcomes.
Published online before print August 23, 2018. The Oncologist
http://theoncologist.alphamedpress.org/content/ear...
doi: 10.1634/theoncologist.2018-0213
{Confidence intervals and hazard ratios were deleted for readability. Please see abstract or full article for more details.} -
Debbew: That is interesting about development moving to China. If true, it seems sad for our talented and experienced researchers here. Development has to be distinguished from production, but given recent safety and quality issues with drugs - not to mention supply chains - it raises questions about quality assurance and and the supply of critical medications.
There is no doubt that therapies that are not likely to be quite profitable are often not researched. Some of that, for better and/or worse, has been addressed by the orphan drug act. Other research needs to be publicly funded. There are a few organizations out there working to distribute low margin drug through public service or low profit corporations/organizations. I'll see if I can find some coverage. It's an interesting model.
-
I was reading a report that marijen posted yesterday. IMHO, this is knock-your-socks-off news. This type of test could allow earlier, non-invasive, accurate diagnoses which can be extremely difficult with certain types of cancer. The post was very thorough but I wanted to post a link in case anyone is interested in that or needs it later:
New blood test capable of detecting multiple types of cancer
- Date:
- September 28, 2019
- Source:
- Dana-Farber Cancer Institute
- Summary:
- A new blood test in development has shown ability to screen for numerous types of cancer with a high degree of accuracy, a trial of the test shows.
- https://www.sciencedaily.com/releases/2019/09/1909...
- Dana-Farber Cancer Institute. (2019, September 28). New blood test capable of detecting multiple types of cancer. ScienceDaily. Retrieved September 28, 2019 from www.sciencedaily.com/releases/2019/09/190928082724...
-
A Superstar Team of Hospitals Is Sick of High Drug Prices—And Launching a Nonprofit Drug Company to Fight Them
By Sy MukherjeeSeptember 6, 2018
...a number of leading U.S. health systems announced an ambitious project: They would be banding together to create a non-profit generic drug company in the hopes of combating sky high drug prices and shortages regularly faced by American patients.
Civica Rx is a joint effort by big names like Catholic Health Initiatives, HCA Healthcare, Intermountain Healthcare, Providence St. Joseph Health, the Mayo Clinic, SSM Health, and Trinity Health. Those seven massive systems encompass about 500 American hospitals and will comprise the initial governing board of the group, which says it has attracted the interest of "more than 120 health organizations representing about a third of the nation's hospitals."
https://fortune.com/2018/09/06/civica-rx-nonprofit...
This article is considerably older:
Nonprofit vows to lower generic drug costs
By Robert Weisman {Boston} Globe Staff,December 13, 2015
https://www.bostonglobe.com/business/2015/12/13/no...
{May require subscription to access}
Also reported upon here:
A U.S. nonprofit says it has a better way to make generic drugs
by EJ Lane | Oct 7, 2015
https://www.fiercepharma.com/manufacturing/a-u-s-n...
-
'Out here, it's just me': In the medical desert of rural America, one doctor for 11,000 square miles
He was the only working doctor left to care for three remote counties east of El Paso, an area similar in size to the entire state of Maryland, home to far-flung oil encampments, a desolate stretch of interstate, communities of drifters living off the electric grid, and highway towns made up of truck stops and budget motels. "A wild place of last resort," was how Garner described parts of his territory, and for every person in every kind of medical trouble, the true last resort was him.
In the medical desert that has become rural America, nothing is more basic or more essential than access to doctors, but they are increasingly difficult to find. The federal government now designates nearly 80 percent of rural America as "medically underserved." It is home to 20 percent of the U.S. population but fewer than 10 percent of its doctors, and that ratio is worsening each year because of what health experts refer to as "the gray wave." Rural doctors are three years older than urban doctors on average, with half over 50 and more than a quarter beyond 60. Health officials predict the number of rural doctors will decline by 23 percent over the next decade as the number of urban doctors remains flat.
https://www.washingtonpost.com/national/out-here-i...
{Article addresses lack of access to medical care in rural areas of the U.S. WaPo may limit access without a subscription.}
-
Second generation antihistamines after breast cancer diagnosis to improve prognosis both in patients with ER+ and ER- breast cancer.
Background: Subgroups of patients with breast cancer (BC) could be candidates for immunological interventions. In the present investigation the role of antihistamines on prognosis of breast cancer has been studied, especially comparing first and second generation H-1 receptor antagonists due to their possible different effects on cytokines.
Methods: The study includes all women with BC diagnosed in Sweden 2000 through 2008 (n = 54406). Dates of birth, BC diagnosis and TNM-stage were directly extracted from the cancer registry. Therapy with antihistamines was gathered from the Swedish Prescription Registry. Other registries utilised were the Cause of Death Registry, Population Registry, and the in patient or out patient registries. BC and overall survival was compared between users of antihistamines and non users. Analyses were adjusted for TNM-stage, receptor status and age at diagnosis. A late entry model was used for different types of antihistamines.
Results: The HR for BC specific survival for the combined group of antihistamine users (n = 9777) was 0.70 (0.66-0.75). All the effect was seen for use after BC diagnosis. Results remained after adjusting for out or in patient diagnoses of allergy. In late entry models women using desloratadine (n = 1895) had a HR of 0.69 (0.52-0.91). Loratadine users (n = 2132) HR of 0.74 (0.60-0.93). Cetirizine users (n = 3001) HR of 1.13 (0.96-1.33) and Klemastine users (n = 2278) had a HR of 0.98 (0.80-1.19). Ebastin users (n = 326) had a HR of 0.50 (0.22-1.12) and Fenofexadine users (n = 145) had a HR of 0.73 (0.30–1.76). The analyses was also stratified for ER-status, but the results did not differ noticeably. Results were similar when overall survival was analysed.
Conclusions: This population based registry study shows that women treated with second generation antihistamines have a better overall and BC specific survival compared with non users regardless of age, history of allergy, ER status and tumor stage. The results are strongest for desloratadine use and use after BC diagnosis. Second generation antihistamines could offer a nontoxic therapy for both receptor positive and negative BC. The mechanism behind this effect is presently unknown.
https://ascopubs.org/doi/abs/10.1200/jco.2015.33.1...
DOI: 10.1200/jco.2015.33.15_suppl.3062 Journal of Clinical Oncology 33, no. 15_suppl (May 20, 2015) 3062-3062.
Published online January 31, 2017.
-
Report Back from ASCO on Metastatic Breast Cancer
Dr. Linda Vahdat, medical oncologist at Memorial Sloan Kettering Cancer Center and Chief of Medical Oncology and Clinical Director of Cancer Services at Norwalk Hospital, will summarize research presented at ASCO 2019 focusing on metastatic breast cancer. Dr. Vahdat will also discuss her current research in triple negative metastatic breast cancer.
@{@ 1 hour video/webinar presentation}
https://www.sharecancersupport.org/report-back-from-asco-on-metastatic-breast-cancer-3/
-
Great variety of articles Lumpie. Thank you
-
Lumpie, thanks for the info on Civica Rx. I hope it succeeds and provides drugs to individuals as well as hospitals!
-
Ultrasound breakthrough 'can spot cancer earlier'
A new ultrasound technique is being hailed as the biggest breakthrough in the technology for more than 60 years.
Developed at Heriot-Watt University in Edinburgh, it produces images that are 10 times better than current scans.
Researchers believe its ability to precisely pinpoint tumours could one day replace biopsies in investigating suspected cancer cases.
The method, which is about to begin trials in human patients, uses existing scanning equipment... The innovation has come in physics, statistics [,artificial intelligence] - and bubbles...
Dr Lu says it helps to think of each microbubble as a car in traffic. He used artificial intelligence to create a powerful algorithm that can track each one, and reveal the busiest routes...
If they go somewhere unexpected, it could be a sign of cancer - and one detectable much earlier than before.
These are super-resolution images showing details far beyond the physical limitations of the scanner...
Trials on human patients are expected to begin before the end of 2019 at the Western General Hospital in Edinburgh.
https://www.bbc.com/news/uk-scotland-edinburgh-east-fife-49870017
-
As Karen said, great variety of articles. Thanks for all the research you do. I save lots of these posts for future needs. I especially liked the one on antihistamine use being good for breast cancer. I have bad allergies and take lots of antihistamines. I've had MBC for almost four years now and I'm stable or NED after Ibrance for only 16 months and Letrozole alone since then. Wonder if the antihistamines are helping to keep the cancer in check.
Faith (in the future)
-
Interesting article about diet and its effect on breast cancer cells (as well as other cancer cells)
https://scienmag.com/dietary-vulnerability-found-i...
-
This provides interesting insights into post-neoadjuvant treatment pathology:
-
This reports a secondary analysis of the TAILORx trial that focused on outcomes for women with scores of 26-100, including a break down of results by chemo regimen.
As a reminder - none of this applies to node-positive cases.
https://www.medscape.com/viewarticle/919336?src=wnl_edit_tpal&uac=153476CT&impID=2117707&faf=1#vp_1
-
Risk Factors for Triple-Negative Breast Cancer among Latina Women
Laura Rey-Vargas, María Carolina Sanabria-Salas, Laura Fejerman and Silvia J. Serrano-GómezDOI: 10.1158/1055-9965.EPI-19-0035Abstract
Breast cancer is the most common cancer in Latina women. Although they have a lower incidence of the disease when compared with other population groups such as non-Hispanic white and African-American women, some studies have shown that Latina women have a higher risk of mortality when compared with non-Hispanic white women. This phenomenon can be explained in part by the higher prevalence of aggressive subtypes in Latina women, particularly the triple negative. Such differences in breast cancer–intrinsic subtype distribution between population groups might be a consequence of a variety of risk factors differentially present among population groups. Here, we provide a full description of risk factors that might be associated with the high prevalence of the triple-negative subtype in Latina women. We assessed demographic (socioeconomic status), modifiable (reproductive patterns, obesity, and physical activity), and nonmodifiable (family history, germline BRCA mutations, and genetic ancestry) risk factors. The observed inconsistencies among different epidemiologic studies in Latinas warrant further research focused on breast cancer subtype–specific risk factors in this population.
-
BevJen, to make your link live, all you have to do is hit return after the link.
-
Marjen,
Thanks. A techie I am not!
-
You’re welcome BevJen. I’ll say I used to be a techie, but now I only care about a few good years of quality life that I have left and keeping up techwise, well, I just don’t care too much anymore.
-
An essential approach in integrative healthcare involves the strategic combination of targeted modalities that work together to increase benefits of conventional therapies. This is particularly essential when addressing cellular health.
A 2017 preclinical study published in BMC Complementary and Alternative Medicine demonstrates that a breast health dietary supplement offers significant support in this area, specifically against the growth of aggressive breast cells.
Performed at the Methodist Research Institute, Indiana University Health, this study highlights the ability of the breast formula to boost the effects of tamoxifen—a hormonal protocol used for cellular breast health—against estrogen receptor-positive (ER-positive) breast cells. This is the fourth published study on this physician-formulated supplement, and the first using ER-positive cells, to demonstrate the vital breast health benefits of this unique formula.*
These outstanding results were also presented June 2019, at the ICCR-2019.Breastdefend Enhances Effect of Tamoxifen in Estrogen ReceptorPositive Human Breast Cancer in Vitro and in Vivo
-
- Patient Selection Key When De-Escalating Radiation in Breast Cancer
- Duke Cancer Institute Faculty Describe Latest Efforts in Breast Cancer Research
- Positive Abemaciclib Data Emerge for Chinese Women With HR+ Breast Cancer
- PD-L1 Assays Demonstrate <70% Concordance in Advanced TNBC
- Abemaciclib/Fulvestrant Improves Survival in HR+ Advanced Breast Cancer
-
Anti-evolution drug may help treat resistant breast cancers
Many cancer treatments work very well in the beginning only to fail later as tumours evolve resistance. But a new generation of therapies are being developed to prevent this.
One, called BOS172722, has been shown in animal studies to restore the effectiveness of paclitaxel, the main chemotherapy used to treat so-called triple-negative breast cancer...
[BOS172722] binds to and blocks a protein called MPS1 that plays a key role in division. The combination of the two drugs together causes such severe chromosomal abnormalities that none of the cancer cells survive. And if no cells survive, there can be no resistance.
There are some side effects, and the initial aim of the trial is to establish the maximum safe dose.
Also, Breast cancer drug trial raises hopes
The drug - known as BOS172722 - works by forcing cancer cells through cell division too quickly.
Spiros Linardopoulos, professor of cancer biology and therapeutics at the ICR, who led the study, said: "We have discovered a brand new type of cancer treatment that uses cancer's rapid growth against it, by forcing cells through cell division so quickly that they accumulate fatal errors...
According to the study published in the journal Molecular Cancer Therapeutics, cancer cells in dishes treated with the MPS1 inhibitor went through cell division in just 11 minutes, compared with 52 minutes without the drug.
And fast-dividing cells, from triple-negative breast cancers, ovarian and lung cancers, were especially sensitive to the effects of blocking MPS1.
Article: https://www.newscientist.com/article/2218935-anti-...
Study: https://mct.aacrjournals.org/content/18/10/1696.abstract
-
Earlier Diagnosis and Treatment Are Next Steps in TNBC Paradigm
There is an unprecedented array of therapeutic options for patients with triple-negative breast cancer, with more approaches on the horizon.
Immunotherapy for Breast Cancer: What's New and What's on the Horizon?
Immunotherapy may finally be taking center stage in breast cancer, although much work remains to be done.
Rugo Highlights Latest Advances in TNBC Treatment
Hope S. Rugo, MD, discusses the latest advancements and clinical trial data in triple-negative breast cancer treatment.
-
Short Courses of Antibiotics Can Cause Big Problems for Dental Patients
Unnecessary antibiotics linked with cases of C. diff, anaphylaxis
Some dental patients who were inappropriately given antibiotics prior to procedures suffered adverse events potentially connected to the drugs, such as anaphylaxis and Clostridioides difficile infection, researchers said here. Of patients inappropriately prescribed antibiotic prophylaxis prior to a dental procedure, almost 4% had adverse events ranging from new allergies and emergency department visits to anaphylaxis and C. difficile infection... Dentists prescribe 10% of antibiotics in the U.S., and are the largest specialty prescriber....o put that into perspective, she added, pediatricians and internists prescribe 10%-12% of all antibiotics in the U.S.
https://www.medpagetoday.com/meetingcoverage/idwee...
{Many of us face dental issues while being treated for b.c. so this article seemed uniquely relevant.}
-
Novel CDK 4/6 Inhibitor Fails in Triple Negative Breast Cancer
Misses primary endpoints but has unexpected key benefit
Attempting to limit adverse events with the investigational cyclin-dependent kinase (CDK) 4/6 inhibitor trilaciclib in triple-negative breast cancer failed to do what investigators theorized, missing both primary and secondary endpoints, researchers reported here. Nevertheless, treatment was still associated with improved overall survival relative to a standard chemotherapy regimen. Median overall survival was 12.6 months for women who were treated with gemcitabine plus carboplatin vs 20.1 months for those who had trilaciclib added twice during each 21-day treatment cycle with the chemotherapy doublet (P=0.0023), and 17.8 months for those who received trilaciclib four times per cycle... treatment was still associated with improved overall survival relative to a standard chemotherapy regimen.
"Patients who didn't receive trilaciclib were able to handle four cycles of chemotherapy, and those who received one of the two trilaciclib administration schedules were about to handle seven or eight cycles of gemcitabine-carboplatin, which translated to receiving 50% more chemotherapy in the trilaciclib arms. But there were no differences between the groups in side effects." ...that suggests some degree of bone marrow protection, because we were able to give more chemotherapy without having any statistically greater adverse events,"
"There is definitely interest in going ahead with a Phase III trial with gemcitabine and carboplatin plus or minus trilaciclib."
https://www.medpagetoday.com/meetingcoverage/esmo/...
-
MedPage Today's coverage from the 2019 European Society for Medical Oncology (ESMO) congress is a wrap -- check out the latest practice-informing news here.
https://www.medpagetoday.com/meetingcoverage/esmo
-
OIG Report: Ambulatory Surgery Center Inspections Lag
Report says states failed to inspect 147 facilities for 6 years, violating Medicare rules
Dozens of states, some of them very large, didn't meet Medicare's requirement that they survey their ambulatory surgery centers (ASCs) at required intervals to assure they met safety protocols, such as infection control or anesthesia administration, and many facilities went without any state survey for at least 6 years.
That's the finding of a recent report from the U.S. Department of Health and Human Services' Office of Inspector General (OIG). The agency took some states to task for not following two rules during fiscal years 2013-2017 -- made more imperative now that Medicare and commercial insurers reimburse ASCs for increasingly risky procedures.
https://www.medpagetoday.com/publichealthpolicy/he...
-
Design characteristics, risk of bias, and reporting of randomised controlled trials supporting approvals of cancer drugs by European Medicines Agency, 2014-16: cross sectional analysis
BMJ 2019; 366 doi: https://doi.org/10.1136/bmj.l5221 (Published 18 September 2019) Cite this as: BMJ 2019;366:l5221Objective To examine the design characteristics, risk of bias, and reporting adequacy of pivotal randomised controlled trials of cancer drugs approved by the European Medicines Agency (EMA).
Design Cross sectional analysis.
Setting European regulatory documents, clinical trial registry records, protocols, journal publications, and supplementary appendices.
Eligibility criteria Pivotal randomised controlled trials of new cancer drugs approved by the EMA between 2014 and 2016.
Main outcome measures Study design characteristics (randomisation, comparators, and endpoints); risk of bias using the revised Cochrane tool (bias arising from the randomisation process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result); and reporting adequacy (completeness and consistency of information in trial protocols, publications, supplementary appendices, clinical trial registry records, and regulatory documents).
Results Between 2014 and 2016, the EMA approved 32 new cancer drugs on the basis of 54 pivotal studies. Of these, 41 (76%) were randomised controlled trials and 13 (24%) were either non-randomised studies or single arm studies. 39/41 randomised controlled trials had available publications and were included in our study. Only 10 randomised controlled trials (26%) measured overall survival as either a primary or coprimary endpoint, with the remaining trials evaluating surrogate measures such as progression free survival and response rates. Overall, 19 randomised controlled trials (49%) were judged to be at high risk of bias for their primary outcome. Concerns about missing outcome data (n=10) and measurement of the outcome (n=7) were the most common domains leading to high risk of bias judgments. Fewer randomised controlled trials that evaluated overall survival as the primary endpoint were at high risk of bias than those that evaluated surrogate efficacy endpoints (2/10 (20%) v 16/29 (55%), respectively). When information available in regulatory documents and the scientific literature was considered separately, overall risk of bias judgments differed for eight randomised controlled trials (21%), which reflects reporting inadequacies in both sources of information. Regulators identified additional deficits beyond the domains captured in risk of bias assessments for 10 drugs (31%). These deficits included magnitude of clinical benefit, inappropriate comparators, and non-preferred study endpoints, which were not disclosed as limitations in scientific publications.
Conclusions Most pivotal studies forming the basis of EMA approval of new cancer drugs between 2014 and 2016 were randomised controlled trials. However, almost half of these were judged to be at high risk of bias based on their design, conduct, or analysis, some of which might be unavoidable because of the complexity of cancer trials. Regulatory documents and the scientific literature had gaps in their reporting. Journal publications did not acknowledge the key limitations of the available evidence identified in regulatory documents.
https://www.bmj.com/content/366/bmj.l5221
{entire article is available for review}
-
Why the Women Most Likely to Die of Breast Cancer Have Gotten the Least Attention
https://time.com/5689570/metastatic-breast-cancer-...
-
Thanks Marijen, good article
-
Hormone Therapy Has a Bigger Impact Than Chemotherapy on Women's Quality of Life [for early stage breast cancer]
Analysis of the CANTO cohort published in the journal Annals of Oncology will upset received wisdom on the effects that hormone therapy and chemotherapy have on the quality of life in women with breast cancer. Contrary to the commonly held view, 2 years after diagnosis, hormone therapy, a highly effective breast cancer treatment worsens quality of life to a greater extent and for a longer time, especially in menopausal patients. The deleterious effects of chemotherapy are more transient. Given that current international guidelines recommend the prescription of hormone therapy for 5 to 10 years, it is important to offer treatment to women who develop severe symptoms due to hormone antagonist medication and to identify those who might benefit from less prolonged or intensive treatment strategies.
-
debbew (and others,) I am ignorant on the issue of hormonal therapy, as I was diagnosed with triple negative cancer. Is there some either-or treatment for hormone positive treatments, like, you can do chemo OR you can do hormonal therapy? I'm thinking of the often used either-or of mastectomy OR lumpectomy with rads.
-
debbew, great post. I failed letrozole after 24 months. Makes me feel a little better about it.
Mountain Mia, hormonal therapy is usually an ‘addition to’ treatment. But it can be used alone without surgery, radiation or chemo.
Thanks Karen. Good luck to you, 11 years cancer free - congrats. How were your lung mets found?
-
MountainMia, as marijen noted, (anti)hormonal treatment is often offered for ER positive bc in conjunction with other possible treatments. I've read that about half of women prescribed hormonal treatment are non-compliant (and guessing the actual percentage is even higher, since I'm sure many women don't inform their doctors that they have stopped or reduced their dosage).
-
Course and predictors of post‐traumatic stress disorder in a cohort of psychologically distressed patients with cancer: A 4‐year follow‐up study
BACKGROUND
Scant evidence exists on the long‐term course of cancer‐related post‐traumatic stress disorder (PTSD). This is among the few studies worldwide, and the first in the South‐East Asian region, to prospectively evaluate PTSD in patients with cancer using gold‐standard clinical interviews. The objective of the study was to assess the course and predictors of PTSD in adult patients with cancer in a South‐East Asian population.
METHODS
A prospective, longitudinal study was conducted in a cohort of 469 consecutively recruited patients (aged ≥18 years) with various cancer types within 1 month of diagnosis at a single oncology referral center. Only patients who had significant psychological distress (Hospital Anxiety and Depression Scale total cutoff score ≥16) underwent the PTSD module of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (SCID) at at 6‐months follow‐up. All patients completed the SCID at the 4‐year follow‐up assessment regardless of their initial Hospital Anxiety and Depression Scale score.
RESULTS
In an analysis combining patients who had both full and subsyndromal PTSD, there was a 21.7% incidence of PTSD at the 6‐month follow‐up assessment (n = 44 of 203 SCID‐interviewed patients), with rates dropping to 6.1% at the 4‐year follow‐up assessment (n = 15 of 245 SCID‐interviewed patients). Patients with breast cancer (compared with those who had other types of cancer) were 3.68 times less likely to develop PTSD at 6‐months, but not at 4‐years follow‐up.
CONCLUSIONS
The overall rates of PTSD decreased with time, but one‐third of patients (34.1%) who were initially diagnosed had persistent or worsening PTSD 4 years later. There is a need for early identification of this subset of patients who have cancer with PTSD to design risk‐targeted interventions. Cancer 2018;124:406‐16. © 2017 American Cancer Society.
-
I found the following article very frustrating for its lack of details about the vaccine/studies; I believe they must be referring to the study in this announcement for a HER2/neu-targeted breast cancer vaccine, TPIV110.
New cancer vaccine shows promise, helped kill cancer cells in patient
A vaccine undergoing testing at the Mayo Clinic has reportedly removed cancer cells in a breast cancer patient. Florida resident Lee Mercker became the first patient to participate in a clinical trial for a new vaccine after being diagnosed in March with early-stages of the disease [DCIS].
Dr. Saranya Chumsri says the vaccine helps the body fight cancer cells.
"It's supposed to stimulate a patient's own immune response so that the immune cells like t-cells would go in and attack the cancer," Chumsri said.
For Mercker, it worked. She says it was just a 12-week process...
[Chumsri] says eventually, they hope it can be used to prevent cancer entirely.
Chumsri says they've made such incredible strides because of people who participate in the clinical trials. She says they've got trials for all stages of cancer, even having Stage 4 cancer patients showing positive results.
If you'd like to learn more about how to join a clinical trial at Mayo Clinic, call 1-855-776-0015.
Edited to add: Here's a more informative article:
-
Imaging tumor stiffness could help enhance treatment for breast and pancreatic cancer
Magnetic resonance elastography was able to visualise and measure how stiff and dense tumours are in mice. The technique, which can be implemented on conventional clinical MRI scanners, may help select the best treatment course for some cancer patients.
Scientists at The Institute of Cancer Research, London, found that using their new type of scan could assess the contribution of collagen to relative stiffness across a number of different tumour types.
This in turn could identify tumours in which there is the potential to use new drugs designed to 'weaken' the structure holding together tumours—thereby giving other drugs access to cancer cells in the centre of the tumour...
Initial studies established that collagen was key to keeping breast and pancreatic cancers stiff and inaccessible to treatments. In contrast, tumours arising from the nervous system, such as some forms of childhood cancer and brain tumours, were relatively soft and lacking in collagen.
The study, published in the journal Cancer Research today, was largely funded by the European Union, Cancer Research UK and the Rosetrees Trust...
the researchers found that the administration of collagenase resulted in a clear overall reduction in the elasticity and viscosity of breast tumours in mice—both of which fell by around a fifth.
The ICR researchers found that MR elastography provided extra details about tumour structure and density in addition to the information about growth and size given by standard MRI scans.
https://medicalxpress.com/news/2019-10-imaging-tumor-stiffness-treatment-breast.html
-
Jane McClelland posted this today on my Repurposed Drugs FB group:
The drug Repertaxin may be a way of targeting this rogue CXCR2 receptor in breast cancer. I was recently investigating this drug for prostate cancer. Here is some info on its use in combination with chemo for gastric cancer: https://www.ncbi.nlm.nih.gov/m/pubmed/26847910/
https://www.sciencedaily.com/releases/2019/10/191007123245.htm
-
Clinical Challenges: Brain Mets in HER2-Positive Breast Cancer
Multidisciplinary approach key as patients with brain metastases live longer
Over the last decade, there has also been a shift in the treatment of breast cancer with brain metastases, with clinicians now considering the use of systemic therapy in place of or in addition to local therapy, according to Jane Meisel, MD, of Winship Cancer Institute in Atlanta.
"In the past a lot of trials excluded these patients, but now more and more are including them, particularly patients with stable metastases after radiation," Meisel said. "Getting this type of real-world data, in this rapidly changing field, is more important than ever."
"... we ... see patients living 5 years or longer with brain metastases," Lin said.
-
This is not breaking but very informative.
Neuropathy in the Cancer Patient: Causes and Cures
Identifying the causes of neuropathy in cancer patients can be difficult. This review looks at the common causes of neuropathy in cancer patients, as well as effective therapies—and even preventions.
-
Breast Cancer Brain Metastases: New Initial Therapy Options
September 17, 2019
https://www.medscape.com/viewarticle/917894?src=mk...
-
'How Long Do I Have?' Tackling Oncology's Most Difficult Question
It's a question that cuts to the heart of patients' concerns.
Even with the help of big data and online prognostic tools, immunotherapies and targeted treatments have made this question very difficult to answer. This is where prognosticating becomes more of an art than a science, and one that requires a careful, step-by-step approach based on clinical experience and intuition.
-
Concordance of Genomic Variants in Matched Primary Breast Cancer, Metastatic Tumor, and Circulating Tumor DNA
The MIRROR Study
Purpose: Genetic heterogeneity between primary tumors and their metastatic lesions has been documented in several breast cancer studies. However, the selection of therapy for patients with metastatic breast cancer and the search for biomarkers for targeted therapy are often based on findings from the primary tumor, mainly because of the difficulty of distant metastasis core biopsies. New methods for monitoring genomic changes in metastatic breast cancer are needed (ie, circulating tumor DNA [ctDNA] genomic analysis). The objectives of this study were to assess the concordance of genomic variants between primary and metastatic tumor tissues and the sensitivity of plasma ctDNA analysis to identify variants detected in tumor biopsies.
Patients and Methods: Next-generation sequencing technology was used to assess the genomic mutation profile of a panel of 54 cancer genes in matched samples of primary tumor, metastatic tumor, and plasma from 40 patients with metastatic breast cancer.
Results: Using Ion Torrent technology (ThermoFisher Scientific, Waltham, MA), we identified 110 variants that were common to the primary and metastatic tumors. ctDNA analysis had a sensitivity of 0.972 in detecting variants present in both primary and metastatic tissues. In addition, we identified 13 variants in metastatic tissue and ctDNA not present in primary tumor.
Conclusion: We identified genomic variants present in metastatic biopsies and plasma ctDNA that were not present in the primary tumor. Deep sequencing of plasma ctDNA detected most DNA variants previously identified in matched primary and metastatic tissues. ctDNA might aid in therapy selection and in the search for biomarkers for drug development in metastatic breast cancer.
August 15, 2019
https://www.medscape.com/viewarticle/916337?src=mk...
JCO Precis Oncol. 2019;2019(3)
-
On-treatment Biomarkers Can Improve Prediction of Response to Neoadjuvant Chemotherapy in Breast Cancer
Breast Cancer Research August 09, 2019
Background: Neoadjuvant chemotherapy is increasingly given preoperatively to shrink breast tumours prior to surgery. This approach also provides the opportunity to study the molecular changes associated with treatment and evaluate whether on-treatment sequential samples can improve response and outcome predictions over diagnostic or excision samples alone.
Conclusion: Changes in gene expression measured in sequential samples from breast cancer patients receiving neoadjuvant chemotherapy resulted in the identification of a potentially novel on-treatment biomarker and suggest that established prognostic tests may have greater prediction accuracy on than before treatment. These results support the potential use and further evaluation of on-treatment testing in breast cancer to improve the accuracy of tumour response prediction.
https://www.medscape.com/viewarticle/915855?src=mk...
Breast Cancer Res. 2019;21(73)
-
Sunday Is Metastatic Breast Cancer Awareness Day
October 13, 20198:00 AM ET
Heard on NPR's Weekend Edition Sunday
NPR's Lulu Garcia Navarro talks to Dr. Filipa Lynce, a medical oncologist, and Julia Maues, a woman living with metastatic breast cancer, about what more can be done to fight the deadly disease.
{Quick listen: 6:45 in length}
https://www.npr.org/2019/10/13/769848661/sunday-is...
-
MacroGenics looks to future with breast cancer drug margetuximab
June 3, 2019
A small biotech, MacroGenics, took the market by surprise earlier this year with some surprising data from its margetuximab – essentially a tweaked version of Roche's Herceptin (trastuzumab) where a few amino acid mutations are enough to produce a stronger cellular response to cancer.
-
New Cancer Vaccine Shows Shows Early Promise In Human Clinical Trials
Doctors say a new vaccine undergoing clinical trials at the Mayo Clinic has effectively removed cancer cells, providing new hope for cancer survivors.
-
'Unacceptable' delays in diagnosing secondary {metastatic} breast cancer
One in four patients with secondary {metastatic} breast cancer had to visit their GP three or more times before they got a diagnosis, a survey suggests.
A breast cancer charity said there should be more awareness that the disease can spread to other parts of the body.
Breast Cancer Now said it was "unacceptable" that some people whose cancer had spread were not getting early access to treatments which could alleviate symptoms and improve their quality of life.
https://www.bbc.com/news/health-49999404?ocid=soci...
{Kudos to Breast Cancer Now for this advocacy work!}
-
Multigene Testing for All Patients With Breast Cancer Is Cost-Effective
- JAMA Oncology Published online October 3, 2019. The authors of this cost-effectiveness microsimulation modeling study estimated the incremental lifetime effects, costs, and cost-effectiveness of multigene testing for all patients with breast cancer. The authors found unselected, high-risk multigene testing to be cost-effective compared with testing based on family history or clinical criteria for both the UK and US healthcare systems. This study provides evidence to support the expansion of genetic testing to all women with breast cancer.https://www.practiceupdate.com/C/90665/56?elsca1=e...https://jamanetwork.com/journals/jamaoncology/full...doi:10.1001/jamaoncol.2019.3323
-
Unraveling the Mystery of What Gives Exceptional Responders Their Superpower
A Conversation With Isaac S. Kohane, MD, PhD
{About a year old but an interesting discussion about Exceptional Responders.}
https://www.ascopost.com/issues/august-25-2018/unr...
-
Following NCCN Guidelines for Metastatic Breast Cancer Results in Lower Costs for Patients, According to New Study
Guideline Discordance and Patient Cost Responsibility in Medicare Beneficiaries With Metastatic Breast Cancer
A new study from the O'Neal Comprehensive Cancer Center at University of Alabama at Birmingham (UAB), published in the October 2019 issue of JNCCN—Journal of the National Comprehensive Cancer Network, finds that direct costs for metastatic breast cancer (MBC) patients increase dramatically when their treatment differs from recommendations in the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Previous studies have found that guideline discordant care results in higher health care costs overall[1], but this is the first study to look specifically at the cost burden for patients.
-
Talking about Toxicity — "What We've Got Here Is a Failure to Communicate"
Improving communication with patients about treatment risks and benefits has long been recognized as a critical priority. But perhaps a necessary first step is for investigators to communicate with clinicians openly and specifically about the toxic effects of treatment.October 10, 2019
N Engl J Med 2019; 381:1406-1408
DOI: 10.1056/NEJMp1908310https://www.nejm.org/doi/full/10.1056/NEJMp1908310...
{NEJM allows access to two articles per month without subscription.} -
I'm sorry: Why I lost my love for medicine
Anonymous | Physician | July 31, 2019
{A physician reflects on his/her disillusion with the practice of medicine and commitment to redeem a sane existence in the wake of a broken system. Link provided by a physician friend.}
https://www.kevinmd.com/blog/2019/07/im-sorry-why-...
-
Lumpie, I registered and read the Talking about Toxicity — "What We've Got Here Is a Failure to Communicate" article. Thank you so much for sharing that one. Very, very helpful.
-
Current Breast Cancer Statistics
- CA: A Cancer Journal for Clinicians The authors used large, national databases to provide updated data on incidence, mortality, survival, and screening among female breast cancer patients in the US. Despite a small increase in the breast cancer incidence rate over the past 5 years, mortality from breast cancer continues to decline. There remains a black–white disparity in breast cancer mortality, with the highest death rate seen in black women aged <50 years. In 6 states, breast cancer is now the leading cause of death in black women. Access to high-quality prevention, early detection, and treatment should be improved to optimize outcomes in this population.
-
Recorded webinar, Brain Metastasis: Emerging Treatments and Reasons to be Hopeful, is now available for viewing.
Join Dr. Nancy Lin, Director of the Metastatic Breast Cancer Program at Dana-Farber Cancer Institute, as she discusses diagnosis, symptom management, emerging treatments and reasons to be hopeful with Julia Maues, a metastatic breast cancer patient advocate. This program is in collaboration with Living Beyond Breast Cancer and Young Survival Coalition.
@ 1 hour in length
https://www.sharecancersupport.org/brain-metastasi...
Presented by sharecancersupport.org
-
HER2-Positive Breast Cancer
Lead KATE2 Author Suggests Atezolizumab Benefits HER2+ Breast Cancer Subgroup
Adding atezolizumab may improve outcomes in HER2+ breast cancer with PD-L1 expression.
Safety Analysis Supports Adjuvant T-DM1 Use in Early HER2+ Breast Cancer
Michael Untch, MD, PhD, discusses a secondary analysis of safety results from the phase III KATHERINE trial.
FDA Updates Neratinib Label in HER2+ Breast Cancer
Review the new safety data included in neratinib's labeling supplement.
Fixed-Dose Subcutaneous Pertuzumab Combo Shows Noninferiority in HER2+ Breast Cancer
The fixed-dose subcutaneous injection formulation plus intravenous chemotherapy had noninferior pharmacokinetics versus standard IV infusions of the regimen in patients with HER2-positive early disease.
-
New treatment combination could work against broader array of cancer cells, study finds [but no trials for bc with this combo yet]
In a proof of concept study, the researchers demonstrated that combining a PARP inhibitor with a DNA methyltransferase (DNMT) inhibitor delivered a one-two punch to non-small cell lung cancer tumors, which are normally not associated with mutations in BRCA genes. The research, conducted in mouse models and cell lines, outlines the mechanistic action of the combination. The DNMT inhibitor triggers an effect that mimics a BRCA mutation in the cancer cell so the cell responds to the lethal effects of the PARP inhibitor, which prevents repair of damage to a tumor cell's DNA, triggering cell death.
"When combined, these agents cause interactions that significantly disrupt cancer cells' ability to survive DNA damage," said study senior author, Feyruz V. Rassool, PhD, professor of radiation oncology at UMSOM. "Our findings could expand the use of PARP inhibitors beyond the minority of inherited cancers that it now treats."
..."Finding a new paradigm to attack cancer cells is very exciting, especially when researchers can make use of drugs that are already on the market and have been well tested for efficacy and toxicity," said E. Albert Reece, MD, PhD, MBA, Executive Vice President for Medical Affairs, UM Baltimore, and the John Z. and Akiko K. Bowers Distinguished Professor and Dean, University of Maryland School of Medicine. "
https://www.eurekalert.org/pub_releases/2019-10/uoms-ntc101319.php
-
Is it possible to prevent breast cancer metastasis?
Study reveals how blood vessels in the bone marrow protect dormant tumor cells, suggests a way to kill them in their sleepJanuary 21, 2019
Researchers at Fred Hutchinson Cancer Research Center in Seattle may have found a way to essentially smother cancer cells in their sleep, preventing them from ever waking up and forming deadly metastatic tumors.
It's always been assumed that dormant cells cannot be killed by any kind of chemotherapy because they're not dividing," said Ghajar, who runs the Laboratory for the Study of Metastatic Microenvironments at Fred Hutch. "But what we're showing is that's not true. They're relying on survival signaling in their microenvironment, in this case specifically from blood vessels within the bone marrow. And if you can take away that signaling, you can sensitize them to chemotherapy."
...a clinical trial could be three to five years away....
https://www.fredhutch.org/en/news/center-news/2019...
-
Sounds like the title of a horror movie “Kill Them in Their Sleep”. That’s awesome!
-
Yes! That's a happy thought isn't it!
") Just the sort of thing you'd want to do to cancer!
Just the sort of thing you'd want to do to cancer! -
When Breast Cancer Hides in Plain Sight with Lynda Weatherby Real Pink
This week on Real Pink we are hosting daily conversations about breast cancer that hides in the shadows: metastatic breast cancer (MBC).
In the US alone, MBC is expected to kill 42,000 people. This special episode, featuring Lynda Weatherby, is part of National Breast Cancer Awareness Month.
Special Guest: Lynda Weatherby.
Sponsored By: Susan G. Komen - MBC Week: Susan G. Komen is proud to launch the "MBC Fund" specifically designed to spur scientific discoveries and support those women and men living with Metastatic Breast Cancer, building on Komen's $210 million investment in metastatic breast cancer research. For more information on the MBC Fund and how to support it, visit www.komen.org/MBC.https://podcasts.apple.com/us/podcast/real-pink/id...
{Podcast re MBC.}
-
Men account for a small fraction of breast cancer cases. Their fatality rate has soared compared with women's
-
Watch: In a quest for more precise cancer care, hospitals invest in new tools — and new training, too
https://www.statnews.com/2019/09/30/precise-cancer...
-
A small biotech raises the price on its cancer drug by 20% this year, but will anyone notice?
https://www.statnews.com/pharmalot/2019/10/09/puma-biotech-drug-prices-cancer/
-
This Free Tool for Doctors Can Cut 5 Years Off Breast Cancer Hormone Therapy
Experts say the online algorithm can accurately predict the risk of reoccurrence of breast cancer and cut post-treatment therapy from 10 to 5 years.
the new algorithm, called CTS5, could cut hormone therapy in half, from 10 years to 5, for certain patients.
Researchers from The Royal Marsden National Health Service (NHS) Foundation Trust and Queen Mary University of London presented their findings {in June 2019}.
Experts told Healthline that CTS5 is a simple, effective tool that can help some patients avoid years of unnecessary therapy.
https://www.healthline.com/health-news/clinical-ca...
https://www.qmul.ac.uk/media/news/2019/smd/clinica...
https://www.cts5-calculator.com/
{Additional links to sources in article.}
-
ESMO Breast Cancer Roundtable: Episode 1
What role does genomic testing play in HR+ breast cancer?
At the recent ESMO Congress 2019 in Barcelona, Hope Rugo, MD, Jennifer Litton, MD, and Michelle Melisko, MD, gathered to discuss new and some potentially practice-changing data from the meeting on advanced hormone receptor-positive breast cancer.
In the first of five exclusive MedPage Today episodes, the discussion centers on use and interpretation of how to approach genomic testing for the management of patients, and how the results can inform treatment decisions and improve patient management.
https://www.medpagetoday.com/meetingcoverage/esmoe...
{Transcript and video}
-
FDA Grants Trastuzumab Deruxtecan Priority Review for HER2+ Breast Cancer
Review the data supporting the application for this antibody-drug conjugate.
-
Blocking tumor evolution to halt cancer drug resistance
[R]esearchers at Massey University and the Maurice Wilkins Centre for Molecular Biodiscovery in New Zealand are developing a new class of drug that could put the brakes on these evolutionary processes by targeting a less-essential immune system enzyme that triggers some of the initial mutations of tumor DNA...
APOBEC-3B has been identified as major source of genetic mutations in multiple breast, bladder, cervical, lung, ovarian and head and neck cancers, according to co-corresponding author Vyacheslav Filichev, a professor at Massey University...
The study, published in the journal Organic & Biomolecular Chemistry, details the work of Filichev's team in synthesizing short oligonucleotides toward a treatment that targets specific APOBEC3 enzymes.
Following these first steps, Filichev estimates that it may take five to 10 years before a potential therapy reaches clinical trials.
https://www.fiercebiotech.com/research/blocking-tumor-evolution-to-halt-cancer-drug-resistance
-
Left-right difference in breast cancer inspires new research, Ann Ramsdell, TEDxColumbiaSC
{Interesting presentation from 2015 re left-right breast tumor laterality.}
Related articles:
Mammary glands exhibit molecular laterality and undergo left-right asymmetric ductal epithelial growth in MMTV-cNeu mice
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4261057/
doi: 10.1038/onc.2014.149
Asymmetric Cancer Hallmarks in Breast Tumors on Different Sides of the Body
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0157416
https://doi.org/10.1371/journal.pone.0157416
Left–right analysis of mammary gland development in retinoid X receptor-α+/− mice
https://royalsocietypublishing.org/doi/full/10.1098/rstb.2015.0416
https://doi.org/10.1098/rstb.2015.0416
-
Lumpie - one of the best things I've watched in a long time. Thanks for posting.
-
Agree--Lumpie this was fascinating reading. . . .thank you for posting.
-
Thanks for the feedback. I will watch for more of these. If you have a moment, let me know what features/aspects you liked. multi-media (video), "accessible" research, etc. I got a link to a podcast about pollutants and BC risk. May not be everyone's cup of tea but some may find it interesting. I haven't listened to it yet but can post the link for those interested.
-
Podcast: Breast Cancer Action's Executive Director Karuna Jaggar interviewed Sharon Lerner, an award-winning investigative journalist who's written a powerful and groundbreaking series on toxic PFAS.
Blurb says "Learn about these toxic chemicals used in every day products, first developed by corporate giant 3M seventy years ago. And find out what Lerner uncovered about how 3M has tried to conceal the serious health risks of PFAS while continuing to develop new chemicals in the class. Take a deeper dive into our 2019 Think Before You Pink Campaign, Say Never to Forever Chemicals. Find out why we're calling on 3M to stop pinkwashing and how you can make a difference."
Brief background on Breast Cancer Action: an activist watchdog organization. BCAction, is focused on systemic interventions that will address the root causes of the disease and produce broad public health benefits. These benefits will ensure that fewer women develop breast cancer and die from breast cancer and no community bears a disproportionate burden of diagnosis or death from this disease. Mission: Breast Cancer Action's mission is to achieve health justice for all women at risk of and living with breast cancer.
{BCA has an environmental focus in much of their work.}
Find the podcast here:
https://bcaction.org/2019/10/17/3ms-post-its-peel-...
-
Yes - that was very interesting. Thanks for all your research.
-
Lumpie - absolutely everything you post will be of interest & importance to different ones. It's just so neat that you take the time to do all this research. And best of all, you do a summary in case we don't understand the reports in the links. (who am I kidding, most of us don't)
Personally I'm interested in HER2+ and bone health - but as I said, everything you post is relevant. Edited to add - lymphadema and neuropathy.
Thanks again.
-
Some of you may enjoy seeing this interview with Kelli Davis, co-founder of the Northwest Arkansas Metsquerade Gala which raises funds for metastatic breast cancer research. Just to the 20 minute mark to see the interview. This interview is about 8 minutes long. {Kudos to Kelli and others in NW Ark who have raised hundreds of thousands of dollars for MBC research. They are an inspiration.}
-
Genetic Testing Vs. Genomic Testing - Differences and Benefits
{Basic discussion about genetic and genomic testing and the differences. Targeted to a lay (non-healthcare professional) audience.}
https://www.whatnext.com/blog/posts/genetic-testin...
"Developed in part with the American Cancer Society, WhatNext uses patent pending matching algorithms to connect people to highly relevant peers, firsthand experiences and American Cancer Society resources."
-
Lumpie, just wanted to express my appreciation for this site and all that you do to keep us informed. You and the others who post here have made it possible for me to be an educated participant in my journey instead of a person being acted upon by disease. THANK YOU!
-
New organelle discovered inside cells found to prevent cancer
Scientists at the University of Virginia School of Medicine have discovered a strange new organelle inside our cells that helps to prevent cancer by ensuring that genetic material is sorted correctly as cells divide.
The researchers have connected problems with the organelle (a subcellular structure) to a subset of breast cancer tumors that make lots of mistakes when segregating chromosomes. Excitingly, they found their analysis offered a new way for doctors to sort patient tumors as they choose therapies. They hope these insights will allow doctors to better personalize treatments to best benefit patients—sparing up to 40% of breast cancer patients, for example, a taxing treatment that won't be effective...
The organelle Stukenberg and his team have discovered is essential, but ephemeral. It forms only when needed to ensure chromosomes are sorted correctly and disappears when its work is done. That's one reason scientists haven't discovered it before now...
Stukenberg and his colleagues described their latest findings in the scientific journal Nature Cell Biology.
https://phys.org/news/2019-10-organelle-cells-cancer.html
-
Women with... triple-negative [bc]... could be differentiated from each other by a panel of 17 small RNA molecules that are directly influenced by genetic alterations typically found in cancer cells.
Researchers lead by Luciane Cavalli, PhD, at Georgetown Lombardi Comprehensive Cancer Center, and colleagues found that variations in how these small RNA, known as microRNA (miRNA), are expressed, at higher or lower levels, could partially explain disparate rates of triple-negative breast cancer (TNBC) in Latina women compared to non-Hispanic white women and potentially lead to more effective treatment options.
That is the finding of a new study that was published October 22, 2019, in Oncotarget...
The scientists discovered that women with TNBC had specific alterations in copies of their genes that directly influenced the expression of 17 miRNAs compared to women with other forms of breast cancer who did not have these alterations. They also found that the expression levels of the majority of these miRNAs were associated with the tumor's clinical aggressiveness (advanced grade and stage).
"The panel of miRNAs we identified indicate potential, critical cancer-related pathways and gene networks that could be targeted for the treatment of TNBC in Latinas, once our findings are validated by larger studies," concluded Cavalli. "Targeting these genetic alterations, that represent the unique biology of their tumors, may lead to more efficient treatments, which could increase the longevity of Latina women who do not have many therapeutic options to fight this very aggressive disease."
https://www.sciencedaily.com/releases/2019/10/191022080728.htm
-
"Breast cancer detected by thermal imaging scan in Edinburgh"
https://www.bbc.com/news/uk-scotland-edinburgh-east-fife-50139540
-
Scientists unveil the secret of cancer-associated Warburg effect
The new study, published in the October 23 issue of Nature, shows that lactate, an end product of metabolism [and the Warbyrg effect], changes the function of an immune cell known as a macrophage, thereby rewiring it to behave differently...
Using bacterially-exposed macrophages as a model system, the researchers found that histone lactylation alters the [macrophages] from a pro-inflammatory and anti-bacterial state (known as M1) to an anti-inflammatory and reparative state (known as M2).
In response to bacterial infection, macrophages must react rapidly with a substantial pro-inflammatory burst to help kill bacteria and recruit additional immune cells to the infection site. During this process, macrophages switch to aerobic glycolysis, which is thought to support generation of pro-inflammatory immune substances called cytokines. However, the researchers show that over time, this metabolic switch also increases lactate, which stimulates histone lactylation to express stabilizing genes that may repair collateral damage to the host incurred during infection.
Although this reparative M2 macrophage phenotype may help control damage during infection, its presence in tumors is known to promote growth, metastasis and immune suppression in cancer...
More research is needed on the role and regulation of this new histone modification, but the discovery draws an exciting link between cellular metabolism and gene regulation that was previously unknown and could have promising implications for human health.
https://www.sciencedaily.com/releases/2019/10/191023132238.htm
-
Stressing cancer with spice [not bc-specific]
The team of Professor Jun-ya Kato, at Nara Institute of Science and Technology (NAIST), had previously identified that curcumin acts on the same reactive oxygen species enzymes as its analogue, PGV-1. By suppressing the enzyme activity, reactive oxygen species are allowed to cause stress on cells, ultimately leading to cell death. Indeed, many anti-cancer drugs operate similarly, but sometimes with severe side-effects due to stress on healthy cells.
In the new study, Kato's team compared the effects of curcumin and PGV-1 on cancer, finding that they shared many of the same properties, but that PGV-1 did so at higher efficiency and lower dose...
Intriguingly, PGV-1 was effective on numerous types of cancers. Moreover, when administered to mice injected with human cancer cells, the mice showed no evidence of the cancer and no side-effects. Furthermore, unlike some other anti-cancer drugs, the anti-cancer effects persisted even after the cessation of PGV-1 administration...
"Considering the high drug efficacy and low amount of side effects in animals, we propose that PGV-1 should be pharmaceutically developed as an orally administered drug for cancer," [Kato] says.
https://www.sciencedaily.com/releases/2019/10/191023104613.htm
-
Mapping cancer's drug resistance could improve treatment [not bc-specific]
The [laboratory and computational] techniques – developed [by Weill Cornell Medicine] with researchers from the New York Genome Center (NYGC) and the Broad Institute of the Massachusetts Institute of Technology and Harvard University – will allow researchers in principle to anticipate resistance mechanisms and suggest optimal drug doses and combinations across cancer types....
Combining two or more treatments that work in different ways is one promising approach, but for most cancers it is impractical to test in clinical trials the many combinations that are now possible.
Landau and his colleagues developed their new technique to reveal likely resistance pathways and optimal drug regimens in advance, with relatively inexpensive and comprehensive laboratory testing. That could allow subsequent tests, including clinical tests, to focus on more promising treatment combinations.
The scientists demonstrated their approach using lung cancer cells whose malignant growth is driven by the overactivity of a growth-factor receptor called EGFR... The results indicated that resistance can arise to these drugs and combinations from dozens of different genes involving multiple pathways... One of the most striking and important findings was that resistance to a combination of two drugs can arise more or less out of the blue – from genes that confer no resistance to either drug alone. The results suggest that the effects of two drugs in combination may be impossible to predict completely from their effects when used singly...
The researchers did, however, develop a framework for using genotype fitness mapping to identify promising drug doses and combinations. They concluded that for many EGFR-driven lung cancers, combining an EGFR inhibitor and an MEK inhibitor is seemingly optimal, though single-drug therapy with an MEK inhibitor might be better if certain other mutations are also present – and for many patients alternating combination therapy with MEK-inhibitor monotherapy might work best.
http://news.cornell.edu/stories/2019/10/mapping-cancers-drug-resistance-could-improve-treatment
-
FDA Calls for Boxed Warning on All Breast Implants
Agency seeks to boost genuinely informed patient consent
The FDA issued a draft guidance recommending that manufacturers of breast implants include a boxed warning that clearly spells out the risks of their products. The agency also called on implant-makers to include a patient decision checklist and list the devices' ingredients, and updated its own recommendations for implant rupture screening.
https://www.medpagetoday.com/washington-watch/fdag...
-
Special garments ease an agonizing ailment for women. But insurance may not pay.
Many lymphedema patients struggle to get health insurers to pay for compression garments. Coverage varies among private insurance plans, and for many patients it is limited. Although Medicaid programs cover some of these expenses, Medicare does not.
https://www.washingtonpost.com/health/special-garm...
https://www.congress.gov/bill/116th-congress/house...
https://www.congress.gov/bill/116th-congress/senat...
{Evidently no movement on these bills this Congress.
 }
} -
Anesthesia Technique Flops in Large Breast Cancer Trial
No effect on recurrence or pain with regional method, opioid avoidance
regional anesthesia-analgesia with paravertebral blocks and propofol during breast cancer surgery did not lower the risk of disease recurrence or incidence of persistent pain compared with general anesthesia with sevoflurane and opioids, a randomized trial found.
https://www.medpagetoday.com/hematologyoncology/br...
-
ESMO Breast Cancer Roundtable: Episode 2
CDK4/6 inhibitors improve overall survival in advanced breast cancer
@{Video and transcript available. @ 10 minutes in length.}
https://www.medpagetoday.com/meetingcoverage/esmoe...
-
Women with interval breast cancer -- detected between two routine screening mammograms -- have an increased risk of developing other types of cancer.
Breast cancer detected between two routine screenings is called interval cancer, and it tends to be more advanced, more aggressive and to have a worse prognosis than cancers found during screenings.
https://www.usnews.com/news/health-news/articles/2...
-
Health-care system causing rampant burnout among doctors, nurses
As many as half of all clinicians suffer from the problem, creating risks to patients, malpractice claims and absenteeism, study finds.
Imagine a health-care system in which doctors and nurses are so exhausted and beaten down that many of them work like zombies — error-prone, apathetic toward patients and at times trying to blunt their own pain with alcohol or even suicide attempts.
That is what America's broken health care system is doing to its health workers, according to a 312-page report released Wednesday by the National Academy of Medicine, one of the country's most prestigious medical institutions.
"It's incredibly inefficient, and the workload is unsustainable," said Liselotte Dyrbye, a doctor and researcher at the Mayo Clinic. "The system is built for billing and not taking care of patients."
Wednesday's report outlined a hefty list of needed changes...
https://www.washingtonpost.com/health/2019/10/23/b...
-
Seattle Genetics Announces Positive Topline Results from Pivotal Trial of Tucatinib in Locally Advanced or Metastatic HER2-Positive Breast Cancer
10/21/2019
-HER2CLIMB Trial Met Primary Endpoint and Both Key Secondary Endpoints-
-Global Regulatory Strategy Includes NDA Submission to U.S. FDA Planned for First Quarter of 2020-
-Data to be Presented at the 2019 San Antonio Breast Cancer Symposium-
https://investor.seattlegenetics.com/press-release...
{Seattle Genetics Press Release}
-
Seattle Genetics Announces Initiation of Phase 3 Clinical Trial of Tucatinib in Combination with Ado-trastuzumab Emtansine (T-DM1, Kadcyla®) for Patients with Advanced or Metastatic HER2-Positive Breast Cancer
10/10/2019
https://investor.seattlegenetics.com/press-release...
{Seattle Genetics Press Release}
-
Thanks Lumpie. Good info for us HER2+ people.
-
My pleasure, MinusTwo!
-
Blame rising cancer overdiagnosis on 'irrational exuberance' for early detection
Here's some good news for a change about cancer: Cancer mortality — the rate of death from cancer — has fallen substantially over the last four decades. There is also, however, some not-so-good news: Cancer incidence — the rate of cancer diagnoses — has been rising. This doesn't reflect increasing dangers in our environment, but a danger in our medical system. Even though overall mortality from cancer is falling, the overall incidence is rising.... overdiagnosis — the diagnosis of cancers not destined to cause symptoms or death. This exuberance began with the observation that patients in whom cancer was detected early lived years longer than those in whom cancer was detected later. The simple inference was that they had benefited from early detection. Many doctors recognized the logical fallacy here, one that has nothing to do with overdiagnosis: If we start the clock earlier in the course of disease, patients will always appear to live longer — even if their time of death is unchanged. These are not epidemics of disease. They are epidemics of diagnosis. Paradoxically, overdiagnosis helps fuel the exuberance for early detection. Survival rates skyrocket either because the clock started ticking earlier or the disease was not destined to cause death. More people appear to be cured. And more survivors — as well as more politicians — advocate for more early detection. Overdiagnosis isn't the only danger caused by early detection. False alarms are another... Early detection is great for the business of medicine.
https://www.statnews.com/2019/10/02/overdiagnosis-...
https://www.nejm.org/doi/full/10.1056/NEJMsr190544...
{The author cautions that early detection in not a panacea. NEJM allows access to a limited number of articles each month for non-subscribers.}
-
How Much Money Has Your Doctor Received From Drug Companies?
Use ProPublica's Dollars for Docs database to find out.
article:
https://www.propublica.org/article/dollars-for-doc...
search database:
https://projects.propublica.org/docdollars/
-
Researchers uncover dangers of ringing a bell to celebrate 'victory' over cancer
Williams, who led the study while completing his residency in radiation oncology at the Keck School of Medicine of USC, expected the bell to have a positive impact on patients. After all, they rang it in celebration. Instead, people who rang the bell viewed their overall treatment as more distressing than those who didn't...
When he surveyed the patients again after three months, the effect had worsened. Williams speculates that ringing the bell locks in painful memories of treatment through a phenomenon called emotional arousal...
Now Williams, who works in a cancer treatment center in Santa Maria, Calif., encourages his patients — especially those who went through a prolonged and painful treatment regimen — to consider subtle and calm ways to celebrate.
https://news.usc.edu/161762/victory-bell-cancer-treatment-usc-research/
-
Lymphedema Bill of Rights - there is legislation to add lymphedema treatment to Medicare. It has not gotten out of committee. This site describes lymhedema, who in congress is on board/who is not, and has links to your representatives, as well as boiler plate statements to include in letters. If Congress keeps getting these, maybe they will start listening. Maybe tie it to voting for a candidate. I wrote a letter, response from my representatives was rather pathetic. https://www.stepup-speakout.org/
Exercise very regularly, if not at the gym, then walk/hike, weights, stretch, swim, x-country ski etc.
Supplements: GAIA turmeric-joint; glucosamine-chondroitin; magnesium glycinate; biotin; potassium-iodine; C; B-complex ; D; Fish oil (but not now). For a year or so after bi-lateral used Juven Nutritional therapy for wound healing with 7g arginine, 7g glutamine for about a year. Often add turmeric to meals. Ran out of fish oil supplement that I liked, other brand caused fish burps, so have not taken for a while
2009 ER+ left breast. 52 yrs. Lumpectomy, Sentinel node removal, negative. Radiation 6 weeks, tamoxifen 5 years. Dense lumpy left breast, normal right. Acupuncture offered at facility as part of integrative medicine. It really helped with anxiety/stress during radiation treatment.
2016 ER+ left breast. Probably a new cancer, but unknown. 4 rounds TC Aug-Oct 2016, Bi-lateral (my choice) Nov 2016, no reconstruction. 2 sentinel nodes remove, negative. Cold Capping using Chemo Cold Caps (DIGNICAP not available). Anastrozole 1 mg starting May 2017. Joint issues noticed immediately. Stopped Anastrozole after 3-4 months due to joint stiffness in. After several months of no AIs, fingers were feeling better. Started tamoxifen March 2018
10/2018 noticed stiffness and some trigger finger again. Was eating meat a lot more (daily) than normal. Usually 1-2 /wk. Have cut way back on the meat, seems to help, but one finger still very prone to trigger finger. Trigger finger seemed to be getting better, but now 4/2019 seems worse, is it the break from added turmeric to meals?
7/19/2019 - swelling in R-arm, opposite side from where lymph nodes removed. Noticed 6/18/2019. Could have been swelling earlier but wearing long sleeves. Trip to urgent care. They did ultrasound, concerned that there might be a clot, there was not. Started seeing lymphatic therapist 7/2/2019.
8/2019 CT, Breast/chest , neck/thyroid ultra sound
9/2019 DR ordered biopsy, said it could be lymphoma, cancer, benign lymphatic. Biopsy R-axilla. Cancer. Genetic test showed no known markers (20+ looked for)
9/29/2019 PET scan, no indication of spread. Arimadex and Ibrance prescribed to shrink tumor prior to surgery
-
They turn to Facebook and YouTube to find a cure for cancer — and get sucked into a world of bogus medicine
Mari pressed kale leaves through the juicer, preparing the smoothie that she believed had saved her life. The video, first uploaded in 2016, remains on YouTube, but there's an "important update" attached to the video's description. It was written by Liz, her niece, a year later. Mari's cancer had returned, the note said, and she had died.
...the web of false, misleading and potentially dangerous cancer "cures" and conspiracy theories isn't just there for those who stumble into it accidentally. More often it ensnares people who are reeling from bad news and groping for answers.
Google and Facebook have promised to crack down on health misinformation in recent months .... But bogus health information cannot be eradicated from the Web....
https://www.washingtonpost.com/lifestyle/style/the...
-
PFAS: Controlling, Preventing, and Understanding Exposure
PFAS, or perfluoroalkyl and polyfluoroalkyl substances, are ubiquitous fluorinated organic compounds found widely in manufactured products, from firefighting foam to stain-resistant carpets. These water- and oil-repellent compounds are known to degrade slowly over time, and have been found in humans, drinking water, and even in Arctic ecosystems.
What do we know about human exposure to PFAS? How can contaminated media be treated? How can these compounds be controlled, and how can exposure be prevented? Last month, the Environmental Health Matters Initiative of the National Academies of Sciences, Engineering, and Medicine hosted a two-day workshop that brought together experts and stakeholders from academia, research, government, and industry to address these and other important questions about PFAS.
View recordings of the event here.
http://www8.nationalacademies.org/onpinews/newsite...
https://vimeo.com/showcase/6332191
-
Anti-CDK4/6 Strategy Tops Chemo in Premenopausal Breast Cancer
CDK4/6 inhibition plus endocrine therapy bests single-agent chemotherapy
-
KOLs Cover Pivotal Findings in Breast Cancer, Ovarian Cancer, GI Cancers, and Prostate Cancer
Hope Rugo, MD, and Joyce O'Shaughnessy, MD, recap the biggest breast cancer data, Mansoor Mirza, MD, highlights top abstracts in ovarian cancer, Tanios Bekaii-Saab, MD, shares insight on exciting gastrointestinal cancer research, and Brad McGregor, MD, covers pivotal prostate cancer trials.
-
I'd be curious to find out how many patients actually see the box that their implants come in. Is it like when you wear shoes out of the shoestore and they send you home with an empty shoebox? Somehow I just don't think we'd see the box anyway.
They also talk about brochures from the makers that help patients decide about reconstruction options. I sure didn't get any of those from my PS!
Oct 25, 2019 12:34AM Lumpie wrote: FDA Calls for Boxed Warning on All Breast Implants Agency seeks to boost genuinely informed patient consent
The FDA issued a draft guidance recommending that manufacturers of breast implants include a boxed warning that clearly spells out the risks of their products. The agency also called on implant-makers to include a patient decision checklist and list the devices' ingredients, and updated its own recommendations for implant rupture screening.
-
Re the implants, I am required to sign a page-long warning every time I get a scan. Given the issues raised, I don't think the box that the implants come in will be relevant. I feel certain that anyone getting them will be required to sign an extensive disclosure before surgery. As a practical matter, the record of disclosure must be acknowledged and scanned into the electronic medical record. So we can expect it to be on 8.5x11 paper (in the US) or other standard size paper. I just hope that there is meaningful "education" before the day of surgery! As serious as some of the problems have been, I think that if they do not make meaningful disclosures *before* the date of surgery, purveyers and surgeons are going to be inviting liability. These guys aren't stupid.
-
Anticoagulants and breast cancer survival, a nationwide cohort study
Pete T. Kinnunen, Mika O. Murto, Miia Artama, Eero Pukkala, Kala Visvanathan and Teemu J. MurtolaDOI: 10.1158/1055-9965.EPI-19-0147Abstract
Background: Various components of the coagulation cascade have been linked to breast cancer (BrCa) progression. In vivo results suggest that anticoagulants possess anticancer properties, but there are virtually no studies in human populations. Our nationwide study explored the association between anticoagulant use and BrCa survival. Methods: All anticoagulants used from 1995-2015 in women (n=73,170) diagnosed with invasive BrCa in Finland between 1995-2013 were identified from the national prescription database; women were identified from the Finnish Cancer Registry. Cox regressions were performed to analyze BrCa survival as a function of pre- and post-diagnostic anticoagulant use; analyses were conducted for different anticoagulant subtypes and overall. Models were adjusted for age, mammography screening, tumor clinical characteristics, comorbidities, statin use, antidiabetic use, and antihypertensive use. To control for immortal time bias, post-diagnostic anticoagulant use was analyzed as a time-dependent variable. Results: At a median of 5.8 years after BrCa diagnosis, 10,900 (15%) women had died from BrCa. In total, 25,622 (35%) women had used anticoagulants during the study period. Post-diagnostic anticoagulant use increased the risk of BrCa death (HR=1.41, 95% CI 1.33-1.49). The risk was especially high for low-molecular weight heparin, although the effect disappeared in long-term users. Conclusion: Anticoagulant use provides no clinical benefit for BrCa survival; however, the association between thrombosis and cancer might mask potential survival benefits. Impact: Future pharmacoepidemiological studies should adjust for anticoagulant use. Research should focus on the use of new oral anticoagulants because these are rarely studied and might be associated with improved BrCa survival.
- Received February 2, 2019.
- Revision received April 4, 2019.
- Accepted October 7, 2019.
-
ESMO Breast Cancer Roundtable: Episode 3
How do we sequence therapy in patients with advanced disease?
@{Video @ 10 minutes and transcript.}
https://www.medpagetoday.com/meetingcoverage/esmoe...
-
Breast Cancer Scare for Beyoncé's Dad
Mathew Knowles reveals his diagnosis
"...breast cancer is not only a woman's disease. Men can certainly get it too. Previously, "Shaft" actor Richard Roundtree and Kiss drummer Peter Criss have both publicly revealed their breast cancer diagnoses."
The article notes that he has talked with the New York Times and Good Morning America. Kudos to Mr. Knowles for taking action to build awareness.
https://www.medpagetoday.com/blogs/celebritydiagno...
-
CMS Aims to Broaden Coverage for NGS Testing in Breast, Ovarian Cancer
Expansion would include patients with risk factors for inherited susceptibility mutations
In a proposed decision memo on Tuesday, the agency stated that sufficient evidence exists to support testing when treating physicians determine that patients with breast and ovarian cancer have clinical indications for germline testing, risk factors for an inherited cancer, and have yet to receive such testing.
https://www.medpagetoday.com/publichealthpolicy/me...
-
New Study Shows Growing Shortage of U.S. Oncologists Poses Risks to Women's Health
Analysis Identifies the 10 Major U.S. Cities Most Likely to Suffer a Shortage of Oncologists
The demand for cancer treatment is expected to grow by 40 percent over the next six years and at the same time, the American Society of Clinical Oncology (ASCO) is projecting a shortage of more than 2,200 oncologists over the next six years.
https://www.doximity.com/press_releases/new_study_...
-
3D-Printed Device Finds 'Needle in a Haystack' Cancer Cells by Removing the Hay
Finding a handful of cancer cells hiding among billions of blood cells in a patient sample can be like finding a needle in a haystack. In a new approach enabled by 3D-printed cell traps, researchers are removing the hay to expose the cancer cells.
Next steps will be to narrow the channels in the device, test white blood cell removal without the use of biotin, boost the percentage of white cell extraction and connect cell traps to increase trapping capacity.
https://www.news.gatech.edu/2019/10/29/3d-printed-...
-
Chemotherapy may spread cancer and trigger more aggressive tumours, warn scientists
Many are given chemotherapy before surgery, but the new research suggests that, although it shrinks tumours in the short term, it could trigger the spread of cancer cells around the body.
It is thought the toxic medication switches on a repair mechanism in the body which ultimately allows tumours to grow back stronger. It also increases the number of 'doorways' on blood vessels which allow cancer to spread throughout the body.
https://stm.sciencemag.org/content/9/397/eaan0026
DOI: 10.1126/scitranslmed.aan0026
-
Ok that is a highly unsettling treatise. There is just so much we still don't understand about this disease.
-
Great article on melatonin someone on my Facebook Repurposed Drugs page posted yesterday:
-
Love the melatonin info. I have been on 20 mg at night since diagnosis (I worked up to that amount). I sleep very restfully and easily.
-
Living Proof
{This isn't exactly news, but some may be interested in this 2008 movie. It is a dramatization about Dr. Slamon who was instramental in developing developed Herceptin. Free to watch on YouTube.}
-
New Study Shows Regional Differences in Improved Survival of Patients with De Novo Metastatic Breast Cancer Over Time
The newly published article looked at regional differences in survival in patients with de novo MBC (dnMBC), which is a first diagnosis of breast cancer that is stage IV. The authors studied dnMBC patients in the Surveillance, Epidemiology, and End Results (SEER) 9 registry....They also studied an institutional cohort...They found that 5-year survival with dnMBC is different depending on where the patients lived. Survival also improved as new treatments were introduced. For patients followed from 1990 through the present day.... women with dnMBC had a 5-year survival rate of 44% compared to 20% of women with rMBC (recurrent MBC). Over the 20-year period, dnMBC 5-year survival improved ...from 28% to 55%, but rMBC survival decreased over time. The authors found a significant decline in rMBC over time, but no increase in survival.Details and links to articles here:DOI: 10.1158/1055-9965.EPI-16-0889 Published June 2017
https://link.springer.com/article/10.1007%2Fs10549-017-4529-5
https://doi.org/10.1007/s10549-017-4529-5
https://link.springer.com/article/10.1007%2Fs10549-018-05090-y
https://doi.org/10.1007/s10549-018-05090-y
-
Lumpie... that Chemo may be helping to spread the cancer and trigger more aggressive tumors is very unsettling indeed, to borrow Rah's word. I'll be asking my MO about this one.
-
Lumpie thank you for the link for Living proof! I've been trying to get it for about 2 months now, but unsuccesfully! Nowhere to see it legally in my country. I am watching it tonight. thank you
-
Simple blood test could spot breast cancer five years before any symptom
The new research, presented at the National Cancer Research Institute's conference in Glasgow, found that a blood test could identify changes in the body's immune response to substances produced by tumour cells...
Presenting the research at the NCRI Conference, researcher Daniyah Alfattani said: "The results of our study showed that breast cancer does induce autoantibodies against panels of specific tumour-associated antigens. We were able to detect cancer with reasonable accuracy by identifying these autoantibodies in the blood."
The most successful technique was able to identify disease in 37 per cent of cases with cancer, and rule it out, in 79 per cent of the control group.
"We need to develop and further validate this test," said Ms Alfattani. "However, these results are encouraging and indicate that it's possible to detect a signal for early breast cancer. Once we have improved the accuracy of the test, then it opens the possibility of using a simple blood test to improve early detection of the disease..."
Researchers said that with sufficient investment, tests could be available in clinics in four to five years.
ETA more info at this link: https://www.eurekalert.org/pub_releases/2019-11/ncri-sbt103119.php
-
Lumpie - thank you for the Washington Post link. A lot of misinformation and out right lies out there. Already confusing with the rapidly changing diagnosis and treatment of cancer, and the varying degree of success for each INDIVIDUAL. Sometimes I get discouraged hearing the "adds" from various cancer centers / cancer research centers that sponsor NPR. It sounds like there are individualized successful treatments, and for most, this just is not true. But the science is rapidly evolving, and maybe, someday there will be.
-
Public service announcement (not exactly breaking news):
If you live in the Baltimore/Washington area, I just got an update from the Cancer Research Institute (very pro immunotherapy) regarding an information session they are doing in Baltimore on Saturday, Nov. 16th from 10-3:30. It is free and looks quite interesting. The main speaker is Dr. Elizabeth Jaffee, the co director of the Sidney Kimmel Cancer Center at Hopkins. They are also going to have navigators there to talk with you about possible clinical trials. You can google Cancer Research Institute to get further info.
-
For some cancer patients, monitoring symptoms can extend their lives
A growing body of research has found that people with cancer who are routinely prompted to answer questions about their symptoms may live months longer and have a higher quality of life than people who don't track their symptoms as closely...
The results [of a new study analysing results from over 120,000 matched pairs of patients who were/were not surveyed about symptoms], published in May, were startling. Patients who answered the survey were less than half as likely to have died during the study period than people who never answered the questions.
Until the past few years, the idea that a patient's experience could be measured and then inform treatment decisions was seen as being too nebulous to be useful in treating cancer...
[An RCT published in 2017] found that people who reported their symptoms via the online program lived, on average, five months longer than people who didn't... [Another RCT published in 2017] reported in their preliminary analysis that patients who monitored symptoms lived, on average, seven months longer than patients who didn't. Earlier this year, their final analysis confirmed that survival benefit...
Wong said many institutions around the world have launched new programs to capture patient-symptom data with varied success.
https://www.washingtonpost.com/health/for-some-can...
-
Targeting metastatic breast cancer with CAR T-cell immunotherapy
A team of researchers from Fred Hutchinson Cancer Research Center and its partner institutions, University of Washington and Seattle Cancer Care Alliance, just received a coveted Department of Defense Breast Cancer Research Program Breakthrough award.
The four-year, $4 million award, led by principal investigators Drs. Cyrus Ghajar and Stanley Riddell of Fred Hutch, will launch an innovative investigation aimed at preventing late-onset, metastatic breast cancer. The team is developing an immunotherapy strategy utilizing immune cells called T cells that are armed with tumor-targeting chimeric antigen receptors, or CARs...
Ghajar's research, along with that of his postdoctoral researchers Goddard and Grzelak, focuses on disseminated tumor cells, or DTCs, the tumor cells that can lie dormant in breast cancer patients for years or decades after treatment for early stage disease before emerging as metastasis...
Using new advances in protein design developed in the Baker Lab at UW, the researchers believe it is possible to engineer unique, customizable CARs that will be highly specific for DTCs and can direct T cells to kill them.
-
On chemo helping the cancer spread, here is an interesting article from the website Science Based Medicine that explains the nuances in those results. The article takes issue with some promoters of alternative remedies that used that study to peddle their stuff. Skip that part and you will find a very good analysis of what these results say about chemo and cancer spread.
https://sciencebasedmedicine.org/does-chemotherapy-cause-cancer-to-spread/
-
Hi all,
the deadly results and statistics of conventional therapies speak for themselves...I can't believe that any intelligent person would defend the status quo, where 30% of stage 1 BC patients will eventually be diagnosed stage 4...
Instead of defending chemotherapy, they should work harder at finding treatments that not only work, but don't require that we lose life and limbs in the process...
-
Frisky - what is your source for that 30% of Stage I patients progressing to Stage IV number? People keep quoting that number but nobody has been able to produce a study showing that. At best, people come up with references to other people who have also quoted the number without backing it up. It seems like this 30% number that everybody throws around is based on something one single person said many years ago, also with no study to back it up. If you look at the actual number of women diagnosed with breast cancer every year vs. the number dying of it every year, that works out to ~15%. So if 100 women are dx'd with breast cancer at any stage in a given year, 15 will die of it in the same year. And the 100 women includes the 6-10% of women who are stage IV de novo. So are there scores of women getting stage IV breast cancer who go on to die of other causes? I don't understand how these numbers can add up.
-
To begin with, that would be 20%- 30% of early stage, which includes stages one through three, not just stage one.
I don't want to derail this thread. There is a discussion of this figure on the web site of Metastatic Breast Cancer Network, a reliable source in my opinion. There is also a long BCO thread on the topic.
-
Here's an article about the issue of provenance of that statistic:
https://www.medscape.com/viewarticle/849644#vp_1
Upshot: the origin of the stat appeared to be iffy:
a 1989 study of 644 patients with stage I (T1N0M0) or stage II (T1N1M0) breast carcinoma, all treated with mastectomy (J Clin Oncol. 1989;7:1239-1251). During the median follow-up of 18 years, 148 patients (23%) died of recurrent breast carcinoma.
Dr van't Veer and her colleagues presumably rounded their figures up (from 23% to 33%) because the referenced population included only patients with stage I and II disease, and therefore did not comprise all early-stage disease.
According to the National Cancer Institute (NCI), the definition of early-stage breast cancer is that which has not spread beyond the breast or the axillary lymph nodes. The range includes stage I, stage IIA, stage IIB, and stage IIIA disease.
So this particular 30%-ish statement from Dr van't Veer and colleagues appears to be an estimate based on a clinical study that is not contemporary. In short, it is not strong evidence.
The article goes on to describe an informal analysis of SEER data:
They looked at breast-cancer-specific mortality (as identified on death certificates) in 12 health districts in the United States from 2008 to 2012. They were surprised by the finding: "28% of the women who died of breast cancer during that time period had localized disease at diagnosis," said Dr Brawley.
But that's not the same as the percentage of early stage beast cancers that progress.
-
Wow I didn't expect a furious reaction after posting additional information to help put in context the terrifying assertion that neoadjuvant chemo causes cancer cells to spread and fuels metastases. Here is my takeaway from the article, which is hard to disprove:
<<Tumor cell dissemination as a result of chemotherapy reduces, not eliminates, the benefit of neoadjuvant chemotherapy, and it certainly does not "make cancer spread" in such a way that neoadjuvant chemotherapy is worse than no chemotherapy.>>
-
Unfortunately SEER counts people with de novo stage four breast cancer, but does not count people who had stage one, two, or three and then had a metastatic recurrence. The recurrence is ignored.
Again, I recommend reading the section about mbc statistics at MBCN. Org. There are sources cited for the information and a discussion of why the figure is hard to pin down.
-
Hapa..for me it's very simple...what are my odds of surviving stage 4? I'm being treated at MSK, and my various MOs there have NEVER EVER given me any hope...mind you...till a few months ago I had Mets only in the bones...I have progressed with Mets to the liver while being treated...some might find this okay...I find this disheartening....
As far as the 20 or 30% progressing...it's a well known fact, that's being accounted—surely optimistically—for by our conventional cancer institutions.
As far as this web site is concerned, most of the people still alive after 5 years are on Herceptin, which seems to be the only reliable treatment...and yet, recently one of our members that is on Herceptin came up with depressing statistics...better than the non HER2 disasters, but still disarming...
Also, this site is another precious source of information regarding progression from early stages, all you have to is read the info at the bottom.
Ultimately, we are all free to chose what to believe and I respect anyone that thinks the odds are improving...yes that could be true....but in comparison to what?
-
frisky, just wanted to sympathize; any kind of breast cancer sucks; chemo is brutal; metastatic breast cancer sucks exponentially more than non-metastatic breast cancer; breast cancer is a formidable challenge for medicine; it is phenomenally complex and the more we learn about it, the more complex it becomes. I am also for science and data and evidence-based medicine, and in my view alternative therapies are alternative not because they are an alternative, but because they cannot be proven to work by any reasonable standard -otherwise, they would become mainstream and conventional. To me, beyond science and reason and evidence, there simply is no alternative.
That article about neoadjuvant chemo causing spread doesn't mean one is better off without chemo. No need to terrorize us even more than we already are.
-
laughingull I didn't mean to scare anyone, the reality of the scientific facts and statistics are scary enough...the problem is that since I'm no longer disassociated from reality, I can no longer avail myself of the usual coping mechanisms.
I ultimately believe that knowledge will serve me better than soothing notions.
you're right...we don't really have any viable choices..all are known to be at best unreliable ..otherwise why would cancer, and better yet, cancer treatments be so terrifying?
and maybe not...I'm sure there are some people that can easily cope with the surgery, radiation, chemo...and the next ten years of estrogen suppression....I do ultimately wish you and everyone else a fearless experience and successful outcome. -
frisky,
I agree, knowledge is power. Much love and peace,
LaughingGull
-
Novel Surgery May Prevent Lymphedema in Patients with Breast Cancer
"Immediate lymphatic reconstruction is a preventive procedure to restore lymphatic connections in the arm," said Frederic Kolb, MD, plastic surgeon at UC San Diego Health. "This delicate surgery is performed at the same time the lymph nodes are removed and tested for cancer. Instead of treating patients after lymphedema presents itself, we hope to prevent the condition for patients who may be at risk."
During lymph node dissection, Kolb and his team map the drainage routes of the nodes in the upper arm. The team reconnects any disrupted channels by creating a "by-pass" to prevent swelling. Using a microscope, the team reroutes the tiny vessels, many less than the thickness of a dime...
"As a cancer surgeon, my primary goal is to accurately stage the cancer to identify which patients need more aggressive treatment," Sarah Blair, MD, surgical oncologist at UC San Diego Health. "In some patients, significant lymph node dissection can unintentionally result in damage to healthy tissue. With this procedure, we can help prevent lymphedema and give the patient a better overall experience and outcome."
-
Pharma's Ghost Labs Find New Life
Finding new tenants for former drug development sites isn't always easy. But a new, thriving industry has materialized to do just that.
Big Pharma has also changed how it conducts R&D. To cut costs, companies are doing less of their own research and are instead relying on making deals with smaller companies or university research divisions that have already successfully developed drug candidates or therapeutics, and often working with contract research organizations on the continued development of those products. "The old 'make what you sell, sell what you make' is no longer the preferred strategy,"
{Article is about real estate but has implications for pharmaceutical development, too.}
-
debbew - thank you for posting the link for novel surgery and preventing lymphedema. One more question to ask the surgeon tomorrow. This is the 3rd time for me, twice left, and now on right. The oncologist feels that each is new cancer, but when pressed, said there is no real way to know since cancer mutates so much. In June I noticed my right arm was swollen. And ultra sound at urgent care showed no blood clot and I was told to see my DR. It was odd, since the surgery had been on the left side. Eventually cancer diagnosed, and the thinking was that the cancer was the source of the lymphedema rather than prior treatment. I'm worried about the upcoming surgery, concerned that it will be much more complicated since it is in the axilla this time.
2009 ER+ left breast. 52 yrs. Lumpectomy, Sentinel node removal, negative. Radiation 6 weeks, tamoxifen 5 years. Dense lumpy left breast, normal right. Acupuncture offered at facility as part of integrative medicine. It really helped with anxiety/stress during radiation treatment.
2016 ER+ left breast. Probably a new cancer, but unknown. 4 rounds TC Aug-Oct 2016, Bi-lateral (my choice) Nov 2016, no reconstruction. 2 sentinel nodes remove, negative. Cold Capping using Chemo Cold Caps (DIGNICAP not available). Anastrozole 1 mg starting May 2017. Joint issues noticed immediately. Stopped Anastrozole after 3-4 months due to joint stiffness in. After several months of no AIs, fingers were feeling better. Started tamoxifen March 2018
10/2018 noticed stiffness and some trigger finger again. Was eating meat a lot more (daily) than normal. Usually 1-2 /wk. Have cut way back on the meat, seems to help, but one finger still very prone to trigger finger. Trigger finger seemed to be getting better, but now 4/2019 seems worse, is it the break from added turmeric to meals?
7/19/2019 - swelling in R-arm, opposite side from where lymph nodes removed. Noticed 6/18/2019. Could have been swelling earlier but wearing long sleeves. Trip to urgent care. They did ultrasound, concerned that there might be a clot, there was not. Started seeing lymphatic therapist 7/2/2019.
8/2019 CT, Breast/chest , neck/thyroid ultra sound
9/2019 DR ordered biopsy, said it could be lymphoma, cancer, benign lymphatic. Biopsy R-axilla. Cancer. Genetic test showed no known markers (20+ looked for)
9/29/2019 PET scan, no indication of spread. Arimadex and Ibrance prescribed to shrink tumor prior to surgery
-
Cryoablation and Immunotherapy: An Enthralling Synergy to Confront the Tumors
-
^^Thanks, BGRS, hope the info was useful!
Revamped cancer drug starves tumors in mice
A bacteria-derived compound called DON... kills tumors by inhibiting several enzymes that allow cancer cells to use glutamine. In clinical trials, however, the drug provoked severe nausea and vomiting, and it was never approved.
Now, Powell and colleagues have crafted a new version of DON that may be easier to stomach. It carries two chemical groups that keep it inert until it reaches the tumor's neighborhood. There, enzymes that normally loiter around tumors remove these molecular handcuffs, unleashing the drug on the cancerous cells. With this approach, "the vast majority of the active drug is where we want," Powell says.
To test their new compound, he and colleagues injected four types of cancer cells into mice, inducing tumors. They then dosed some of the animals with their next-generation DON. The drug worked against all four kinds of tumors, the scientists report today in Science. In untreated mice, for example, colon cancer tumors had grown more than five times larger after about 3 weeks. But in rodents that received DON, the tumors shrank and almost disappeared. The researchers found that the drug wasn't just throttling glutamine metabolism. It was also disrupting other aspects of the cells' biochemistry, such as their ability to use the sugar glucose.
One concern about drugs that target cancer cell metabolism is that they will also poison normal cells, including the immune cells that battle tumors. But Powell and colleagues found that their version of DON revved up T cells to destroy cancer cells. The scientists discovered that T cells deprived of glutamine by DON could switch to an alternative source of the raw materials needed to synthesize DNA and other key molecules, whereas tumor cells couldn't.
...Powell says safety testing of the drug will begin in people [next year].
Article: https://www.sciencemag.org/news/2019/11/revamped-cancer-drug-starves-tumors-mice
Paper (abstract is free): https://science.sciencemag.org/content/early/2019/11/06/science.aav2588
-
Human trials to begin next year using a virus to kill cancer
Scientists have created a new cowpox-style virus in a bid to cure cancer.
The treatment, called CF33, can kill every type of cancer in a petrie dish and has shrunk tumours in mice, The Daily Telegraph reported.
US cancer expert Professor Yuman Fong is engineering the treatment, which is being developed by Australia biotech company Imugene.
They are hoping the treatment will be tested on breast cancer patients, among other cancer sufferers, next year.
More context at: https://www.frontpagelive.com/2019/11/09/the-new-cure-that-can-kill-every-type-of-cancer-the-story-of-science-viruses-hope-and-money/
Company webpage about this virus: https://www.imugene.com/oncolytic-virus
-
Cowpox like virus to treat cancer? Amazing. Cowpox is what was initially used to vaccinate against smallpox. Jefferson saw this used in France, and introduced to to the US. Fortunately, the vaccine came a long ways since those days. With the elimination of smallpox world wide, the vaccine is no longer part of the usual vaccines. I wonder how this new treatment will work on those of us old enough to have gotten a smallpox vaccine as a child.
-
Not sure, but a neighbor of mine with glioblastoma that recurred after chemo/radiation is going to be treated with the polio virus--so far this polio treatment has shown the most positive results for glioblastoma as there really are not a lot of good options for that particular cancer. He said he got the polio virus immunization as a child and he had to get some sort of booster and make sure he was responding to the booster before they proceed. . .in some ways this treatment sounds similar. Here is some info on the polio virus thing he is doing. . .
"The poliovirus receptor is present on all solid tumors, which means that all solid tumors will get infected by the genetically modified poliovirus if put in contact with it," she said. "Another positive is that the poliovirus survives for only a short period of time: It triggers the infection and the immune activation, but then disappears. It does not stay around and decrease the long term immune response like other viruses might do."
In May 2016, the Food and Drug Administration (FDA) granted breakthrough therapy designation to the genetically modified poliovirus, PVSRIPO, which will hopefully help expedite research into this line of therapy.
For this study, the phase 2 trial is ongoing in adults with recurrent glioblastoma and a phase 2 trial is open for pediatric patients with a recurrent brain tumor. Investigators plan to soon begin trials in patients with melanoma and breast cancer." -
I saw the same information about the cowpox virus, and posted in on the ringworm, etc. link for stage 4 cancer. It sounds very interesting.
-
USFDA designates Indian invention a 'breakthrough device' for cancer
The Centre for Devices and Radiological Health (CDRH) of the US Food and Drug Administration (USFDA) has designated Cytotron—a device invented in India by a Bengaluru scientist—as a "Breakthrough Device" in the treatment of liver, pancreas and breast cancers...
Cytotron uses Fast Radio Bursts (FRB)—a high energy and powerful short radio bursts—in which both electric and magnetic components of the electromagnetic signals are "circularly" polarized...
FRBs can be used to communicate with the cellular command and control, to up or down regulate a specific protein or gene. In cancer cells, Cytotron does two things:First, it alters the protein pathways of a pro-apoptosis protein called p53 via p21 inducing programmed cell death in the cancer cells, and secondly, exposure to Cytotron stops metastasis by inhibiting the Epithelial Mesenchymal Transition cells, responsible for spread of cancer[.]
-
"Scientists have created a new cowpox-style virus in a bid to cure cancer.
The treatment, called CF33, can kill every type of cancer in a petrie dish and has shrunk tumours in mice, The Daily Telegraph reported.
US cancer expert Professor Yuman Fong is engineering the treatment, which is being developed by Australia biotech company Imugene.
They are hoping the treatment will be tested on breast cancer patients, among other cancer sufferers, next year."
-
Common early sign of cardiovascular disease also may indicate cancer risk, study finds
A Mayo Clinic-led study involving 488 cardiac patients whose cases were followed for up to 12 years finds that microvascular endothelial dysfunction, a common early sign of cardiovascular disease, is associated with a greater than twofold risk of cancer.
https://journals.sagepub.com/doi/full/10.1177/2047487319884246
-
'Smart needle' could speed up cancer detection 'with a less intrusive process'
Cancer detection could become much quicker and easier in the future after scientists developed a new "smart needle" that uses a mini laser to identify diseased tissue within seconds.
Researchers have demonstrated the technique works in the lab and have just begun a major three-year clinical trial to test it in living people.
They have focused on lymphoma so far but are hopeful the technique could also be used to diagnose other forms of the disease, such as breast and prostate cancer, further down the line.
-
NIH RO1 grant to help improve ultrasound tomography for breast cancer detection
"The current methods of mammography or tomosynthesis are based on X-rays," Anastasio noted. "Some small early stage cancers especially in younger women are difficult to detect in such images so the industry understands the need for improvement. We're investigating this new technology that can be useful for breast cancer imaging that is based on the use of ultrasound instead of X-rays. Not only is it safer because it doesn't involve ionizing radiation, it is more sensitive to certain tissue properties that will make it easier to detect subtle breast cancers..."
"We quickly realized that through the use of advanced image reconstruction principles and high-performance computing, we can actually do a better job of modeling the physics and reconstruct images of much better quality," Anastasio explained. "They almost look like MRI images in terms of resolution."
Both Duric and Anastasio chose to focus this technique on breast cancer detection, partly because it is a disease the affects a vast number of women, but also because it is a part of the body where ultrasound tomography will work relatively well.
https://www.eurekalert.org/pub_releases/2019-11/uoic-nrg111119.php
-
Axillary Evaluation Is Not Warranted in Patients Preoperatively Diagnosed With DCIS Core Needle Biopsy
- The authors of this retrospective study of 604 women with a preoperative diagnosis of ductal carcinoma in situ (DCIS) by core needle biopsy looked for predictors of upstaging and axillary lymph node metastasis. Upstaging to DCIS with microinvasion (20%) and invasive breast cancer (32%) was common, but positive axillary lymph nodes (7%) were not. Factors predicting upstaging on multivariate analysis included tumor size >2 cm on ultrasound and ER+/HER2+ status. Factors predictive of axillary lymph node metastasis included tumor size on pathology and number of lesions.
- The authors concluded that the finding of a low rate of axillary metastasis, even in the setting of a 52% upstaging rate in this study, supports the omission of axillary evaluation in low-risk patients.
-
HOUSEHOLD CHEMICALS COULD BE LINKED TO AGGRESSIVE FORM OF BREAST CANCER, SCIENTISTS BELIEVE
The team found many of the nuclear receptors behaved differently in the [triple negative] breast cancer samples. Using a computer model, they identified certain household detergents, antiseptics, industrial pollutants and prescribed medications which might to activate nuclear receptors, or change how they are expressed.
Study co-author Laura Matthews, a breast cancer and nuclear receptor expert at the University of Leeds, said in a statement: "We are now investigating how the environmental chemicals change the behavior of normal breast cells so we can understand how they might drive cancer development.
"We are also testing whether using drug combinations that target multiple NRs [nuclear receptors] at the same time might prevent or be an effective treatment for TNBC. Our goal is to reduce the number of people that develop breast cancer, and guide new therapies, so that more people can live beyond breast cancer," she said...
Justin Stebbing, professor of Cancer Medicine and Medical Oncology at Imperial College London... commented in a statement: "...This study opens up new avenues for research. However, for now there is no link between household antiseptics or chemicals to breast cancer."
-
No info in the article re. what chemicals exactly. --Rude! Well always good to use vinegar for cleaning! Cheap and pretty effective. Seems like if that is the case-- household detergents- chemicals that they would see a higher incidence of BC in people who clean for a living.
-
^^^I agree 2019whatayear; the study was just a computer model so it wasn't tied into epidemiological data, but they could have been more helpful on the details.
___________________________________________________________
Cardiac resynchronization therapy benefits cancer survivors with heart failure
A pacemaker-like device restored heart function in a group of cancer survivors -- mostly women with breast cancer -- who had suffered from heart failure as a result of chemotherapy treatment, a study in the Journal of the American Medical Association (JAMA) reports...
Known as the MADIT-CHIC study, it was the first of its kind to assess whether cardiac resynchronization therapy (CRT) could improve heart function in patients with congestive heart failure and cardiomyopathy, an enlargement of the heart due to chemotherapy side effects.
After six months with the implanted CRT devices, the 30 patients who received cardiac resynchronization therapy experienced significant improvement. The study, which took place between 2014 and 2018, was designed to address a problem that impacts more than half of people who receive anthracycline-based chemotherapies to treat cancer.
https://www.eurekalert.org/pub_releases/2019-11/uorm-crt111219.php
-
Researchers Halt Spread of Breast Cancer by Blocking Metastasis-Promoting Enzyme
In a breakthrough with important implications for the future of immunotherapy for breast cancer, UC San Francisco scientists have found that blocking the activity of a single enzyme can prevent a common type [luminol B] of breast cancer from spreading to distant organs.
The new study, published Nov. 14 in the journal Life Science Alliance, shows that these metastases can be stopped before they are able to lay the foundations for tumor growth. By administering an antibody that specifically targets and disrupts MMP9 activity, the scientists were able to prevent cancer from colonizing the lungs of mice. But interestingly, interfering with MMP9 had no effect on the primary tumor, which suggests that the enzyme's primary role in this scenario is helping existing malignancies metastasize and colonize other organs rather than promoting the growth of established primary tumors...
The researchers also discovered that interfering with MMP9 activity helped recruit and activate cancer-fighting immune cells to metastatic sites, a result with important implications for treating certain types of metastatic breast cancer with immunotherapy...
"These findings come at an exciting time in cancer immunology, with antibodies targeting MMP9 being actively explored for clinical use within the biotech industry," Plaks said. "There's been great interest in trying to use immunotherapy to treat metastatic breast cancers of the luminal B type, but so far, success has been limited. Our work indicates that a combination approach of immunotherapy with antibodies targeting MMP9 activity might actually succeed."
-
now all we have to do is stay alive for the next ten/fifteen years...
-
Profound.
-
Mechanism of a breast cancer drug points to a possible new therapy
Despite trastuzumab being a game-changing treatment for HER2-positive breast cancers over the past two decades, its success has come with key gaps in the understanding of how, exactly, it works...
Hartman and colleagues confirmed in mouse experiments and human cell lines that trastuzumab triggers a process called antibody-dependent phagocytosis, which is a way that specific immune cells engulf and eat particles, specifically tumor cells coated with the HER2 antibody.
They also found that by adding another antibody to remove a roadblock in this cell death process, they could strongly improve the drug's anti-tumor ability. The finding was notable because this roadblock for cell death is driven by the CD47 gene, which is highly expressed in HER2-positive breast cancer patients who have worse outcomes.
"Our finding suggests that blocking this CD47 axis could lead to an effective therapeutic strategy in patients," Hartman said.
https://medicalxpress.com/news/2019-11-mechanism-breast-cancer-drug-therapy.html
-
Environmental toxins. Reading "Anti Cancer Living " Cohen and Jeffries. In their chapter on "The Environment and Quest for Health" and "Appendix C, Environmental Toxin Hit List", the list is extensive and includes far more than just pesticides/herbicides. The book has an extensive bibliography. I used to read labels for added sugar, artificial ingredients. I need to become much more informed. Need to watch the soaps/shampoos, and other cleaners, toothpaste, Not ready to throw out all the yogurt containers I use for left overs and invest in glass containers.
-
Best, Worst, and Typical Cancer Survival: New Estimates Tool
"How much time have I got, Doc?" That's a question never far from the mind of most metastatic breast cancer patients. Unfortunately, accurate estimates are elusive. A new approach mitigates the difficulty of that tough task by offering not one but three estimates.
Belinda Kiely, MD, ...proposed offering patients best, worst, and typical scenarios derived from clinical trial data. Her system is not formalized as an online tool but is a simple math exercise.
...physicians who give advanced breast cancer patients one estimate, such as 12 months, are wrong 70% to 80% of the time.
Kiely's method involves using multiples based in part on overall survival curves from clinical trials...doctors estimate the expected survival time for a patient, **divide it by four to get the worst-case scenario, and then multiply by three to get the best-case scenario. The typical scenario is between a half and two times the doctors' estimated survival.**
...providing three scenarios helps patients prepare for the possible worst case and, at the same time, hope for the possible best case....subtype, extent of disease, comorbidities, and other factors determine outcomes. By using multiples derived from studies that closely reflect a given patient's situation, oncologists can offer a more nuanced assessment.
"Research shows that patients who discuss these issues with their doctor have better quality of life, are less likely to undergo aggressive end-of-life resuscitation, and are less likely to die in the hospital. But at the moment, we also know that many patients are not having these conversations."
https://www.medscape.com/viewarticle/921425?src=wnl_edit_tpal&uac=210289DR&impID=2169570&faf=1#vp_1
-
For anyone who is interested in finding out about clinical trials in immunotherapy, go to the Cancer Research Institute -- website is https://www.cancerresearch.org
I went to one of their patient summits today up at Johns Hopkins, and it was a fabulous program. Lots of opportunities for information sharing, both with patients and practitioners. Very worthwhile program (they already have 2 set up for 2020 -- see their website).
-
https://www.breastcancertrials.org/bct_nation/browse_trials.seam
is another great site to review a variety of breast cancer trials.
-
Could value-based care help cure diagnostic errors?
Dr. David Newman-Toker told the Diagnostic Error in Medicine conference that fee-for-service payments are "toxic to diagnosis" and eliminating them would significantly reduce errors. Dr. Mark McClellan said alternative payment models are an important step toward more rapid progress in reducing diagnostic errors, while Dr. Michelle Schreiber talked about quality measures based on diagnosis and said she would like to see quality and safety measures given more attention.
https://www.medpagetoday.com/publichealthpolicy/publichealth/83303
-
Breast Cancer Screening Policies Questioned Again
Current guidelines may miss early detection in women with family history
Researchers conducting a large national registry study recommended changes to current breast cancer screening guidelines that would make family history a more important consideration in setting ages to begin regular mammography.
https://www.medpagetoday.com/hematologyoncology/br...
-
Pivotal Data in HER2+ Breast Cancer Transform Paradigm
Erika P. Hamilton, MD, discusses several studies in the HER2-positive breast cancer space and sequencing challenges that have emerged.
Research Efforts in HER2+ Breast Cancer Focused on Optimizing Novel Agents
Gregory Vidal, MD, PhD, highights ways in which available and investigational agents are being evaluated across HER2-positive breast cancer settings.
Adjuvant T-DM1 Approaches EU Approval for HER2+ Early Breast Cancer
Will the phase III KATHERINE data lead to a European approval in the adjuvant setting?
Exciting Advances Continue in HER2+ Breast Cancer and Other Subtypes
Kurt W. Tauer, MD, FACP, discusses encouraging updates across the spectrum of breast cancer subtypes.
-
Arthritis drugs could prevent fatal spread of breast cancer
Research teams from the University of Manchester and the University of Sheffield discovered that a protein released by bone marrow, called interleukin 1-beta encouraged breast cancer cells to form secondary tumours once they reach the bone.
Tests found that this molecule can be blocked by the drug anakinra, already used to treat arthritis.
-
Study finds breast cancer recurrence score has different implications for men
A new study by Vanderbilt-Ingram Cancer Center (VICC) researchers published in Clinical Cancer Research, a journal of the American Association for Cancer Research, indicates that a lower threshold is needed for male patients to predict mortality using the genetic assay, Oncotype DX, a commercial diagnostic test.
-
Study Suggests Viable Alternative to Mastectomy After In-Breast Recurrence
Mastectomy rates low, good cancer control in selected patients
A second lumpectomy followed by partial breast re-irradiation (PBrI) was an effective alternative to mastectomy in women who had in-breast cancer recurrence after initial treatment with breast-conserving surgery and whole breast irradiation (WBI), a single-center, phase II study found.
Continued follow-up of patients enrolled in the NRG/RTOG 1014 trial demonstrated that a second breast-conservation approach using lumpectomy and partial breast re-irradiation for management of in-breast recurrence was associated with continued high breast preservation (5-year freedom from mastectomy rate of 90%), with good cancer control and low risk of toxic effects," the researchers wrote in JAMA Oncology.
They noted that approximately 10% of 10 women treated with lumpectomy and irradiation will have a recurrence of breast cancer in the ipsilateral breast -- i.e., in-breast recurrence -- which historically, has always been managed with mastectomy.
They cautioned, however, that this approach is not recommended for all patients with an in-breast recurrence after their first lumpectomy but rather only for women with small, recurrent disease amenable to a second lumpectomy and who are motivated to avoid a mastectomy.
https://jamanetwork.com/journals/jamaoncology/article-abstract/2755430
-
mysticalcity - thank you for the post to clinical trials. BC for the third time!!! When I contacted one research facility, they said they had no trials, did not know of any for my situatain, and would be prescribing the same treatment as my DR. They sounded bored with my history and treatment of BC. This site will help me do a little of my own "research" and maybe ask questions that I had not thought about.
2009 ER+ left breast. 52 yrs. Lumpectomy, Sentinel node removal, negative. Radiation 6 weeks, tamoxifen 5 years. Dense lumpy left breast, normal right. Acupuncture offered at facility as part of integrative medicine. It really helped with anxiety/stress during radiation treatment.
2016 ER+ left breast. Probably a new cancer, but unknown. 4 rounds TC Aug-Oct 2016, Bi-lateral (my choice) Nov 2016, no reconstruction. 2 sentinel nodes remove, negative. Cold Capping using Chemo Cold Caps (DIGNICAP not available). Anastrozole 1 mg starting May 2017. Joint issues noticed immediately. Stopped Anastrozole after 3-4 months due to joint stiffness in. After several months of no AIs, fingers were feeling better. Started tamoxifen March 2018
7/19/2019 - swelling in R-arm, opposite side from where lymph nodes removed. Noticed 6/18/2019. Could have been swelling earlier but wearing long sleeves. Trip to urgent care. They did ultrasound, concerned that there might be a clot, there was not. Started seeing lymphatic therapist 7/2/2019.
8/2019 CT, Breast/chest , neck/thyroid ultra sound
9/2019 DR ordered biopsy, said it could be lymphoma, cancer, benign lymphatic. Biopsy R-axilla. Cancer. Genetic test showed no known markers (20+ looked for)
9/29/2019 PET scan, no indication of spread. Arimidex and Ibrance prescribed to shrink tumor prior to surgery.
10/2019 – Stopped Tamoxifen. Started Arimidex and Ibrance. Brand name Arimidex so far does not seem to have the SEs that generics did, but stiff/trigger finger on left middle finger returned.
-
Amazing new technology for detecting cancer using a drop of blood!
https://mainichi.jp/english/articles/20191125/p2g/00m/0bu/030000c
-
T-DM1 Efficacy in Patients With HER2-Positive Metastatic Breast Cancer Progressing After a Taxane Plus Pertuzumab and Trastuzumab
- This observational study was designed to evaluate the outcomes of patients with HER2-positive metastatic breast cancer treated with T-DM1 after prior exposure to trastuzumab/ pertuzumab/ taxane. The median overall survival (OS) was not reached, with a 1-year OS rate of 82%. The objective response rate was 27%, with 40% of patients achieving durable disease control.
- T-DM1 appears to have meaningful activity among patients with HER2-positive metastatic breast cancer previously treated with pertuzumab plus trastuzumab and a taxane.
Commentary by Lillie D Shockney RN, BS, MAS, ONN-CG
These results are refreshing and hopeful for clinicians and their patients. T-DM1 is familiar to those who specialize in breast cancer, but it may not be to general medical oncologists. This could serve as a reminder to patients to obtain a second opinion from a large teaching hospital or comprehensive cancer center where specialization in breast cancer exists. Patients need access to the right treatment, and their treatment team needs to be totally knowledgeable and offer the right drug therapies that can provide optimal clinical outcomes.
https://www.practiceupdate.com/C/92586/56?elsca1=emc_enews_topic-alert
https://www.clinical-breast-cancer.com/article/S1526-8209(19)30671-8/pdf
DOI: https://doi.org/10.1016/j.clbc.2019.09.001 -
Stereotactic Ablative Body Radiotherapy for Bone Only Oligometastatic Breast Cancer
- This prospective trial was designed to evaluate the use of single-fraction stereotactic ablative body radiotherapy (SABR) for 15 patients with bone-only oligometastatic breast cancer. The 2-year local progression-free survival rate was 100%; the 2-year distant progression–free survival rate was 67%.
- SABR appears to be feasible and effective in this population. Randomized trials are warranted to compare outcomes with SABR and the current standard of care.
Commentary by Lillie D Shockney RN, BS, MAS, ONN-CGSABR is a new treatment option for patients that has not been usually utilized before. It may require a second opinion, and application of this treatment may need to be done elsewhere, particularly if the patient lives in a rural area and/or receives care from a general medical oncologist without knowledge or readily available access to this type of treatment. Accuracy of staging work-up needs to be factored in here, too, to confirm the patient has bone-only disease.
https://www.practiceupdate.com/C/92587/56?elsca1=emc_enews_topic-alert
https://www.thebreastonline.com/article/S0960-9776(19)30590-9/fulltext
-
Lumpie, please translate!
search Article
Diet-related metabolomic signature of long-term breast cancer risk using penalized regression: an exploratory study in the SU.VI.MAX cohort
Lucie Lécuyer, Céline Dalle, Sophie Lefevre-Arbogast, Pierre Micheau, Bernard Lyan, Adrien Rossary, Aicha Demidem, Mélanie Petera, Marie Lagree, Delphine Centeno, Pilar Galan, Serge Hercberg, Cécilia Samieri, Nada Assi, Pietro Ferrari, Vivian Viallon, Mélanie Deschasaux, Valentin Partula, Bernard Srour, Paule Latino-Martel, Emmanuelle Kesse-Guyot, Nathalie Druesne-Pecollo, Marie-Paule Vasson, Stéphanie Durand, Estelle Pujos-Guillot, Claudine Manach and Mathilde Touvier
DOI: 10.1158/1055-9965.EPI-19-0900
Abstract
Background:Diet has been recognized as a modifiable risk factor for breast cancer. Highlighting predictive diet-related biomarkers would be of great public health relevance to identify at-risk subjects. The aim of this exploratory study was to select diet-related metabolites discriminating women at higher risk of breast cancer using untargeted metabolomics. Methods:Baseline plasma samples of 200 incident breast cancer cases and matched controls, from a nested case-control study within the SU.VI.MAX cohort, were analysed by untargeted LC-MS. Diet-related metabolites were identified by partial correlation with dietary exposures, and best predictors of breast cancer risk were then selected by Elastic Net penalized regression. The selection stability was assessed using bootstrap resampling. Results:595 ions were selected as candidate diet-related metabolites. 14 of them were selected by Elastic Net regression as breast cancer risk discriminant ions. A lower level of piperine (a compound from pepper) and higher levels of AcetylTributylCitrate (an alternative plasticizer to phthalates), pregnene-triol sulfate (a steroid sulfate) and 2-amino-4-cyano butanoic acid (a metabolite linked to microbiota metabolism) were observed in plasma from women who subsequently developed breast cancer. This metabolomic signature was related to several dietary exposures such as a "Western" dietary pattern and higher alcohol and coffee intakes. Conclusions:Our study suggested a diet-related plasma metabolic signature involving exogenous, steroid metabolites and microbiota-related compounds associated with long-term breast cancer risk that should be confirmed in large-scale independent studies. Impact:These results could help to identify healthy women at higher risk of breast cancer and improve the understanding of nutrition and health relationship.
- Received July 29, 2019.
- Revision received October 3, 2019.
- Accepted November 18, 2019.
- Copyright ©2019, American Association for Cancer Research.
-
"Eating a Western diet and consuming alcohol/coffee in high amounts produces a pattern of metabolic effects that also correlate with higher risk of BC. These metabolic effects can be measured by a blood test, and may predict risk of BC before it develops."
-
ugh I don't like the vague *high amounts* on that. will look forward to more studies.
-
Don't like the side-effects of CHEMO? Then read this....
https://unitedwithisrael.org/israeli-chemo-breakth...
-
Well maybe Lumpie has access to the full study..
-
Hmmmm...." A lower level of piperin...."were observed in plasma from women who subsequently developed breast cancer." This is the ingredient that they say should be in your turmeric to make sure it carries through your body. That's why I take the Gaia brand. The piperin is already in it. My holistic doctor and my PCP both are very strong believers in turmeric to help prevent BC. This article seems to support that.
-
Very interesting observation Lala. Here’s an article on benefits of perine, bioperine, peperine
https://www.livestrong.com/article/534594-benefits... -
COMMENTARY
A Novel, Effective Way to Treat Stage IV Breast Cancer
-
marljen,
Interesting article. It's also worth it to read the comments, especially the first one. The patient did not continue her treatment, regressed, and subsequently passed away a while later. However, this methodology of treatment still seems promising if one would stick with it.
-
Oh thanks Bev/Jen, I didn't look at the comments. Well that's so disappointing. I wouldn't have posted it at all if I had seen that.
-
I think the theory behind the treatment still seems promising. It ties into a lot of things that I've been reading. So it was worthwhile to post!
-
marijen---I didn't have chemo or rads but my doctors did say that if I had, they would not have let me take the turmeric. That article you posted pretty much explains why. As with everything, it's best to run it by your doctor first before you take anything. (Then do what I do and run it by everyone on these boards who I've decided collectively know more than all the doctors!)
-
Re "run it by your doctor first"-- YMMV.
Unless the specific MO is *also* trained and experienced in complimentary practices, they will often say a blanket "no" to antioxidants as there are not double blind clinical trials proving their safety and helpfulness. (My home town MO said the same.) I also went to an Integrative Oncologist for a consult, and got very different advice. Due to his 30 years of clinical practice data, I had confidence in him and I followed his recommendations, which involved a boatload of antioxidants, including a heavy dose of curcumin daily. My hometown MO looked up every recommended supplement and found nothing contraindicating their use. I began the supplement protocol in early chemo and followed it throughout my treatment and am still on it. I feel insanely good-- no more aches and pains-- and I had a perfect response to chemo. Besides supplements I had an exercise regime and a diet regime. My home MO told me that he believes the complimentary practices made a large difference in my outcome. I was 3C by current rubric... 3.8 cm TNBC tumor and 3 cm lymph node. Grade 3. Got a pCR. It makes me so frustrated when I hear comments warning about supplements from non-specialists. I think they helped me beat my odds -- and so does my former-doubter MO.
-
Yes, it seems pointless to ask any of my doctors about supplements. Santabarbarian, was the integrative oncologist covered by insurance? Another problem is long term use of a lot of supplements can be very expensive. But I do believe they definitely improve health and fight cancer. I am taking quite a few.
-
Yes the Integrative Onc (Dr Keith Block) takes insurance and can treat you from afar even; many of his patients fly in for their chemos. But not everything he does gets reimbursed (he does IV curcumin for example, which was not available in my town). I was tempted to go to him but the thought of getting on a plane to Chicago every 3 weeks just sounded too daunting. I was able to duplicate most of what Dr Block would have done in my home area. Some of his innovations are to give much slower drips and to "pulse" the chemo according to circadian clock; that was another I could not duplicate but the rest I followed to the letter.
The consult I did was actually a third opinion so I did not submit it to insurance. It was $1800 for a four part consult-- I spoke to three different people for one hour each re diet supplements exercise stress/psychological.... and then got 1 hour with the MO. After you do this you can get 15 mins with doctor for $150 any time for those pesky next-generation questions.
Best $1800 I ever spent.
-
Thanks for the post SB - I am in the Chicago Area it is great to know this doctor is here. I am happy with my currrent MO and team - and she is pro supplements and integrative approaches to cancer treatment - and I'm on my last chemo so I am going to continue on with where I am and then see about the Block Center for their approach to cancer reoccurence prevention. My biggest accomplishment on this front so far is running throughout chemo :-) Thanks again SB!
-
Lumpie, can you find anymore info on this one?
Research team discovers drug compound that stops cancer cells from spreading
https://news.ohsu.edu/2018/06/22/research-team-dis... -
I also saw a holistic doctor when I first started treatment. I didn't have chemo or rads but had a pretty strong reaction to Tamoxifen including severe joint and muscle pain as well as nausea and dizziness that hit me pretty hard. This guy used to work under Dr Weil treating BC and has retired to my area. After my MO just kept saying take glucosamine the holistic doctor put me on Gaia turmeric, a good ginger and magnesium glycinate. Those 3 things made a huge difference. I saw him for a follow up and he suggested copious amounts of water to counteract the dehydration Tamoxifen causes. When I added that (along with my exercise/yoga regimen) I finally got relief from my SEs. My MO was very skeptical especially about taking turmeric but he researched it thoroughly and has become a believer as well. Heck I told my BS how I had suggested turmeric to my 82 year old dad who was looking at a double knee replacement and the turmeric took away all his pain, and my BS now takes it for his arthritis! These doctors will come around. We just have to keep pounding it into them!
-
Is the 21st Century Cures Act a Solution or a Problem?
The permissive drug approval process enabled by the 21st Century Cures Act may cause public health problems.
People use medications because they want to live longer and to feel better. Over the last few decades, FDA has put greater emphasis on measures of health outcome that are important to patients, such as length of life and quality of life.
However, drugs and devices are often evaluated on the basis of surrogate markers, including clinical lab tests that evaluate blood chemistry or tumor characters. These surrogates can be important if they are closely associated with health outcomes. But the surrogates are often uncorrelated with measures that are meaningful to patients.
the 21st Century Cures Act was motivated by the desire to speed up the drug approval process. It does that by allowing pharmaceutical companies to use surrogate markers rather than mortality and quality of life as evidence that their products contribute to longer or better lives.
the Act ... lowers the standards for the evaluation of medical devices
the Act... risks allowing drugs to be licensed on the basis of preliminary studies.
....the FDA process is slow and inefficient. But high standards used by FDA evolved because of terrible disasters such as thalidomide, diethylstilbestrol, and the Dalkon Shield intrauterine device. Cures are important, but so is safety. The 21st Century Cures Act is deserving of our continuing scrutiny.
https://www.theregreview.org/2019/05/07/kaplan-21st-century-cures-act/
-
Fewer Late-Stage Cancers Found With Annual Vs Biennial Mammography
Cancers detected in women who undergo annual mammography screening are smaller and less advanced than those found with biennial screening, according to a retrospective study.
https://www.medscape.com/viewarticle/921895?src=wnl_edit_tpal&uac=210289DR&impID=2189594&faf=1
https://press.rsna.org/timssnet/media/pressrelease...
-
Actionability of HER2-Amplified CTCs in HER2-Negative Metastatic Breast Cancer
- In this prospective phase II trial, the authors assessed the efficacy of trastuzumab-emtansine (T-DM1) in patients with HER2-negative metastatic breast cancer with HER2-positive circulating tumor cells treated with two or more prior lines of chemotherapy. Among the 154 screened patients, nearly 10% exhibited HER2-amplified circulating tumor cells. However, the ratio of HER2-amplified to HER2-negative circulating tumor cells was low, suggesting that, even in these patients, these are subclones associated with a lower tumor burden.
- Ultimately, 11 patients received treatment with T-DM1, which resulted in only 1 confirmed partial response and 4 stable disease as best response. The median progression-free and overall survival were 4.8 months and 9.5 months, respectively.
Commentary by Lillie D Shockney RN, BS, MAS, ONN-CGHER2 testing has been challenging from the start—several decades ago—and remains challenging. The accuracy of the pathology testing directly and profoundly influences what treatments will or may work for the patient. This study had a small "n" of 11 patients. It would seem worthwhile to have the original HER2 testing repeated on the original specimen to determine if other pathologists agreed with the negative results. Also, we know that a portion (~22%) of prognostic factors (ER, PR, HER2) of the metastatic lesions can and do become the opposite of what they originally were in the primary breast tumor. It raises the question whether that is what this study is actually demonstrating.doi:10.1186/s13058-019-1215-z -
Santabarbarian, would you be willing to post your supplement regimen?
Many thanks,
Lanne
-
If you search the Fenbendazole Thread, my whole list of supplements is on there. Most are antioxidants. All but Metformin are OTC.
-
santabarbarian - I went through 7 pages, can you give us another hint?
The Game Changer -"Low Dose Naltrexone and Cancer" https://player.vimeo.com/video/168562089
-
Ok, sorry-- I can't find it either! Here's the whole program of what I did for complimentary stuff, most of it from Dr Block and a few things per a naturopath in my town. NOTE: I had TNBC which may make a few recommendations different. I also have NO underlying conditions or health problems that others might have that might contraindicate some of this. So, YMMV.
MORNING meds 500 mg metformin (taken for anti cancer purposes not diabetes purposes); 400 mg Vitamin E & 400 mg pentoxifylline - for post rads fibrosis prevention
EVENING meds 500 metformin, pentoxifylline, ashwaghandha 600 mg, Magnesium Citrate 500 mg, Niacin 500 mg, Melatonin 20 mg (work up to 20 mg slowly)
Other Supplements, which I split up am/pm mealtimes... I do rotate a couple of these in and out, and give myself pill free days here and there when I need them... But basically each day I take:
D3 5000 IU , ALA 300 mg, Wild caught Nordic fish oil ~2000 mg, Curcumin 6000 mg, Quercetin 2000 mg, Vitamin C 1000-2000 mg, Berberine 1000 mg, Luteolin 100 mg, Sea Buckthorn 500-1000 mg, Rose Hips 500 mg, Astralagus 2600 mg, Feverfew 760 mg, Selenium 200 mg, Ubiquinol 200 mg, Resveratrol 500 mg, EGCG (Green tea extract) 1340 mg, B6 50 mg, Om Reishi Mushroom Superfood 1500 mg, Super Greens Organic green powder 8g, Zinc citrate 50 mg, Calcium D glucarate, 81 mg aspirin Took organic whey protein isolate during chemo for extra protein when I felt food averse.
Pectasol modified citrus pectin: 3 scoops/day. best on empty stomach. Took for 2 weeks prior to LX surgery. Going back now to it due to my high AR+ and the recent trial results re prostate cancer. Doubt it can hurt and it might help.
A couple of these supplements, like the PectaSol, were not suggested by Dr Block but by a naturopathic physician I see. But 90% was via Dr Block. Pentoxifylline from RO. Astralagus came in recently for blood support on the rec of a BCO friend.
During chemo I also took 750mg L Glutamine on day before, day of, and day after chemo per Dr Block. Claritin 2 days prior to chemo day for 7 days. Also did Fasting mimicking prior to each chemo (not Dr Block but via Dr Valter Longo). Also did a ton of heat on my tumor & node (hyperthermia). Lots of heat for 2-3 days prior to chemo. Heat is very damaging to cancer cells at temps not damaging to healthy cells.
Dr Block recommended Interval training or other aerobically intense workout 3x week & pilates or yoga 2x week and also support or meditation to deal w stress. I did all that. Did intervals on the morning of chemo and did well on exercise until the last 2 chemos made me too breathless.
Dr Block recommends an organic pescatarian/vegan whole food diet favoring anti cancer foods (alliums, peppers, ginger, berries, greens, etc) Pre and probiotics, legumes, etc. LOW egg, LOW dairy. I probably did a little too much of both of those but cut way way down from my former diet. I lost 30 lbs following these plans and feel FANTASTIC. No aches or pains that I used to have (I am 58).
Once a month, still, I take artemesinin suspension and ALA in am, then I get Hyperbaric Oxygen, then I go straight to my High dose C IV. I used to do this routine 2x a week during chemo but dropped back to 1x a month. after treatment. Also during treatment I got a few Vitamin D injections and a few glutathione injections. When in chemo, I would typically have chemo on a Monday, then do High dose C on Weds/Fri.
-
You must be GLOWING with health Santabarbarian! Thank you! (Saved) to my notes)
On the Metformin, I looked it up at my drug plan and it’s $117 per month. Does that sound right? And I’m wondering how hard it would be to get any conventional Oncologist to prescribe any proactive cancer drugs
-
Hospitals Sue Trump to Keep Negotiated Prices Secret
-
Thank you SantaB!
Lanne
-
SantaB (sorry, one more question),
Which curcumin supplement do you use?
Lanne
-
OK I am sorry lumpie to hijack your thread!! I think we need to get back to regularly scheduled programming but here are the answers.
1. I have been using Theracumin, which is by Integrative pharmaceuticals.
2. My MO gave me the metformin immediately when I asked. There is a lot of evidence on Metformin being a benefit in terms of less cancer/recurrence. It made me wonder why he had not suggested it!! On my Obamacare plan, my Metformin is only about $1 per month... but I might have a surprise next year when the copays re-start...
It differs hugely whether or not a MO is open to the off-label uses of drugs and whether they will embrace antioxidant supplementation. My MO is very conservative and was initially not on board. But getting my recommendations from ANOTHER MO might have blunted his skepticism a bit. And then he saw my outcomes. I had a 3.8 cm multifocal tumor in my breast and a 3 cm lymph node, grade 3 TNBC. He confessed later he would NEVER have predicted the outcome I got. Initially I asked him to explain the risks of antioxidants and of high dose C IVs. Mostly what he said is, "untested... we think it could possibly harm the effect of chemo... blah blah..." Since Dr Block has been using these supplements in his patients for decades with great results, I said, "Ok I have considered the risks and benefits and I am going forward." I wanted to be honest w my MO. To his great credit, he respected my ability to decide and he has been very generous in his comments about how much I helped myself and helped my outcome.
Many people doing off-label meds are going through the Care Oncology Clinic (COC)-- London based, but available in the US-- which has a 4 drug regimen they will give (doxycycline, metformin, lovastatin, and mebendazole). These 4 are based on Jane McClelland's work (How To Starve Cancer). When I asked my MO about it he said he would NOT give me any of the other drugs now because me being NED (risk/benefit analysis) but if I were fighting active disease it would be a different situation. The doxy and the mebendazole have risks when taken long term so he felt they are not worth it for prevention purposes.
-
Triplet Active in Anti-HER2-Exposed Metastatic Breast Ca
Regimen well tolerated with reduced-dose gemcitabine
Dual HER2-directed therapy after prior pertuzumab (Perjeta) exposure was active and well-tolerated when combined with gemcitabine (Gemzar) for women with metastatic HER2-positive breast cancer, a single-arm phase II trial indicated.
Among 44 evaluable patients, 73.3% were free of disease progression at three months following treatment with the triplet regimen of trastuzumab (Herceptin) plus pertuzumab and gemcitabine (95% CI 61.5%-87.5%)
At 27.6 months follow-up, median progression-free survival (PFS) was 5.5 months (95% CI 5.4-8.2) while median overall survival (OS) was not yet reached. The 3-month OS rate was 100%.
One patient had a complete response, 20% experienced a partial response, and disease stabilized in 52% of the group.
"After three months of therapy, if patients were deemed to be progression-free, gemcitabine could be held at the discretion of the treating physician and patients were maintained with antibodies alone," the authors noted.
Treatment was continued until disease progression or the development of unacceptable toxicity. The median duration of treatment was 20.8 months
"Our findings support the advancement of phase 3 trials comparing the efficacy of regimens containing trastuzumab and pertuzumab with standard and novel ERBB2-directed treatment in patients previously treated with this dual-antibody combination."
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2755853
doi:10.1001/jamanetworkopen.2019.16211
-
Hi Folks. I was traveling for Thanksgiving with minimal internet access. Hope everyone celebrating had a nice holiday.
I note that there has been a lot of discussion about supplements. I think that discussion would be more appropriately moved to a forum on the topic of supplements. I know that this is a topic of interest to many so I searched to see if could find one. To my surprise, I did not see much. Here are a few possibilities:
Opting out
https://community.breastcancer.org/forum/78/topics...
Alternative Forum
https://community.breastcancer.org/forum/121
Seems to me that a forum specifically discussing supplements would be worthwhile if anyone is interested in starting one. I think there would be a lot of interest. Scientific evaluation of supplements can be spotty so guidance and direction to meaningful resources/research would be a great way to support one another.
Thanks.
-
Lumpie - I like the idea of a forum dedicated to supplements. What a person takes and why., brands they like etc. Do they let the Oncologist/DR know what they are taking, and is the DR supportive or have any opinions. Usually the information on supplements is included on what ever forum someone is posting to. So information can be very scattered - but I'm finding this to be true of the forums in general. An ND recommended green tea (alot), a mushroom powder, among other supplements for my cancer. For the most part, my oncologist feels I should get as much as I can from real foods, and not supplements ( I agree, but sometimes it is hard to get "enough" of a particular substance in food). She also exressed some concern about the mushroom powder, since not mush is known about interaction with other drugs. I do take a number of supplements (mostly vitamins).
2009 ER+ left breast. 52 yrs. Lumpectomy, Sentinel node removal, negative. Radiation 6 weeks, tamoxifen 5 years. Dense lumpy left breast, normal right. Acupuncture offered at facility as part of integrative medicine. It really helped with anxiety/stress during radiation treatment.
2016 ER+ left breast. Probably a new cancer, but unknown. 4 rounds TC Aug-Oct 2016, Bi-lateral (my choice) Nov 2016, no reconstruction. 2 sentinel nodes remove, negative. Cold Capping using Chemo Cold Caps (DIGNICAP not available). Anastrozole 1 mg starting May 2017. Joint issues noticed immediately. Stopped Anastrozole after 3-4 months due to joint stiffness in. After several months of no AIs, fingers were feeling better. Started tamoxifen March 2018
10/2018 noticed stiffness and some trigger finger again. Was eating meat a lot more (daily) than normal. Usually 1-2 /wk. Have cut way back on the meat, seems to help, but one finger still very prone to trigger finger. Trigger finger seemed to be getting better, but now 4/2019 seems worse, is it the break from added turmeric to meals?
Swelling in R-arm, opposite side from where lymph nodes removed. Noticed 6/18/2019. Could have been swelling earlier but wearing long sleeves. Trip to urgent care. They did ultrasound, concerned that there might be a clot, there was not. Started seeing lymphatic therapist 7/2/2019. Stopped seeing lymphatic therapist early October. She did not think it would help until tumor removed/chemo'd/radiated into oblivion.
8/2019 CT, Breast/chest , neck/thyroid ultra sound
9/2019 DR ordered biopsy, said it could be lymphoma, cancer, benign lymphatic. Biopsy R-axilla. Cancer. Genetic test showed no known markers (20+ looked for)
9/29/2019 PET scan, no indication of spread. Arimidex and Ibrance prescribed to shrink tumor prior to surgery.
10/2019 – Stopped Tamoxifen. Started Arimidex and Ibrance. Brand name Arimidex so far does not seem to have the SEs that generics did, but stiff/trigger finger on left middle finger returned.
-
Novel Anti-HER2 Agents Look to Change Practice at SABCS
2019 program to also feature new data on immunotherapy
"It's one of the best meetings," "And it's the most important breast cancer meeting in the world."
Re DESTINY: "I think this is one of the most exciting anti-HER2 drugs out there."
Article includes discussion of several other trials... one on Kadcyla for early stage HER2+ disease.
-
FDA Approves Generic Everolimus Tablets
The FDA has approved 2 abbreviated new drug applications for everolimus (Afinitor) tablets for the treatment of patients with advanced hormone receptor–positive, HER2-negative breast cancer in postmenopausal women; advanced renal cell carcinoma; progressive neuroendocrine tumors (NETs) of pancreatic origin; progressive, well-differentiated, non-functional unresectable NETs of gastrointestinal or lung origin; and renal angiomyolipoma and tuberous sclerosis complex.
-
Giving common antibiotic before radiation may help body fight cancer
The antibiotic vancomycin alters the gut microbiome in a way that can help prime the immune system to more effectively attack tumor cells after radiation therapy. A new study in mice from researchers at the Abramson Cancer Center of the University of Pennsylvania found giving a dose of the common antibiotic not only helped immune cells kill tumors that were directly treated with radiation, but also kill cancer cells that were further away in the body, paving the way for researchers to test the approach in a human clinical trial. The Journal of Clinical Investigation published the findings today.
https://www.eurekalert.org/pub_releases/2019-12/uops-gca120719.php
-
Baicalein induces apoptosis and autophagy of breast cancer cells via inhibiting PI3K/AKT pathway in vivo and vitro
Baicalein, a widely used Chinese herbal medicine, has shown anticancer effects on many types of human cancer cell lines. However, little is known about the underlying mechanism in human breast cancer cells. In this study, we examined the apoptotic and autophagic pathways activated following baicalein treatment in human breast cancer cells in vitro and in vivo.
-
Effects of hormone receptor status on the durable response of trastuzumab-based therapy in metastatic breast cancer
This study investigated the clinical factors that influence patient response to trastuzumab (Herceptin) therapy in human epidermal growth factor receptor 2 positive (HER2+) metastatic breast cancer (MBC). Hormone receptor (HR) status was found to be a possible predictor of a strong response to trastuzumab-based therapy.
Only 10% of HER2+ MBC patients experience a lasting response of more than 3 years. The role of HR status in HER2+ treatment response is not well known.
This study included 153 women with HER2+ MBC who were treated with trastuzumab and either paclitaxel (Taxol) or docetaxel (Taxotere) as their primary treatment. The patient's HR status and metastases were reviewed. Average follow-up time was 28 months with an average age of 52 years. Progression-free survival (PFS; time from treatment until disease progression) and overall survival (OS; time from treatment until death from any cause) were measured.
HR- patients showed a longer average PFS (19 months), compared to HR+ patients (9 months). The OS of HR- patients was 37 months. HR+ patients had an OS of 47 months.
Bone metastases were also associated with a longer PFS (15 months) and OS (75 months) than metastases to internal organs which showed a PFS of 11 months and OS of 34 months.
The study concluded that HR status is a possible predictor of outcome in patients with HER2+ MBC who receive trastuzumab-based therapy. Sites of metastases were found to independently influence treatment response.https://medivizor.com/view_article/37085117?id=21147
https://link.springer.com/article/10.1007%2Fs10549-017-4175-y
https://doi.org/10.1007/s10549-017-4175-y
-
How Close Are We to a Blood Test for Breast Cancer?
- Researchers are looking at whether we can detect breast cancer via blood test.
- We're still years away from the test being available to the public.
- Early stage cancers shed very small amounts of most biomarkers into blood.
Cancer cells make antigens that cause the body to make antibodies known as autoantibodies. The test looks for the presence of autoantibodies against tumor-associated antigens (TAAs).
The team was able to make a panel that looked for autoantibodies against 40 antigens that are known to be associated with breast cancer.
Another blood test for breast cancer in testing claims to be able to detect 15 different biomarkers (microRNA and methylation markers) in the blood, spotting metastatic and recurring cancers at an early stage, as well as small tumors.
If funded and evaluated completely, the test could be available in about 4 to 5 years, the researchers said.
Early stage cancers shed very small amounts of most biomarkers into blood, making the pursuit for early detection tests fraught with challenges
"There are multiple subtypes of breast cancer, and to detect these cancers through a blood test may not be a one-size-fits-all approach," Berger said.
Different antigens may be needed to detect hormone receptor-positive breast cancer compared to HER2-positive breast cancer or triple-negative breast cancer...
Tests have to be accurate. They also need to show that they improve outcomes as well...
"We will get there,"
Article states research was presented at
https://conference.ncri.org.uk/
but no specific citation was provided.
{Article is aimed at a non-academic, non-medical audience.}
-
New Standard for Metastatic HER2 Breast Cancer
Consistent PFS, OS benefit with combination including oral HER2 inhibitor tucatinib
Patients with heavily treated metastatic HER2-positive breast cancer lived significantly longer with the addition of an investigational anti-HER2 drug to trastuzumab (Herceptin) and chemotherapy, a large randomized trial showed.
Almost three times as many patients were alive without disease progression after 1 year when treated with tucatinib, trastuzumab, and capecitabine, as compared with the two drugs (33.1% vs 12.3%). The 2-year overall survival (OS) was 44.9% with tucatinib and 26.6% without it. Among patients with brain metastases, a fourth remained alive without disease progression at 1 year versus none of the patients randomized to placebo in addition to trastuzumab and capecitabine.
"Tucatinib in combination with trastuzumab and capecitabine has the potential to become a new standard of care in this population with and without brain metastases."
"Overall, tucatinib reduced risk of progression or death by 50%," Tierstein added. "I think this regimen may be considered a new standard of care for pretreated HER2-positive metastatic breast cancer. Very exciting."
San Antonio Breast Cancer Symposium
Source Reference: Murthy RK, et al "Tucatinib vs placebo, both combined with capecitabine and trastuzumab, for patients with pretreated HER2-positive metastatic breast cancer with and without brain metastases (HER2CLIMB)" SABCS 2019; Abstract GS1-01.New England Journal of Medicine
Source Reference: Murthy RK, et al "Tucatinib, trastuzumab, and capecitabine for HER2-positive metastatic breast cancer" N Engl J Med 2019; DOI: 10.1056/NEJMoa1914609.
-
Lumpie, said it before and do so again....you are a STAR! You’ve hopefully an idea now how much it helps the rest of us knowing there are people like you out there dedicated to sharing their knowledge.
-
Thank you Karenfizedbo15!! You made my day!
-
Chemo-Free Regimen Feasible in High-Risk Luminal Breast Cancer
Downstaging just as frequent with endocrine therapy plus CDK4/6 inhibitor
-
Chemo-Free Regimen Feasible in High-Risk Luminal Breast Cancer
Downstaging just as frequent with endocrine therapy plus CDK4/6 inhibitor
A neoadjuvant chemo-free combination achieved similar responses to a standard chemotherapeutic regimen for postmenopausal women with high-risk luminal B breast cancer, a small randomized trial out of Spain indicated.
In the CORALLEEN trial, 46.9% of patients treated with the aromatase inhibitor letrozole (Femara) plus CDK4/6 inhibitor ribociclib (Kisqali) achieved a low risk of relapse (ROR) following surgery, as compared with 46.1% in the chemotherapy group...
"Neoadjuvant ribociclib and letrozole in high-risk luminal B breast cancer achieves high rates of ROR-low disease at surgery," said Gavilá during an oral abstract session here.
While Gavilá explained that chemotherapy does this just as well, and is the current standard treatment, it comes at the price of higher rates of toxicity.
a chemo-free treatment strategy based on CDK4/6 inhibition is worth exploring in future neoadjuvant trials,"
The Lancet Oncology
Source Reference: Prat A, et al "Ribociclib plus letrozole versus chemotherapy for postmenopausal women with hormone receptor-positive, HER2-negative, luminal B breast cancer (CORALLEEN): An open-label, multicentre, randomised, phase 2 trial" Lancet Oncol 2019; DOI: 10.1016/S1470-2045(19)30786-7.Secondary SourceThe Lancet Oncology
Source Reference: Cristofanilli M, et al "Time for a shift in molecular down staging in luminal breast cancer" Lancet Oncol 2019; DOI: 10.1016/S1470-2045(19)30806-X.
-
Residual Cancer Burden Predicts Patient Outcomes Across Breast Cancer Subtypes
Residual cancer burden (RCB) after neoadjuvant chemotherapy has been shown to be an accurate long-term predictor of disease recurrence and survival across all breast cancer subtypes, according to data from a large meta-analysis presented at the 2019 San Antonio Breast Cancer Symposium.
-
T-DM1 for Early Stage Breast Cancer
Promising efficacy but higher discontinuation rates and cost likely a deterrent
Adjuvant treatment with ado-trastuzumab emtansine (Kadcyla), or T-DM1, demonstrated acceptable efficacy as a standalone treatment for women with stage I HER2-positive breast cancer, but failed to reduce clinically relevant toxicities, a randomized phase II trial found.
The so-called ATEMPT study met its primary efficacy endpoint, with 97.7% of patients treated with T-DM1 remaining disease free at 3 years (95% CI 96.2%-99.3%), Sara Tolaney, MD, MPH, of the Dana-Farber Cancer Institute in Boston, reported here at the San Antonio Breast Cancer Symposium (SABCS).
...the rate of clinically relevant toxicities -- the study's other primary endpoint -- was no better than standard paclitaxel plus trastuzumab (TH), landing at 46% for both arms.
grade ≥3 non-hematologic events were similar between the T-DM1 and TH arms (10% vs 11%, respectively), as were rates of febrile neutropenia (0% vs 2%) and grade ≥4 hematologic events (1% vs 0%).
"It's also important to note that not all toxicities that are significant for our patients are captured in this clinically relevant toxicity endpoint, such as alopecia,"
"Given the low event rate seen in this trial, T-DM1 may be considered an alternative treatment approach to TH for select patients with stage I HER2-positive disease..." {but} "For stage I disease, paclitaxel and trastuzumab remains the standard of care."
Primary Source
San Antonio Breast Cancer Symposium
{Gratuitous editorial commentary: toxicities were similar (curious given that I think neutropenia is much more common on taxanes); not having (sometimes permanent) alopecia is a BIG deal!; the article discusses at some length the cost of Tx with Kadcyla. The bills I have seen would indicate that Kadcyla is less expensive than T&H, certainly less than TCHP. I would be interested to hear from others about billed costs of these drugs.}
-
HRT Has 20-Year Impact on Breast Cancer Risks
Prospective data confirm long-term benefit with estrogen-only and harm with added progestin
Menopausal hormone replacement therapy (HRT) with estrogen alone yielded lasting reductions in breast cancer incidence and death while estrogen plus progestin showed persistent increases in both, long-term data from two Women's Health Initiative (WHI) trials indicated.
At over 16 years of cumulative follow-up, women with prior hysterectomy randomized to estrogen-only HRT had a 23% reduction in breast cancer diagnosis compared to those assigned placebo (HR 0.77, 95% CI 0.62-0.92), driven in large part by fewer diagnoses of estrogen receptor-positive/progesterone receptor-negative disease,
Primary Source
San Antonio Breast Cancer Symposium
-
Subdivision of M1 Stage for De Novo Metastatic Breast Cancer to Better Predict Prognosis and Response to Primary Tumor Surgery
Patients with de novo metastatic breast cancer (MBC) constitute a heterogeneous group with different clinicopathologic characteristics and survival outcomes. Despite controversy regarding its prognostic value, primary tumor surgery may improve survival for selected patients.
Subdivision of M1 stage facilitates prognosis prediction and treatment planning for patients with de novo MBC. Treatment offered should be decided in a coordinated multidisciplinary setting. Primary tumor surgery may play an important role in the management of selected patients.
DOI: https://doi.org/10.6004/jnccn.2019.7332 -
Checkpoints Show Different Outcomes in Breast Cancer
Atezolizumab misses complete response benefit in triple negative patients
The PD-L1 checkpoint inhibitor atezolizumab (Tecentriq) plus chemotherapy came up short in getting women with early stage triple-negative breast cancer to a pathologic complete response in the neoadjuvant setting when compared with chemotherapy alone, researchers reported...
In the preliminary results of the NeoTRIPaPDL1 Michelangelo trial, 43.5% of patients achieved a pathologic complete response when they were taking atezolizumab and the chemotherapy regimen of carboplatin and nab-paclitaxel compared with 40.8% of those taking only the chemotherapy (P=0.66)
patients who had PD-L1 positive tumors fared better with atezolizumab therapy than women who had PD-L1 negative tumors. Women with a high level of PD-L1 were twice as likely to achieve a pathologic complete response if they were in the atezolizumab group of patients.
In the KEYNOTE-522 trial ...64.8% of the triple-negative breast cancer patients achieved pathologic complete response with pembrolizumab plus two chemotherapy regimens compared with 51.2% of patients treated with chemotherapy alone.
...atezolizumab appeared to show activity in the metastatic setting, and was surprised that it did not show similar activity in the early stage setting.
-
Yikes with the RCB study. I mean, I knew at some level, but this did not start my day off well...
-
I am in the same boat Lexica and I agree...BUMMER
-
Lumpie I can answer your question about the cost of those drugs. My Kadcyla is being billed at $8050 every 3 weeks. My Herceptin was $6300 and Perjeta was $5625 earlier this year (it went up again this year), again every 3 weeks. Taxol is cheap and was only a couple hundred dollars when every 3 weeks ($300-$400). Taxol and Herceptin without Perjeta would be cheaper than Kadcyla, but THP is more expensive. A large percentage drop the Perjeta due to side effects, and a lot of early stage never even go on Perjeta, they just do the one year of Herceptin. So it's valid to compare the cost of Kadcyla to TH like they did in the study, and from my billing rates Kadcyla would definitely be more expensive.
What I don't understand is why they would have someone who is early stage do one full year of chemo instead of one year of a biologic with relatively few side effects like Herceptin.
-
LoriCA,
Wow! Thanks for sharing that info. Where are you getting your drugs!? My were being billed at:
Herceptin $9,424 discounted to $8,010 per dose
Perjeta $12,180 discounted to $10,353 per dose
That was in April. I wonder if it went up after that? Yikes! I do not see the bills for my Kadcyla since I am in a clinical trial.
I know that my Taxotere was being billed at around $3,500 per dose. I also got Cyclophosphomide. Can't find cost records for it right now. (All of these are drug only prices. Does not include administration, etc.)
I was actually told by one woman that she was being bill approximately triple the amount I was. Insane.
The combination of drugs used and these very different price numbers would make a big difference in the total treatment cost for early stage. Based on the charges for my TCH vs your Kadcyla, the Kadcyla would be cheaper. As I noted, one huge advantage of Kadcyla would be avoiding hair loss. I realize that cost analysts may say "not a big deal" but for those of us that 1) live with the loss and 2) *never* get our hair back, it is a HUGE, HUGE deal. Not to mention the fact that I am tolerating Kadcyla so, so much better than TCH. I don't feel nearly as bad as on the taxane. Huge QOL issue for me.
PS: Does it not strike people as utterly crazy that we are all charged incredibly different prices for these drugs? Crazy-making!
-
Promising news for those of us with lymphedema!
-
Lumpie I'm not sure if some of the drugs are dosed based on weight, but I'm a petite 5'4" so maybe that affects my costs. I live in one of the most expensive areas of the country (LA metro) and everything is more expensive here, so I don't understand why someone in another part of the country would pay more. Unless maybe the volume of patients treated in an area like mine means the facilities get volume discounts on drugs hahaha! It is crazy that pricing could be so different for each of us. Someone once posted that their cost for H&P was $21,000 every 3 months and it left me scratching my head, how could that be? (And yes, the costs I posted were for drugs only.)
I agree about no hair loss and better QoL than a taxane. That's the reason I asked to move on to Kadcyla this time instead of trying another Herceptin + chemo combo. I wanted to keep my hair for Christmas this year haha! But still, a full year of chemo vs a few months when you're early stage is something to think about. QoL of Herceptin for one year is much better than QoL of Kadcyla, especially if they're like me and have a tough time getting along with Kadcyla. It says there is a higher discontinuation rate for Kadcyla than TH, and I'm guessing that's due to the SEs. I think Kadcyla would have to show a major improvement over TH to be worthwhile. And a small number of people do lose their hair with Kadcyla for some reason (3.9% according to manufacturer), so it's not a complete guarantee one wouldn't lose their hair.
Would be interesting to hear what early stage people think about it.
-
Thanks Murfy. Very interesting research about LE.
-
Denosumab Does Not Alter the Course of Early Breast Cancer
-D-CARE trial failure spurs reassessment of adjuvant treatment with bone-modifying agent
-
I don’t remember seeing this posted here yet. Sorry if I am reposting.
-
-
Radiotherapy for ductal in situ carcinoma ups mortality risk in invasive second breast cancer
For women with primary ductal carcinoma in situ (DCIS), use of radiotherapy (RT) is associated with increased rates of breast cancer-specific mortality for those women who subsequently develop an invasive second breast cancer (SBC), according to a study published in the November issue of the Journal of the National Comprehensive Cancer Network...
The researchers found that even after controlling for cancer stage, prior RT was associated with higher rates of breast cancer-specific mortality (hazard ratio, 1.70; 95 percent confidence interval, 1.18 to 2.45; P = 0.005). The risk trended higher in patients with ipsilateral versus contralateral SBC (hazard ratio, 2.07 versus 1.26; P = 0.16). Patients with ipsilateral SBC were younger and more often lacked estrogen receptor expression compared with patients who developed contralateral SBC...
https://medicalxpress.com/news/2019-12-radiotherapy-ductal-situ-carcinoma-ups.html
-
I feel like that article is misleading. It should be comparing survival in women who get radiotherapy after DCIS vs women who don't, with both groups randomly assigned. It could be that women who have radiotherapy and go on to develop a second breast cancer had a radiation-resistant strain of breast cancer to begin with, which is more aggressive and less treatable. Whereas the women who didn't have radiotherapy may have developed a second breast cancer more often, and many of theirs were successfully treated with radiotherapy, but just as many died of radiation-resistant breast cancer in the end. Not to mention, some of those women could have been recommended radiation because their DCIS was of a more aggressive variety and thus more likely to recur.
Edit: I tracked down the original article, and it does cover this possibility:
"One factor likely contributing to the finding of increased mortality associated with ipsilateral SBC after prior RT is that prior radiation to the ipsilateral breast limits subsequent salvage options in the same breast. In our cohort, the proportion of patients receiving RT for contralateral SBC was higher than the proportion receiving RT for ipsilateral SBC after DCIS (P<.001). Another hypothesis that may explain this finding is that BCS followed by RT is less effective in preventing recurrence of invasive disease that is more aggressive biologically, and therefore prior treatment with RT may in fact confer a worse prognosis among patients who develop an invasive SBC. Indeed, our findings showed that patients who developed ipsilateral SBC were younger at the time of SBC development and had breast cancers that were more likely to lack ER expression, characteristics that are associated with more aggressive cancer biology. These possible explanations for the increased mortality associated with prior RT are not mutually exclusive, and both may be true."
Full article for anyone who is interested: https://jnccn.org/view/journals/jnccn/17/11/article-p1367.xml
In any event, looking only women at who have gotten a second breast cancer for the study instead of comparing all women and seeing how many of them 1) got second breast cancers and 2) survived completely discounts all the women who were cured by the radiation they received. If you did a study the other way around, discounting all the women who died or had recurrence and looking at the effects of treatment in the remaining population, it would be totally ridiculous.
-
hapa, thats exactly the thought that occurred to me. Thanks for stating it so well.
-
-
A Genetic Test Led Seven Women in One Family to Have Major Surgery. Then the Odds Changed.
Two sisters, their mother and aunts showed a mutation on a BRCA gene and an elevated risk of breast and ovarian cancer. But these interpretations can be revised.
Read in The Wall Street Journal: https://apple.news/Ap2sanVeJRkatMHZ2NLBF-Q
Shared from Apple News -
marijen, I read this article in the WSJ yesterday, and just read again the comments from readers.
It's disheartening, in so many ways.
The family involved seems to have not understood that genetic information is ever-changing - this should have been clearly explained to them by a genetic counsellor, as it was explained to me 14 years ago.
The articles notes "There are tens of thousands of BRCA variants and new research reveals that not all confer the same level of risk to a patient. Some gene variants “have intermediate or moderate levels of risk, not full-blown risk," says Fergus J. Couch, a professor at the Mayo Clinic, whose lab has worked on some of these studies.". Seriously, this is being presented as new news? I knew this from my own reading 14 years ago prior to my discussions with the genetic counsellor, and this was confirmed in that discussion. Anything I've read that mentions risk levels associated with the BRCA1 and BRCA2 mutations always presents a range of risk, never a single number.
The way the family feels now, and the way the story has been presented, indicates that some or all of the women regret their decisions to have prophylactic surgeries, based on the new information about their BRCA mutation. Well, what about the fact that they still have the family history of cancer? That hasn't changed. And it's not well explained that the new VUS status for their particular BRCA mutation does not mean that this mutation might not in fact present a high risk - VUS means that maybe it will or maybe it won't, and we just don't know yet. That's covered off in the article in one short sentence that's easy to miss. I appreciate that the family members are angry because they had these surgeries thinking their risk was much higher - but they are still high risk. And with their family representing such a large percent of the people with this mutation, and with so many of them having had prophylactic surgeries, at this point it may be very difficult to ever truly know what their risk really was.
It's mentioned in the article, but not emphasized, that changing the assessment of a genetic mutation from high risk to VUS status happens to only 1% of genetic mutations. So this cautionary tale about a very rare situation will scare some people away from genetic testing; not knowing their positive status and taking preventative action might lead to some deaths from cancers that could have been averted.
Then there are the letters. So little understanding of why people get genetic testing and why those who test positive for a high risk mutation often choose prophylactic surgery. No understanding that screening can miss some breast cancers and that even with extensive monitoring, sometimes breast cancers are not found when they are early stage, or that sometimes early stage breast cancer kills. One writer mentioned a 100% survival rate for breast cancer caught early and no one has contradicted her and provided the facts. A few people, all personally affected, have mentioned that there is no effective way to screen for ovarian cancer and that most ovarian cancers are found at Stage III or IV, but no one unaffected seemed to have any idea about this. One man mentioned that he is BRCA positive and has had breast cancer but every other writer seems to think this is a female issue.
I know how poorly educated the general public is about the realities of breast cancer so the fact that they are even more ignorant about genetic testing and the implications of being positive shouldn't surprise me, but it is demoralizing.
-
This may have been posted before since it was in the news earlier this year, but I am just seeing it now, so thought I'd share.
Gain Fat—Lose Metastasis: Converting Invasive Breast Cancer Cells into Adipocytes Inhibits Cancer Metastasis
"Adipogenesis-inducing drug combinations repress metastasis in preclinical models"
"Delineation of the molecular pathways underlying such trans-differentiation has motivated a combination therapy with MEK inhibitors and the anti-diabetic drug Rosiglitazone in various mouse models of murine and human breast cancer in vivo. "
https://www.cell.com/cancer-cell/fulltext/S1535-6108(18)30573-7
Here is an easier - to -read article about the research:
"Scientists Successfully Turn Breast Cancer Cells Into Fat to Stop Them From Spreading"
-
New Standard Likely for Some Metastatic HER2 Breast Cancer
-
Study by Geisel group details process enzyme plays in cancer
Using cell models in the lab, the team found that LPL [Lipoprotein Lipase] docks on the surface of breast cancer cells, enabling them to absorb whole fat particles from the bloodstream...
Pinning down how cancer cells get the fat they need to replicate is important, Kolonin said, because patients need to know what effect their diet may have on their cancer risk or progression of their existing disease.
In an effort to reduce their consumption of carbohydrates and sugar — which cancer cells may use to make fat — some patients have turned to the high-fat, adequate-protein ketogenic diet, Kolonin said.
But if the Geisel researchers' findings are borne out in future studies, "reducing fatty acids in diet is something to consider," he said.
Then the question left for researchers is between carbohydrates and fat: "What's the worse of the two evils?" Kolonin said.
https://www.vnews.com/Dartmouth-researchers-find-breast-cancer-cells-gobble-up-dietary-fat-31464521
-
CytoDyn Reports Early, But Strong Positive Clinical Responses for Two Patients, One in Metastatic Breast Cancer and One in Metastatic Triple-Negative Breast Cancer Trials
CytoDyn... a late-stage biotechnology company developing leronlimab (PRO 140), a CCR5 antagonist with the potential for multiple therapeutic indications, announced today continued promising clinical responses from its metastatic triple-negative breast (mTNBC) Phase1b/2 trial and its trial investigating leronlimab for the treatment of metastatic breast cancer (MBC).
"In the first patient, we're encouraged to see that after 11 weeks these additional data provide further preliminary evidence of efficacy, as demonstrated by sustained undetectable levels of CTCs and a reduction of cancer-associated macrophage like cells (CAMLs)," said Bruce Patterson, M.D., Chief Executive Officer of IncellDx...
CytoDyn's second patient enrolled is a stage 4 MBC patient. The metastasis progressed to the liver, lung and brain... This patient received her first injection of leronlimab on November 25, with one 700 mg dose each week... "The results from two subsequent scans of the metastatic lesions for this second patient demonstrated shrinkage of the tumors at both timepoints following the first leronlimab injection, reduction in brain edema, and remarkably, disappearance of several metastatic tumors."
The U.S. Food and Drug Administration (FDA) has granted a "Fast Track" designation to CytoDyn for two potential indications of leronlimab for deadly diseases. The first as a combination therapy with HAART for HIV-infected patients and the second is for metastatic triple-negative breast cancer (mTNBC). Leronlimab is an investigational humanized IgG4 mAb that blocks CCR5, a cellular receptor that is important in HIV infection, tumor metastases, and other diseases including NASH...
In the setting of cancer, research has shown that CCR5 plays an important role in tumor invasion and metastasis. Increased CCR5 expression is an indicator of disease status in several cancers. Published studies have shown that blocking CCR5 can reduce tumor metastases in laboratory and animal models of aggressive breast and prostate cancer. Leronlimab reduced human breast cancer metastasis by more than 98 percent in a murine xenograft model. CytoDyn is therefore conducting a Phase 2 human clinical trial in metastatic triple-negative breast cancer and was granted Fast Track designation in May 2019.
-
Prescient Therapeutics (ASX:PTX) reports positive results in breast cancer drug trial
- Prescient Therapeutics (PTX) has reported a high response rate from its Phase 2a clinical trial for breast cancer
- All of the evaluable patients responded to the PTX-200 drug, with the disease completely eradicated in some patients
- All but one of these women are progression-free up to 40 months after treatment
-
Olma, your easier to read link didn't work, but when I cut & pasted the words in your link to a search bar, I got the article.
Thanks!
-
Taking certain vitamins during breast cancer chemo tied to recurrence, death
Use of dietary supplements that boost levels of antioxidants, iron, vitamin B12 and omega-3 fatty acids appeared to lower the effectiveness of chemotherapy, researchers report in the Journal of Clinical Oncology...
After accounting for other factors that might increase the risk of recurrence or death, they found patients who took any antioxidant at the outset and during chemotherapy - including carotenoids, Coenzyme Q10 and vitamins A, C, and E - were 41% more likely to have their breast cancer return and 40% more likely to die during follow-up compared to patients using no supplements...
Those taking B12 and iron supplements were at greater risk of recurrence and those results were statistically significant. Women taking B12 were 83% more likely to experience a recurrence and 22% more likely to die during follow-up compared to those who did not take those supplements. Women taking omega-3 supplements before and during chemo had a 67% higher likelihood of recurrence and those taking iron supplements were 79% more likely to experience a recurrence...
-
Nanoparticle therapeutic restores tumor suppressor [p53], sensitizes cancer cells to treatment [research not on bc but bc is often p53-deficient]
Investigators have long sought a way to restore the activity of tumor suppressor genes such as p53. Most recently, attention has turned to an approach developed at Brigham and Women's Hospital that uses nanotechnology to deliver synthetic messenger RNA (mRNA). Leveraging advancements in nanotechnology, investigators from the Brigham have found that restoring p53 not only delays the growth of p53-deficient liver and lung cancer cells but may also make tumors more vulnerable to cancer drugs known as mTOR inhibitors. The team's findings are published in Science Translational Medicine...
Shi and colleagues, including co-corresponding authors Omid Farokhzad, MD, MBA, (director of Brigham's Center for Nanomedicine) and Wei Tao, Ph.D., (faculty in the Center), and first author Na Kong, MD, used a redox-responsive nanoparticle platform to deliver p53-encoding synthetic mRNA. The synthetic p53 caused cell cycle arrest, cell death and delayed the growth of liver cancer cells and lung cancer cells in which p53 had been depleted. In addition, synthetic p53 made the cells more sensitive to everolimus, a drug which is an mTOR inhibitor. The team reports successful results in multiple in vitro and in vivo models...
The authors note that further preclinical development and evaluation will be needed to explore that translational potential and scalability of the approach as well as its applicability to other p53 mutations and other cancers.
"We expect that this mRNA nanoparticle approach could be applied to many other tumor suppressors and rationally combined with other therapeutic modalities for effective combinatorial cancer treatment," the authors write.
https://medicalxpress.com/news/2019-12-nanoparticle-therapeutic-tumor-suppressor-sensitizes.html
-
Adherence to Dietary Recommendations Among Long-Term Breast Cancer Survivors and Cancer Outcome Associations
Fei Wang, Hui Cai, Kai Gu, Liang Shi, Danxia Yu, Minlu Zhang, Wei Zheng, Ying Zheng, Ping-Ping Bao and Xiao-Ou Shu
Cancer Epidemiol Biomarkers Prev; Published OnlineFirst December 23, 2019; doi:10.1158/1055-9965.EPI-19-0872
http://cebp.aacrjournals.org/content/early/2019/12/21/1055-9965.EPI-19-0872.abstract
-
Prevalence of Inherited Mutations in Breast Cancer Predisposition Genes among Uganda and Cameroon Women
Babatunde Adedokun, Yonglan Zheng, Paul Ndom, Antony Gakwaya, Timothy Makumbi, Alicia Y Zhou, Toshio F Yoshimatsu, Alex Rodriguez, Ravi K Madduri, Ian T Foster, Aminah Sallam, Olufunmilayo I Olopade and Dezheng Huo
Cancer Epidemiol Biomarkers Prev; Published OnlineFirst December 23, 2019; doi:10.1158/1055-9965.EPI-19-0506
http://cebp.aacrjournals.org/content/early/2019/12/21/1055-9965.EPI-19-0506.abstract
-
re the antioxidants: not a double blind trial, a very small sample size, and the only supplements which had statistical significance in negative outcomes were B12, A, and iron.
-
thanks for the comment Santa B. That article scares the crap out of me b/c I took a multivitamin - as per my MO during chemo. The percentages seem Bonkers!
-
-
Obesity tied to higher breast cancer therapy-related cardiotoxicity risk
Obese individuals with stage I to III breast cancer who received anthracycline and/or trastuzumab had significantly higher odds of cardiotoxicity, compared with normal-weight patients, according to a French study in PLOS Medicine. Multivariable analysis also showed that obesity and trastuzumab treatment had an independent correlation with cardiotoxicity. Physician's Briefing/HealthDay News
https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1002989
https://doi.org/10.1371/journal.pmed.1002989
-
Some supplements during chemo may worsen breast cancer outcomes
Women with breast cancer who received any antioxidant supplement before and during chemotherapy had 41% and 40% increased odds of breast cancer recurrence and mortality at follow-up, compared with those without supplement use, researchers reported in the Journal of Clinical Oncology. The findings also showed 83% and 22% increased recurrence and death risk, respectively, among those who took vitamin B12 supplements, while those with omega-3 supplement intake before and during chemo and those who received iron supplements had a 67% and 79% higher likelihood of breast cancer recurrence, respectively.Reuters
https://ascopubs.org/doi/10.1200/JCO.19.01203
DOI: 10.1200/JCO.19.01203 Journal of Clinical Oncology
{This may be duplicative of info already posted but I wanted to be sure the DOI was available for future reference. I also want to point out the potentially obvious - that if supplements were taken to address deficiencies, such as anemia, were the supplements the problem or was the deficiency?}
-
Lumpie I thought the same thing...
-
It could also be that women who were using iron for anemia or B12 for neuropathy were more likely to have dose reductions or stop chemo early.
I was told to take B12 for neuropathy, along with B6 and biotin.
-
I was given to understand that one or more B vitamins (6? 12?) were widely used in Europe (and perhaps in other countries) because they were believed to reduce symptoms of neuropathy. (I don't have a citation.)
-
I was also told to take B-6 and B-12 to combat neuropathy. Sadly it didn't work as my feet are dead. On the other hand, I don't have any pain with my neuropathy, so who knows.
-
In my country, we are told to run from B12 during treatment. Really, everybody in our support FB group knows to avoid it. Interestingly, I joined a German FB group (not my country, but I speak German) and people were recommending to take B12. That suprised me, as you can imagine.
I was thinking the same as some of you say above. Maybe the defficiency is the problem, B12 is often taken by vegans...
-
I was told to take B6 - and that was the only B recommended to me by the Integrative Onc I saw. He did not suggest A or iron.
Here's another angle: I was told to take Omega 3 but ONLY from wild-caught Nordic fish (due to pollutants). I wonder if the 'cheap' brands of various vitamins may have less bioavailability or more pollutants in them....? When you pull up a given vitamin on Amazon there is often a huge range of prices and formulations to pick from... the study did nothing to differentiate those kinds of things.
-
When I was first diagnosed, I found a study of men, lung cancer and B12 online . The men who had taken high doses of B12 daily before diagnosis had a higher incidence of lung cancer. That article alone convinced me avoid B12 supplements and I had been using B12 for years on and off because I tend to be anemic (congenitally low hemoglobin so iron supplementation does not help).
After chemo, I found a B complex in CVS that had no more than 100% of RDA of each vitamin. I took that for awhile but now have stopped.
-
I buy my Omega 3 from the cancer center. My NP told me most fish oil supplements you get in the store are a waste of money. They use low grade fish and there is very little benefit in taking them.
-
'Are you kidding me?': Check out the price tags on 'combination drugs'
"It's an abuse of the system," said one critic. The "business model ... involves gouging insurers and health plans, which ultimately costs consumers."
Read in NBC News: https://apple.news/AfVtvQkE-S6ilLEYIBkKJ-w
Shared from Apple News -
AI 'outperforms' doctors diagnosing breast cancer
An international team, including researchers from Google Health and Imperial College London, designed and trained a computer model on X-ray images from nearly 29,000 women.
The algorithm outperformed six radiologists in reading mammograms...
https://www.bbc.com/news/health-50857759
Original abstract in Nature...
International evaluation of an AI system for breast cancer screening
We show an absolute reduction of 5.7% and 1.2% (USA and UK) in false positives and 9.4% and 2.7% in false negatives. We provide evidence of the ability of the system to generalize from the UK to the USA. In an independent study of six radiologists, the AI system outperformed all of the human readers: the area under the receiver operating characteristic curve (AUC-ROC) for the AI system was greater than the AUC-ROC for the average radiologist by an absolute margin of 11.5%. We ran a simulation in which the AI system participated in the double-reading process that is used in the UK, and found that the AI system maintained non-inferior performance and reduced the workload of the second reader by 88%. This robust assessment of the AI system paves the way for clinical trials to improve the accuracy and efficiency of breast cancer screening.
https://www.nature.com/articles/s41586-019-1799-6
[Uses Google's Tensorflow machine learning platform, but they aren't releasing the code due to internal dependencies. This isn't the first AI system to help/improve mammogram reading. IBM has a Watson-based system and MIT posted code for their system on github (https://github.com/yala/OncoServe_public) and there are others, including commercially available software aids.]
-
marijen, thanks for the link to the 'combination drugs' article. So frustrating.
-
Antibiotics failed, then a Minnesota man turned to an old remedy that worked
Haverty, 62, of Brownsville, Minnesota, had 17 surgeries over a decade to rid his right leg of a stubborn infection that lingered after knee-implant surgery.
...his doctor at the Mayo Clinic leveled with him: Antibiotics were proving ineffective against the klebsiella pneumoniae bugs causing Haverty's infection, and he would probably grow so weary of surgeries that he would eventually opt to have the leg removed at the hip.
He had no way of knowing his eventual cure lay in a bacteria-killing virus known as a "phage,"...
The rising incidence of "superbugs," which have evolved to resistant human-made antibiotics, is driving renewed interest in phage therapy. Experimental efforts a century ago to harness phages for infections faded from mainstream science partly because antibiotic drugs worked so well and were relatively cheap. Modern phage researchers and entrepreneurs now have the tools to rapidly analyze the genomes of bacteria and phages, and machine-learning may aid in finding the perfect match.
Adapative Phage Therapeutics (APT) plans to recruit patients in up to four different clinical trials at 10 sites in 2020. The company has nearly 1,000 phages meticulously cataloged and stored and is targeting eight common types of bacterial infections.
{This article isn't cancer specific, but the treatment approach is so fascinating, I wanted to share.}
-
Study Backs Breast Cancer Subtype That Had Been Questioned
Increased risk of fatal breast cancer versus ER-positive/PR-negative tumors
"The results support the existence of the ER-negative/PR-positive subtype and indicate that ER-positive/PR-negative and ER-negative/PR-positive tumors are distinct subtypes of breast cancer," the authors concluded. "The assessment of PR status provides valuable information for prognosis and for evaluating the benefit of endocrine therapy. Further studies and clinical trials are needed to optimize the treatment regimens for patients with single-hormone receptor-positive breast cancer."
Conclusions and Relevance In this cohort study, statistically significant distinctions between survival rates of patients with single hormone receptor–positive BC vs double hormone receptor–positive/double hormone receptor–negative BC were observed. Different strategies may be required for patients with single hormone receptor–positive tumors to ensure optimal treatment and maximum benefits from therapies.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2758208
doi:10.1001/jamanetworkopen.2019.18160
-
Lumpie, thanks for posting this. Noticed that you are a double negative too. Hopefully, identifying these subgroups and outcomes will be included in future treatment studies.
-
A dear family friend works for an organization that has created a running database of PubMed publications. If you look at the home page for PubMed, it says "PubMed comprises more than 30 million citations for biomedical literature from MEDLINE, life science journals, and online books. Citations may include links to full-text content from PubMed Central and publisher web sites." That's a lot of links, and they don't database it to make it easier to search.
The database my friend is working on is called meta.org. Here is a page on how it works. You can create customized searches and get notifications of new research posted. You will need to create an account, but it is FREE and always will be.
My first search term (and you can create multiples) is for triple negative breast cancer. Here is part of the page of searches, so you can see what it looks like.
I have just opened my account this week, so I am barely figuring out how to deal with it. Those of you who are even more research oriented than I might have a good time with this.
-
Coolio, thanks, MM!
-
Newly discovered behavior of known chemical compound might lead to breast cancer drugs that keep [ER+] tumors from coming back
...Tamoxifen, and drugs like it, block the ER-alpha receptor, while fulvestrant and similar drugs induce the cell to degrade it. By blocking or degrading the ER-alpha receptor, these anti-hormonal drugs greatly reduce the signal for the cancer cell to grow and reproduce. But, as Prossnitz and his team have previously shown, they also activate GPER, and GPER signals the cell to keep growing and reproducing.
Most breast cancer cells follow the ER-alpha signal and die on schedule when ER-alpha is blocked or degraded. But a very small number of breast cancer cells may follow the GPER signal and survive. And those cells can grow into aggressive tumors that no longer respond to anti-hormonal drugs.
Prossnitz and his team discovered a compound some years ago called AB-1 that binds to ER-alpha but does not activate GPER, thereby avoiding the undesirable side effect of current anti-hormonal drugs. In their Cell Chemical Biology paper, they report their studies that describe AB-1's unique binding and activity behavior.
https://www.newswise.com//articles/discovery-could-lead-to-new-breast-cancer-drugs
-
Genetic study provides most comprehensive map of risk to date of breast cancer risk
A major international study of the genetics of breast cancer has identified more than 350 DNA 'errors' that increase an individual's risk of developing the disease. The scientists involved say these errors may influence as many as 190 genes...
In this new study, researchers from hundreds of institutions worldwide collaborated to compare the DNA of 110,000 breast cancer patients against that of some 90,000 healthy controls. By looking in much closer detail than was previously possibly, they identified 352 risk variants. It is not yet clear exactly how many genes these target, but the researchers have identified 191 genes with reasonable confidence; less than one in five of these had been previously recognised.
https://www.sciencedaily.com/releases/2020/01/200107122305.htm
-
New Compounds Block Master Regulator of Cancer Growth, Metastasis
Scientists have developed new drug compounds that thwart the pro-cancer activity of FOXM1, a transcription factor that regulates the activity of dozens of genes. The new compounds suppress tumor growth in human cells and in mouse models of several types of human breast cancer...
"FOXM1 is a key factor that makes breast cancer and many other cancers more aggressive and more difficult to treat," Benita Katzenellenbogen said. "Because it is a master regulator of cancer growth and metastasis, there has been great interest in developing compounds that would be effective in blocking it."The research is promising, but preliminary, the scientists said. Full development of new anti-cancer drug agents can take more than a decade from this stage of discovery.
https://scitechdaily.com/new-compounds-kill-breast-cancer-cells-and-block-tumor-growth/
-
For those who are HER2+ -- this just appeared in the National Cancer Institute newsletter about two new treatments
https://www.cancer.gov/news-events/cancer-currents...
-
https://www.practiceupdate.com/C/94747/56?elsca1=emc_enews_topic-alert
Re: Clinical and pathological factors influencing risk of late distant recurrence in ER+ ILC
-
Murfy - thank you for the lymphedema post. I will ask the DR. Right now my DR is very hopeful that the Ibrance will knock out the tumor in the axilla causing it, and that no more treatment will be needed. It is on the contraleteral side where lymphnodes removed. Have you heard anything about the success rate of surgery for lymphedema? DR, a surgeon, and lymphatic therapist not confident in surgery approach, not available in my state.
2009 - Left. Lumpectomy, 2 nodes checked, radiation, tamoxifen 5 years
2016 Left, again. Chemo, bi-lateral (my choice), AI initially, switched to tamoxifen (SEs)
2019 - Sweeling in right arm. Scans and biopsy revealed cancer in R- A axilla. Now on Ibrance.
-
Molecule 'selectively killed [triple negative] cancer cells,'
[A] small molecule discovered in animals on the seabed off the coast of Bjørnøya in 2011 [is being investigated for its effects on caner].
The molecule is part of a so-called hydroid – a collection of single cells joined together in a plant-like form and stuck on the seabed. Tests of its impact on multiple cell lines revealed many that were unaffected, but breast cancer cells showed the greatest impact.
The largest impact was the samples against a special type of breast cancer cells including triple-negative breast cancer...
"If it can be developed into a medicine, it will be a completely new treatment alternative for a group of cancer patients who now have limited treatment options," [Kine Østnes Hansen, an associate researcher at UiT Norway's Arctic University] said.
-
Flu vaccines may shrink tumors and boost cancer treatment
-
nice one Marijen
-
-
That is pretty amazing Bev/Jen. It's good for 10 autoimmune diseases and fatty liver. I wonder what the autoimmune diseases are as a lot of us have them.
-
Wow! Thanks for posting!
-
Marijen,
I also wonder if this would be applicable to non-TNBC cancer at some point, since it sure sounds like some kind of wonder drug.
-
another nice one BevJen!
-
Thanks BevJen, I think Leronlimab is also for other types, as CCR5 expression could be observed in many different cancers....
-
How proton radiotherapy can kill cancer in milliseconds
New research in mice shows "for the first time" that scientists can use protons to administer radiation therapy in a matter of milliseconds, killing cancer cells while protecting healthy tissue.
https://www.medicalnewstoday.com/articles/327476.p... -
New Cardiac Abnormalities Following Radiation Therapy in Breast Cancer Patients Treated With Trastuzumab
- "This retrospective study was designed to evaluate imaging abnormalities following modern radiation therapy and trastuzumab for breast cancer. Left-sided radiation was associated with an increase in new cardiac abnormalities. The incidence of new abnormalities correlated with radiation dose exposure." – Neil Majithia, MD
- New cardiac abnormalities appear to be relatively common among patients with breast cancer treated with trastuzumab plus radiation. Further studies are warranted to evaluate the long-term clinical significance of these abnormalities seen on imaging.
-
Molecular Imaging to Identify Patients With Metastatic Breast Cancer Who Benefit From Endocrine Treatment Combined With Cyclin-Dependent Kinase Inhibition
- This study was designed to evaluate the predictive benefit of positron-emission tomography with estrogen-tagged labeling (FES-PET) for 27 patients with ER+ breast cancer treated with letrozole and palbociclib. The median time to progression was 73 weeks in those with 100% FES-positive disease versus 27 weeks in heterogenous FES-positive disease and 15 weeks in those without FES positivity.
- FES-PET may identify patients with ER+ breast cancer who will benefit from the addition of a cyclin-dependent kinase inhibitor to letrozole.
Commentary by Lillie D Shockney RN, BS, MAS, ONN-CGIt is wonderful to see that FES-PET may provide a means of helping to determine which patients with hormone receptor–positive metastatic disease may benefit most from endocrine treatment combined with a CDK-inhibiting drug. The authors discuss the difficulties in obtaining biopsies from metastatic lesions, which can be correct in some cases. A bigger issue, however, is that, in many cases, no attempt is made at all, and treatment remains based on the primary lesion in the breast to determine the prognostic factors of the metastatic lesions, which is a mistake and a violation in the standard of care.
Whatever can be done to make it easier on the patient (biopsies of other organ sites are quite painful) and potentially more accurate in determining the degree of positivity of each metastatic organ site can really go a long way in potentially helping to determine who are the right candidates for this therapy. Those benefiting seem to benefit for a long time, which is wonderful, truly making this disease a chronic illness that is manageable.
-
Things are changing! "Innovators have invented a better way for surgeons to locate tumors during lumpectomies for breast cancer."
-
umakemehappy ...GPS guided surgery. That's really exciting. For surgeons for sure. Interesting reading. Thanks!
-
Inclusion of endogenous plasma dehydroepiandrosterone sulphate and mammographic density in risk prediction models for breast cancer
Marike Gabrielson, Kumari A. Ubhayaseker, Santosh R. Acharya, Mikael Andersson Franko, Mikael Eriksson, Jonas Bergquist, Kamila Czene and Per Hall
DOI: 10.1158/1055-9965.EPI-19-11Abstract
Background Endogenous hormones and mammographic density are risk factors for breast cancer. Joint analyses of the two may improve the ability to identify high-risk women. Methods This study within the KARMA cohort included pre-diagnostic measures of plasma hormone levels of dehydroepiandrosterone (DHEA), its sulphate (DHEAS) and mammographic density in 629 cases and 1,223 controls, not using menopausal hormones. We evaluated the area under the receiver-operating curve (AUC) for risk of breast cancer by adding DHEA, DHEAS, and mammographic density, to the Gail or Tyrer-Cuzick 5-year risk scores or the CAD2Y 2-year risk score. Results DHEAS and percentage density were independently and positively associated with breast cancer risk (P=0.007 and P<0.001, respectively) for postmenopausal, but not premenopausal, women. No significant association was seen for DHEA. In postmenopausal women, those in the highest tertiles of both DHEAS and density were at greatest risk of breast cancer (odds ratio (OR) 3.5; 95% confidence interval (CI) 1.9-6.3) compared to the lowest tertiles. Adding DHEAS significantly improved the AUC for the Gail (+2.1 units, P=0.008) and Tyrer-Cuzick (+1.3 units, P=0.007) risk models. Adding DHEAS to the Gail and Tyrer-Cuzick models already including mammographic density further increased the AUC by 1.2 units, (P=0.006) and 0.4 units (P=0.007), respectively, compared to only including density. Conclusion DHEAS and mammographic density are independent risk factors for breast cancer and improve risk discrimination for postmenopausal breast cancer. Impact Combining DHEAS and mammographic density could help identify women at high risk who may benefit from individualised breast cancer screening and/or preventive measures among postmenopausal women.
- Received September 11, 2019.
- Revision received November 6, 2019.
- Accepted January 10, 2020.
- Copyright ©2020, American Association for Cancer Research.
-
Acid reflux drugs may have negative side effects for breast cancer survivors
New Ohio State University research shows an association between breast cancer survivors' use of proton pump inhibitors (PPIs) and reports of problems with concentration and memory. On average, cognitive problems reported by PPI users were between 20 and 29 percent more severe than issues reported by non-PPI users. PPIs are sold under such brand names as Nexium, Prevacid and Prilosec.
https://www.sciencedaily.com/releases/2020/01/200117110840.htm
Study DOI: 10.1007/s11764-019-00815-4
-
Some happy reading!
Immune cell which kills most cancers discovered by accident by British scientists in major breakthrough
.
-
Interesting article Kanga Roo. From the article it sounds like they plan to start doing human trials maybe in November. I wonder if this is doing well in trials how long we would have to wait before it could be made available...5 to 10 years? I don't know what the timeframes are in the UK for new treatments. Does the UK have the "Right to Try" like the USA now has?
-
I hope we here more about this 'new' immune cell! wow! Exciting!
-
Oh my gosh, billions spent on cancer research and they find this by accident! I hope it lives up to even a fraction of its potential!
-
Dear all, what Kanga_Roo posted... That would be so crazy... I don't know even what to say, and although sounds "too easy and good to be true", CAR-T was just the same genius story, which we have already forgotten - we simply use these therapies today. Let's hope for the best, let's hold on!
Husband Saulius
-
Not as dramatic, but more upbeat reading...
Dozens of non-oncology drugs [have newly discovered ability to] kill cancer cells
Researchers tested approximately 4,518 drug compounds on 578 human cancer cell lines and found nearly 50 that have previously unrecognized anti-cancer activity. These drugs have been used to treat conditions such as diabetes, inflammation, alcoholism, and even arthritis in dogs.,,
The surprising findings, which also revealed novel drug mechanisms and targets, suggest a possible way to accelerate the development of new cancer drugs or repurpose existing drugs to treat cancer.
https://www.sciencedaily.com/releases/2020/01/200120113130.htm -
UW-Madison professors create revolutionary GPS device to help surgeons find breast cancer tumors during removal
Before the SmartClip, for the last 70 years, when doctors biopsy a breast cancer tumor, they also insert a little clip at the center of the tumor. But when it comes time to remove the tumor, surgeons can't see where that clip is...
In order for the surgeons to know where the tumor is, right before surgery a radiologist has to mark the area with a wire [which is stressful for patients].
The SmartClip is streamlining the breast cancer removal process. It can be placed during biopsy weeks or months before surgery, cutting out an additional procedure and possible scheduling conflicts with the radiology department.
-
Alcohol Consumption, Cigarette Smoking, and Risk of Breast Cancer for BRCA1 and BRCA2 Mutation Carriers: Results from The BRCA1 and BRCA2 Cohort Consortium
Cancer Epidemiol Biomarkers Prev; Published OnlineFirst December 2, 2019; doi:10.1158/1055-9965.EPI-19-0546
http://cebp.aacrjournals.org/content/early/2020/01/21/1055-9965.EPI-19-0546.abstract
-
A Trickster Enters the Fight Against Metastatic Cancers - Scientific American
https://www.scientificamerican.com/custom-media/a-trickster-enters-the-fight-against-metastatic-cancers/?mvt=i&mvn=5f65a57f546f4dcca5ab47f6dfda6a55&mvp=NA-SCIEAMERLIVE-11237933&mvl=HomePopular
-
Lumpie, are you ok and just taking a break? Just wondering if things a reasonably OK with you
-
Karenfizedbo15: you are so thoguhtful to be concerned! Doing pretty well here actually. Recent scans were stable - yeah! I've just slowed down a bit. Had *a lot* going on on the personal side. Needed some down time over the holidays. Kinda got overwhelmed with the amount of (good) info (some of it repetitive) coming out of San Antonio. And after that... seems like there is a lot of stuff that is either of marginal value or such early bench science that ... i have to try not to get disillusioned about how long it will take to turn into anything actionable. Did I mention that my washer died? How's that for all over the board? Thanks for checking in!
-
Yes Lumpie, i noticed that you were MIA about ten days a little back and wa worried too. Glad your scans are stable!
-
Thanks for the update Lumpie and all you do here!
I googled confidence interval for dummies and I still don't understand what it means. Does anyone happy to have an easy explanation? I wish my local community college had a class on how to interpret medical studies.
from the BRCA study link above...
Results: For both BRCA1 and BRCA2 mutation carriers, none of the smoking-related variables was associated with breast cancer risk, except smoking for more than 5 years before a first full-term pregnancy (FFTP) when compared with parous women who never smoked. For BRCA1 mutation carriers, the HR from retrospective analysis (HRR) was 1.19 [95% confidence interval (CI), 1.02–1.39] and the HR from prospective analysis (HRP) was 1.36 (95% CI, 0.99–1.87). For BRCA2 mutation carriers, smoking for more than 5 years before an FFTP showed an association of a similar magnitude, but the confidence limits were wider (HRR = 1.25; 95% CI, 1.01–1.55 and HRP = 1.30; 95% CI, 0.83–2.01). For both carrier groups, alcohol consumption was not associated with breast cancer risk.
Conclusions: The finding that smoking during the prereproductive years increases breast cancer risk for mutation carriers warrants further investigation.
-
2019whatayear - thanks!
Regarding confidence intervals... as you note, it is a statistics term. I actually took stats not too long ago - but it is hardly my strong suit. Long story short.... and probably over simplified.... if you have a bell curve (not sure if I can insert a pic but it comes right up if you google it), the confidence interval states how confident you are that all relevant values are in the part of the graph where you think they should be. At least for scientific research, the confidence interval is almost always between 95% and 99%. The higher the number, the more confident you are about your results. So with a 95% confidence interval, you are 95% confident that the values fall where expected. For peer reviewed, scientific research, the confidence intervals are going to be very high. 95% or higher. I think I usually see 95%.
When reading high quality, peer reviewed research, I don't get real bogged down in the CI number. It is going to be high and it's not like I am going to (or able to!) re-do the math to confirm it.
I hope that helps.
PS: That's a good tip for your community college or local adult education program...or maybe even a library if they have classes, seminars or talks on topics!
-
Lumpie, so glad to hear you're doing pretty well! I also noticed you hadn't posted something here for a while, but I saw you were active on other boards.
Here's a new tidbit:
Could beta-blockers slow the spread of cancer?
New research from Monash University has suggested that anti-stress drugs, known as beta-blockers, could slow the spread of cancer in the body.
The study, which was published in Clinical Cancer Research, marks the first ever study marking that beta-blockers stop cancer cells spreading through the body in women with breast cancer.
http://www.pharmatimes.com/news/could_beta-blockers_slow_the_spread_of_cancer_1323268
-
Researchers uncover two-drug combo that halts the growth of [HER2] cancer cells
DALLAS - Jan. 23, 2020 - UT Southwestern Simmons Cancer Center researchers have discovered a two-drug combo [everolimus added to neratinib] that halts the growth of cancer cells that carry HER2 mutations.
The findings, published today in the journal Cancer Cell, were prompted by the observation that, after an initial response, patients with cancers harboring HER2 mutations eventually develop resistance to a promising new cancer drug [neratinib] currently in clinical trials...
Sudhan says the combination of neratinib and everolimus worked in cell lines, organoids established from patient-derived tumors, and in mice harboring HER2 mutant tumors. The next step will be testing this two-drug combo in humans.
https://www.eurekalert.org/pub_releases/2020-01/usmc-rut012320.php
-
Insurance Status Helps Explain Racial Disparities in Cancer Diagnosis
From blog of Dr. Francis Collins, Director of the National Institutes of Health:
A new NIH-funded study of more than 175,000 U.S. women diagnosed with breast cancer from 2010-2016 has found that nearly half of the troubling disparity in breast cancer detection can be traced to lack of adequate health insurance. The findings suggest that improving insurance coverage may help to increase early detection and thereby reduce the disproportionate number of breast cancer deaths among minority women.
-
Whew Lumpie, hope you managed to get the washer fixed / replaced? Can’t have you being so smelly we whiff you in Scotland!
It’s a bit of a thing when you are prolific and sound, so folk start to depend on you. That’s also too much and you need to be able to check out and have a breather!
-
Thanks for taking time to explain Lumpie.
I am going to contact my library and suggest a program on how to understand medical news/read medical studies.
:-)
-
Lumpie, you deserve all the breaks you want. We so appreciate you and all the wonderful information shared here.
-
Lumpie, thank you for taking a break when you need to. We sure appreciate all you do here and want you to take good care of yourself.
-
Night Shift Work-A Risk Factor for Breast Cancer
The case-control study was conducted from 2015-2019 in the Łódź region [in Poland]... Even after considering the effect of other possible cancer factors (like high BMI, smoking, early menstruation, late menopause, pregnancy history, age, place of living, education), the odds of developing cancer were twice as high in the group of shift workers (OR = 2.20 (95% CI: 1.57; 3.08)).
https://www.physiciansweekly.com/night-shift-work-a-risk-factor-for-breast-cancer/
-
Magnetized Particles Show Live Metabolic Activity of Breast Cancer
Researchers at Cancer Research UK Cambridge Institute and the Department of Radiology at the University of Cambridge are now reporting in Proceedings of the National Academy of Sciences that they've used magnetized particles to image the actual metabolic activity of breast cancer tumors. This may provide a relatively accessible new way of categorizing tumors, allowing for more accurate decision making during diagnosis and subsequent treatment, saving lives in the process and minimizing unwarranted therapies.
-
Why eating yogurt may help lessen the risk of breast cancer
One of the causes of breast cancer may be inflammation triggered by harmful bacteria suggest researchers. Scientists advise consuming natural yogurt, which contains beneficial bacteria which dampens inflammation and which is similar to the bacteria found in breastfeeding mothers. Their suggestion is that this bacteria is protective because breast feeding reduces the risk of breast cancer. The consumption of yogurt is also associated with a reduction in the risk of breast cancer.
https://www.sciencedaily.com/releases/2020/01/200124073857.htm
-
key being NATURAL yogurt
-
Help me out with a definition of "natural yogurt." How is that different? What makes it "natural?"
-
According to my google it is plain yogurt. No added anything
-
Honestly, I was hesitant to post the yogurt article, because it's just about a paper speculating on the reason *why* yogurt seems to reduce bc risk (published in the journal "Medical Hypotheses"). But articles based on that paper popped up in a lot of places sounding like there was new yogurt evidence (which I did not see) so I posted a link to the article that seemed clearest. If you want to look at potentially relevant yogurt studies, the food for breast cancer site references several: https://foodforbreastcancer.com/foods/low-fat-yogurt.
-
Thanks, whatayear. Plain it is, along with berries and some ground flaxseed for me. Alas, it didn't keep me from getting cancer! Nor did all the other reasons I woulda been pegged as "low risk."
-
I raise a fist in anger on your behalf Mountain Mia! IF only we could return our cancer like a pair of shoes to the store. Yeah, these boobs just didn't work out, I would like to return them and get my clean bill of health back.. tyvm!
-
Single dose of psychedelic drug eased cancer patients' anxiety, depression for years
Nearly five years after a group of cancer patients were given a single dose of a psychedelic drug [psilocybin] to ease depression and anxiety, new research finds that many of them are still feeling the positive effects...
Dr. Stephen Ross, director of addiction psychiatry at New York University's Langone Medical Center who led the 2016 study and co-authored the new research, said the results of the latest study are "mind-boggling."
-
Natural Body Protein Found to Suppress Breast Cancer Metastasis
A protein naturally produced in the body has been found to suppress breast cancer metastasis in animal models of human tumors, according to a research study ("The RNA-binding protein AKAP8 suppresses tumor metastasis by antagonizing EMT-associated alternative splicing") led by a team at Baylor College of Medicine. The team also found that high levels of this protein, AKAP8, predicts a better survival for breast cancer patients. Their work appears in Nature Communications. The findings show that AKAP8 inhibits metastasis by interfering with the production of proteins that promote metastatic behavior in cells and suggest strategies that may help treat metastatic cancer in the future.
https://www.genengnews.com/news/natural-body-protein-found-to-suppress-breast-cancer-metastasis/
-
Novel Drug May Reverse Breast Cancer Hormone Therapy Resistance
SFX-01 – inspired by a natural plant-derived compound called sulforaphane, which was first discovered in cruciferous vegetables such as rocket, broccoli and kale – has recently been shown in a clinical trial to delay the progression of incurable secondary breast cancer in women whose disease has already developed resistance to hormone therapy.
In a new study led by Dr Bruno Simões, Dr Sacha Howell and Professor Rob Clarke at the University of Manchester, researchers investigated the effect of SFX-01 alone, or in combination with tamoxifen or fulvestrant, in patient samples and in mice to understand how the drug works and how it can be best used to treat breast cancer.
They found that SFX-01 reduced the ability of specialized cells called breast cancer stem cells to form tumors in mice, with the drug also reducing the ability of breast cancer cells to form secondary tumors in the mice's lungs. -
A targeted therapy for triple negative breast cancer may lie [in] existing drugs
- Researchers identified two proteins -- mutant tumor protein 53 (mtp53) and poly-ADP-Polymerase (PARP) -- that are present and interacting with DNA during the replication process in [most] patients with triple negative breast cancer.
- Suppressing these proteins through a combination of existing PARP-inhibiting therapies [talazoparib and temozolomide] could be an effective way to interrupt the development of triple negative breast cancer cells and offer the first targeted treatment for this form of the disease.
- The findings may also reclassify triple negative breast cancer as a different form of the disease that can be treated by combining already existing therapies.
https://eurekalert.org/pub_releases/2020-01/asrc-att012920.php
-
I had this technique for my lumpectomy. It was called a savi scout. It was inserted just like a tumor marker during biopsy a day or two before my surgery.
-
The Expression Level of HJURP has an Independent Prognostic Impact and Predicts the Sensitivity to Radiotherapy in Breast Cancer
-
Choice of anesthesia may change metastatic process of breast cancer
Jun Lin, MD, PhD, of the Department of Anesthesiology in the Renaissance School of Medicine at Stony Brook University, and colleagues found that sevoflurane anesthesia leads to more metastatic burden in the lung after breast tumor resecting surgery than propofol in laboratory models.
The study findings may serve as a guide to design clinical trials for clinicians to optimize anesthesia choice for breast cancer surgery in order to achieve best long-term outcomes.
Source:
-
CytoDyn Announces Stunning Results from Clinical Trials Evaluating mTNBC and MBC with Leronlimab and will Request an Emergency Type C Meeting with FDA to Enroll 50 Awaiting Patients with a Serious Solid Tumor Cancer Condition
[BTW, I posted about earlier results a month ago.]
Third patient data supports leronlimab (PRO 140) as a potential treatment option for metastatic triple-negative breast cancer (mTNBC) and metastatic breast cancer (MBC). Patient CTC dropped to zero after 2 weeks of leronlimab treatment, same as the first patient on leronlimab
https://finance.yahoo.com/news/cytodyn-announces-stunning-results-clinical-110010381.html
-
Wow, that last one is a stunner! Something to clearly watch. Thanks much.
-
"Choice of anesthesia may change metastatic process of breast cancer" barely gave any info and what it gave didn't make sense. I wonder if there's an actual article on this somewhere else?
-
Look up ketorolac.... there is a lot of info on it being a good anesthesia choice that discourages mets.
-
You're welcome, BevJen!
thisiknow, the actual study being referenced seems to be here: https://www.nature.com/articles/s41467-019-14065-6
It only seems to be comparing sevoflurane and propofol. It goes into a lot of detail, but...
"In summary, in this report we show that a volatile anesthetic sevoflurane leads to more lung metastasis than an intravenous anesthetic propofol following surgery in two mouse models of spontaneous metastasis."
-
Thanks debbew ...that's just so weird.
-
one quick question on that study does this mean lumpectomies: "after breast tumor resecting surgery" and so then they didn't look at masectomies.
One of my goals this week is to call my Nurse Navigator b/c she is involved w/the cancer related stuff at the hospital (like support groups, etc) and ask her about a how to read medical studies and news class at the hospital. :-)
-
2019whatayear, the study used mouse models... they were resecting tumors in mice! The results might not apply in humans at all (but gives researchers some reason to think it might).
Apparently, the potential effect of anesthesia on long-term outcomes is an active area of research.
Here is a retrospective study done on bc patients a year ago which found no difference in long term outcomes between IV and inhaled anesthesia: https://anesthesiology.pubs.asahq.org/article.aspx?articleid=2712483 But *this* study refers to a previous study from 2016 (https://ekja.org/journal/view.php?doi=10.4097/kjae.2016.69.2.126) that did seem to show a difference between sevoflurane and propofol, but notes that the previous study's sample size was small.
Sorry the results aren't clear yet.
-
Naltrexone for BC? Links to a clinical trial as well as a study in dogs below. Targets estrogen . Have not found mention of positive/negative interaction with other drugs. A friend mentioned that her partner will be using it for early onset alzheimer/dementia. Studies into BC treatment seem to be just starting. The main use so far seems to be for alcohol and opiod addiction.
https://clinicaltrials.gov/ct2/show/NCT00379197
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6171873/
-
psychedelics....... interesting. Suggested reading, Michel Pollan "How to Change Your Mind" https://bioneers.org/how-to-change-your-mind-a-review-of-michael-pollans-latest-book-about-psychedelics-zmbz1805/ . These were being researched fairly intensively until tune in, tune out ,drop out, became the rage. Lots of interesting information in Pollan's book. Research seems to be starting up again .
-
If one acid trip can stop years of cancer anxiety- sign me up! Debbew re: the anesthetic study thanks for the clarification- I guess it is what it is since I already had surgery.
-
I wouldn't count on LSD to reduce anxiety. It might for some but it could go in the complete opposite direction for others. There are just too many variables to take into consideration.
I would suggest seeing what you can find out about using low-dose psilocybin for cancer patients
-
Discovering the anticancer potential of non-oncology drugs by systematic viability profiling
-
Hi, I have joined this forum in the hope of sharing our experience...and your post seemed to be one of the only ones that references the circumstances surrounding my mother's passing...My name is Robyn, I reside in Australia. This post is difficult to write, however my sister and I feel it would have been valuable information to us if we had it late last year. Our gorgeous mother was diagnosed with Stage IV mets that had spread to her bones, Aug 2019. Completely out of the blue. We were advised that once the initial rounds of radio were complete a regime of Kisqali/Ribociclib would enable a diagnosis of 10 years. Only 10 weeks later mum was transferred from rehab to emergency then ICU with sudden onset of lung inflammation in both lungs. After 12 days, we had to make the devastating decision to turn of life support. 4 days later, whilst researching Kisqali/Ribociclib we happened upon an FDA warning directly identifying sudden lung inflammation as a side effect of this drug, and as such patients should have their lungs monitored. Our mother began Kisqali/Ribociclib on Sept 19 2019, 3 days after her 70th birthday. This FDA warning was released on September 13 2019. Our mother was an otherwise healthy woman, with a rich and loving life ahead, she did everything she could in ICU to give herself a chance, "i want to get better" was her anthem between oxygen masks. Eventually mum was intubated whilst her ICU and Infectious disease specialists tested for all possible types of infection/diseases/pneumonia possible. We have lodged documents with Novartis and they are requesting follow up. In no way do we want to deter women from this treatment, we were so happy mum had this option, Kisqali/Ribociclib would have let her and her children and grandchildren say hello each day and goodbye on our own terms if we had the chance. We only think it should be a safe playing ground and so have decided to share this information. we also believe it should be a fare playing ground and are at a loss as to why these alerts are not sent out globally, given they are used globally. We are heart broken, we are completely devastated as she was everything to us. Nothing can be done to bring mum back but we so do not wish upon anyone else. Just ask the question, is all.
-
Robyn and sister, My condolences the loss of your mother and thank you for sharing.
-
Yes--Robyn and sister thank you for sharing that with this group and my deepest sympathies on the loss of your mother.
-
By combining Herceptin and Tykerb treatments in 66 women with HER2-positive breast cancer before surgery and comparing the results to 191 similar women who were either treated with just one of the drugs or neither of them, 7 of the 66 women showed no trace of their tumors afterward. Another 11 of them showed considerable shrinkage of their tumors.
-
Not breast cancer, but this was posted recently on a Facebook cancer group I am in. It was interesting the negative effect of hyaluronic acid on myeloma. . . as hyaluronic acid is in many, many cosmetics. . . for it's plumping effect. . even cosmetic brands considered a bit "healthier" like Aveda use it. . .
-
RobynKH , deepest sympthies for the loss of your mother. The more we share, the more learned
-
How some states are taking unusual action to lower prescription drug prices
-
In terms of state laws, a new law in PA requires insurance companies to cover approved cancer drugs prescribed for metastatic patients (rather than forcing a "fail first" with cheaper drugs):
(notes that "Legislatures in Georgia, Illinois, and Maryland have passed similar legislation in recent years.")
-
Robots steady breast cancer surgeon's hands in first human trial
Writing in Nature Communications, researchers in Maastricht and at Eindhoven University of Technology describe a pilot trial in which a specialist surgeon used the robot to re-route lymphatic vessels around women's scar tissue. The surgeon operated on 20 women and used the robot in eight of those procedures.
-
debbew: thanks for all your interesting posts!
lumpie: we are thinking of you & sending you well wishes
-
Bell Ringing Not So Joyous for Cancer Patients?
Greater treatment-related distress for those who rang bell at end of treatment
-
Really interesting about the bell. Since I don't care for the image of cancer as a "battle" or a "war", I was less than pleased with a "conquering hero" victory celebration. I did the necessary treatment. A quiet glass of wine would have been nice.
-
Not a breast cancer cure, but who knows what this sort of treatment may contribute to management of side effects etc......
Breakthrough trials explore the link between immune cells in our gut and brain... So could a matchbox-sized electrical implant end the misery of diabetes, asthma AND arthritis?
-
yw, santa, glad you found them interesting!
I'll add my thanks to marijen and mystical and all the others who post and comment, but especially Lumpie for starting and really running this thread (hope things are going well!).
-
Cancer and Metabolic Disorders Linked with Testosterone Levels in Both Sexes, but with Differences
Additionally, they found that genetically higher testosterone levels increased the risks of breast and endometrial cancers in women, and of prostate cancer in men. "MR analyses indicated that testosterone increases prostate cancer risk in men … We found evidence that testosterone increased the risk of estrogen receptor (ER)-positive but not ER-negative breast cancer … There was also evidence for a protective effect of SHBG [sex-hormone binding globulin] on risk of endometrial cancer in women, which was consistent across all models, but a risk-increasing effect of SHBG on ER [estrogen receptor]-negative breast cancer."
-
I just don’t understand why it took them so long to figure out the testosterone thing. It’s included with the HRT treatment for menopause. At least what I was given.
-
My TNBC was 90% AR+....
-
Dark Chocolate Intake Acutely Enhances Neutrophil Count in Peripheral Venous Blood
Beside the well-established impact on decreasing the risk of cardiovascular diseases (1), recent attention has been paid to the relationship between cocoa-containing foods and the immune system (2), showing that dark chocolate consumption enhances the systemic defense against bacterial (3) and viral (4) infections. Hence, the current study aimed at investigating the acute effect of dark chocolate intake on peripheral blood leukocytes.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC58353...
Iran J Pathol. 2017 Summer; 12(3): 311–312.
PMCID: PMC5835384
PMID: 29531561
{Any excused for chocolate!}
-
Add-On Keytruda Doubles pCR Rate in Early Breast Cancer
Rate of complete response reached 60% in triple-negative cohort
Escalating preoperative systemic therapy with immunotherapy improved pathologic complete response (pCR) rates for women with high-risk early breast cancer, results of a phase II trial showed.
Among 240 women with stage II/III breast cancer and HER2-negative disease, those assigned to neoadjuvant chemotherapy plus pembrolizumab (Keytruda) achieved a pCR rate of 44%, as compared with 17% for a control group on chemotherapy alone, reported Rita Nanda, MD, of the University of Chicago, and colleagues.
Patients with triple-negative disease in the so-called I-SPY2 trial had pCR rates of 60% with pembrolizumab, a PD-1-directed checkpoint inhibitor, and 22% without it. While those with hormone receptor (HR)-positive/HER2-negative disease had rates of 30% versus 13%, respectively, as described in JAMA Oncology.
-
Q & A: How Corrupt Scientists Threaten Public Health
David Michaels, a GW professor and former Obama administration official, talks about his new book and how manufactured studies harm consumers.
https://gwtoday.gwu.edu/q-how-corrupt-scientists-t...
{This is more about public health than cancer specifically, but it is interesting - and troubling in an environment in which many are uncertain about what science to trust.}
-
Anybody out there go back to your old treatments and if so did you get positive results ?
-
Kimchee,
I repeated taxotere after about 18 months. Worked like a charm. Got a near PCR (again). Taxanes seem to be very effective for my type of cancer: HER2+, hormone negative. I remained on H&P which worked for about 14 months.
-
I'm Er+Pr+ Her2- was on piqray and stopped working , Dr. wants me to go back to old treatments . Thank you for your reply so fast . I'm so glad to have found this site .
-
taxol worked for me after 7 years.
-
Interesting data for those on CDK4-6 inhibitors. The authors investigated enzyme Thymidinkinase (unspecific tumour marker) and could predict the response (developing resistance or sensitivity).http
 /clincancerres.aacrjournals.org/content/early/2020/01/14/1078-0432.CCR-19-3271.full-text.pdf
/clincancerres.aacrjournals.org/content/early/2020/01/14/1078-0432.CCR-19-3271.full-text.pdf -
Hi Santabarbian, Ketrolac is a NSAID sometimes used during or after surgery. Not really anesthesia
-
Strontium89 Now Available for Relief of Metastatic Bone Pain
-
nice to see you back Lumpie! But good that you had a break too
-
Welcome back Lumpie and thanks for all you do!
-
So good to see you back Lumpie! Thank you for this thread and all you do!!
-
Why biometrics are the future of patient care
"We have seen an increased investment in biometrics by our healthcare customers as a way to accurately identify people in their ecosystems, including patients and clinicians, maintain secure access to protected health information, and secure high-risk work flows such as electronic prescribing for controlled substances,"
...healthcare organizations are using biometric tools for two-factor or multi-factor identification and single sign-in for staff and patient identification.
"Some providers or patients may be concerned that the government will get access to their information....
it was important to develop on "elevator speech" for staff to explain to patients how the technology would be used and data would be stored.
"A lot of our staff training was educating them on how to speak to a patient about the technology....
https://www.medicaleconomics.com/news/why-biometri...
{Thanks for all the kind comments. I have had a lot going on and have had to put myself on an internet "diet." It's brutal!}
-
De Novo Versus Recurrent HER2-Positive Metastatic Breast Cancer: Patient Characteristics, Treatment, and Survival from the SystHERs Registry
Limited data exist describing real-world treatment of de novo and recurrent HER2-positive metastatic breast cancer (MBC). The Systemic Therapies for HER2-Positive Metastatic Breast Cancer Study (SystHERs) was a fully enrolled (2012-2016), observational, prospective registry of patients with HER2-positive MBC. Patients aged ≥18 years and ≤6 months from HER2-positive MBC diagnosis were treated and assessed per their physician's standard practice. The primary endpoint was to characterize treatment patterns by de novo versus recurrent MBC status, compared descriptively. Secondary endpoints included patient characteristics, progression-free and overall survival, and patient-reported outcomes.
Patients with de novo versus recurrent HER2-positive MBC exhibit different disease characteristics and survival durations, suggesting these groups have distinct outcomes.
Clinical trial identification number NCT01615068 (clinicaltrials.gov).
https://www.meta.org/papers/de-novo-versus-recurre...
DOI: 10.1634/theoncologist.2019-0446
https://theoncologist.onlinelibrary.wiley.com/doi/...
-
Antitumor Activity and Safety of Trastuzumab Deruxtecan in Patients With HER2-Low-Expressing Advanced Breast Cancer: Results From a Phase Ib Study
Trastuzumab deruxtecan (T-DXd, formerly DS-8201a) is a novel human epidermal growth factor receptor 2 (HER2)-targeted antibody drug conjugate (ADC) with a topoisomerase I inhibitor payload. A dose escalation and expansion phase I study evaluated the safety and activity of T-DXd in patients with advanced HER2-expressing/mutated solid tumors.
Here, results for T-DXd at the recommended doses for expansion (RDE) in patients with HER2-low (immunohistochemistry [IHC] 1+ or IHC 2+/in situ hybridization-) breast cancer (ClinicalTrials.gov identifier: NCT02564900) are reported.
The novel HER2-targeted ADC, T-DXd, demonstrated promising preliminary antitumor activity in patients with HER2-low breast cancer. Most toxicities were GI or hematologic in nature. ILD (interstitial lung disease/pneumonitis) is an important identified risk and should be monitored closely and proactively managed.
https://www.meta.org/papers/antitumor-activity-and...
DOI: 10.1200/jco.19.02318
https://ascopubs.org/doi/10.1200/JCO.19.02318
-
Molecular heterogeneity in breast carcinoma cells with increased invasive capacities
Background Metastatic progression of breast cancer is still a challenge in clinical oncology. Therefore, an elucidation how carcinoma cells belonging to different breast cancer subtypes realize their metastatic capacities is needed. The aim of this study was to elucidate a similarity of activated molecular pathways underlying an enhancement of invasiveness of carcinoma cells belonging to different breast carcinoma subtypes.
Conclusions: We can conclude that hormone receptor-positive cells with increased invasiveness acquire the molecular characteristics of triple-negative breast cancer cells, whereas Her2-positive INV cells specifically changed their own molecular phenotype with very limited partaking in the involved pathways found in the MDA-MB-231-INV and T47D-INV cells. Since hormone receptor-positive invasive cells share their molecular properties with triple-negative breast cancer cells, we assume that these types of metastatic disease can be treated rather equally with an option to add anti-hormonal agents. In contrast, Her2-positive metastasis should be carefully evaluated for more effective therapeutic approaches which are distinct from the triple-negative and hormone-positive metastatic breast cancers.
https://www.meta.org/papers/molecular-heterogeneit...
https://content.sciendo.com/view/journals/raon/ahe...
-
GREELEY, Colo. (CBS4) – A team of scientists at the University of Northern Colorado believe venom from venomous snakes could carry the cure to cancer. Dr. Stephen Mackessy, professor at UNC's School of Biology, says studies show venoms in different snakes can attack human cancer cells in unique ways.

To conduct the study, Mackessy's students are given access to hundreds of snakes from around the world, all of which are stored in a secured facility on the campus of UNC. From rattlesnakes to vipers, the students are able to extract venom from each snake to study the compounds and proteins.
"These are compounds that have evolved to kill other animals, and kill things … in general, wreak havoc with living systems," Mackessy told CBS4's Dillon Thomas. "It turns out they are actually a very logical place to look for therapeutics."
Mackessy said that when sharing his studies with the public, many times people automatically think of the dangers venomous snakes come with. However, most don't consider the benefits the reptiles can offer to humans.
"People tend to have a visceral reaction to snakes in general," Mackessy said.

Snake venoms have been used since the 1950s to treat things like high blood pressure in millions of people around the globe. However, Mackessy said his lab is one of the first to research the possible uses of venom compounds to battle various forms of cancer.
"When you think about looking for a therapeutic drug, you don't turn first to something like a venom or toxin as a source," Mackessy said.
PhD candidate Tanner Harvey has specifically been researching viper venoms, some of which come from habitats as close as southern Arizona. Each venom, in different doses, reacts to cancers uniquely.
"(One viper venom) kills breast cancer really quickly at low doses. And, it kills colon cancer at low doses. But, it doesn't kill melanoma," Harvey said.
However, other venoms strongly react to melanoma.
Killing the cancer with venom isn't hard. It's not killing the patient at the same time that's the challenge. The team at UNC said their challenge is finding which compounds can be combined with other remedies to kill cancer efficiently, while preserving other life-dependent cells.
"(Finding the proper doses and mixes) is just like panning for gold," Harvey said.
The study is still in preliminary phases. Once the team feels they have a solid answer to which venom compounds are safe to battle cancer with, the research would press on to one day potentially meet clinical studies.

When asked if students at UNC were capable of finding the cure to cancers, Mackessy said they were well on their way toward that direction.
"There is no question they have the ability to make that kind of contribution," Mackessy said.
While Mackessy's team is working toward the goal of curing cancers, another takeaway from their research was also offered. Both Mackessy and Harvey hope their research will encourage the public to stop senselessly killing snakes simply out of fear. While both said they understood human instinct to fear a snake's ability to take life, they hoped the public would ultimately come to value the snake's ability to preserve life at the same time.
"You never really know what is going to come from a natural source, even something like a rattlesnake," Mackessy said. "It may be, in fact, that these dangerous animals house in their venom something that one day may be lifesaving for you, or your family members."
-
that seems pretty logical taxol is derived from a plant - maybe future “chemo” could come from venom.
-
Using ctDNA to Predict Relapse in Patients With Early-Stage Breast Cancer
- Interview by
- Farzanna S Haffizulla MD, FACP, FAMWA
- Interview with
- Ben Ho Park MD, PhD
- So, we'd like to talk about circulating tumor DNA today. Can you tell us how reliable modern technology is in identifying ctDNA?
- Can you tell me about then early-stage breast cancer and some challenges perhaps in identifying ctDNA in this patient population?
- Do you think that we can look at circulating tumor DNA as a potential biomarker perhaps for early-stage breast cancer patients?
- https://www.practiceupdate.com/C/94149/56?elsca1=e...
- @{Interview addresses these and other questions. Video and transcription provided. Video is @ 3.5 minutes long. If log in is required, it is free.}
- {Yikes... those snakes...! (in the post above)}
-
Immune cell which kills most cancers discovered by accident by British scientists in major breakthrough
20 Jan 2020 The Telegraph
A new type of immune cell which kills most cancers has been discovered by accident by British scientists, in a finding which could herald a major breakthrough in treatment.
Researchers at Cardiff University were analysing blood from a bank in Wales, looking for immune cells that could fight bacteria, when they found an entirely new type of T-cell.
That new immune cell carries a never-before-seen receptor which acts like a grappling hook, latching on to most human cancers, while ignoring healthy cells.
"Our finding raises the prospect of a 'one-size-fits-all' cancer treatment, a single type of T-cell that could be capable of destroying many different types of cancers across the population. Previously nobody believed this could be possible."
The research was published in the journal Nature Immunology.
https://www.msn.com/en-gb/news/uknews/immune-cell-...
-
Hippocampal Avoidance During Whole-Brain Radiotherapy Plus Memantine for Patients With Brain Metastases
- Journal of Clinical Oncology
- The authors of this phase III randomized trial studied hippocampal avoidance using intensity-modulated radiotherapy during whole-brain radiotherapy with memantine and compared that approach with WBRT with memantine in 518 randomly assigned patients with brain metastases. The most common primary sites of malignancy were breast and lung. The risk of cognitive function failure was significantly lower in the hippocampal-avoidance arm (aHR, 0.74; P = .02), and this was primarily due to less deterioration in executive function at 4 months and learning and memory at 6 months. There was no significant difference in overall survival or intracranial progression-free survival between the two groups.
- These results support hippocampal avoidance as the standard of care in this patient population.
doi: 10.1200/JCO.19.02767. -
Not surprising...
Higher case numbers correlated with better results in breast cancer surgery
[A study in Germany showed that] a positive correlation exists between the volume of services provided and the quality of treatment results in the surgical treatment of primary breast cancer: In hospitals with larger case numbers and with medical teams who perform many breast cancer operations, the overall survival chances are higher for breast cancer patients who underwent surgery. In addition, further surgery on the operated breast is less common.
-
Also not surprising...
Certain factors linked with discontinuing breast cancer [anti-hormonal] therapy
In the study of 1,231 women who completed questionnaires, 59% reported at least one barrier to adhering to endocrine therapy. Three factors were identified as important: habit (challenges developing medication-taking behavior), tradeoffs (perceived side effects and medication safety concerns), and resource barriers (challenges related to cost or accessibility).
-
The article about ringing the bell was fascinating. It made me think that while cancer is sneaky, maybe the brain is tricky in how it processes all the treatment andthe associated events.
-
Shannen Doherty's Stage IV Breast Cancer
— "Beverly Hills, 90210" star
In an ABC News interview, actress Shannen Doherty told Amy Robach (herself a breast cancer survivor) that her breast cancer has returned and that it is now stage IV. The 48-year-old actress is best known for her roles in the original "Beverly Hills, 90210" and "Charmed."
https://www.medpagetoday.com/blogs/celebritydiagno...
ABC interview:
{This is sad news. Perhaps a silver lining will be added attention to and awareness of MBC.)
-
marijen - loved those snake pictures!!! I wonder if some types of venom would be better than others. So would doses be givne in IVs or bites? Maybe a pill. And are they wearing protective gear when milking the snake.
-
I am guessing a formulation by injection. Unfortunately it will take more research and testing.
-
If Only That Phase III Oncology Trial Had Been Designed Differently
The cancer treatment community's ultimate perception of a successfully completed phase III randomized trial depends in large part on how well the trial was conceived and structured....the question it poses must be relevant to ensure interest by clinical investigators, referring clinicians, and potential research subjects. Further, the initiative must have adequate funding for data collection and analysis, translational laboratory investigations, and other trial components. {There is a} risk that study results may lead investigators and others to question the study's design in retrospect.
...the goal {in writing this} has been to emphasize both the critical relevance of very careful consideration of the impact of trial design on the interpretation of possible study results and the legitimate risk that individual trials, no matter how meaningful or even "positive" their outcomes may be, may raise as many clinically relevant questions as they answer.
https://www.onclive.com/publications/Oncology-live...
{An interesting perspective, especially for those in or considering clinical trials.}
-
Homing in on Targeted Treatment Strategies in Breast Cancer
The fields of early-stage hormone receptor (HR)–positive and metastatic HER2-positive breast cancer have made great strides in recent years, said Neelima Denduluri, MD, and such progress could be attributed to the emergence of tailored treatment strategies and the use of HER2-directed agents, respectively.
OncLive: How are you approaching treatment in patients with early-stage HR-positive, HER2-negative breast cancer?
Could you discuss the use of genomic assays in practice?
Could you discuss some of the key studies that were presented at the 2019 San Antonio Breast Cancer Symposium?
...anything else ...?
https://www.onclive.com/web-exclusives/homing-in-o...
{Dr. Denduluri shares insight on treatment, advances, etc. An accessible commentary on treatments advances and options.}
-
Agnes Dumas, PhD, on the Impact of Breast Cancer Treatment on Employment
Two years post-diagnosis, 21% of patients had not returned to work, study shows
The adverse effects of breast cancer treatment are known to often prevent patients from going back to work -- leading to negative economic as well as psychological consequences. French researchers recently analyzed a prospective cohort of more than 1,800 patients with stages I-III breast cancer who were employed prior to their diagnosis, showing that 2 years after diagnosis, 21% had not returned to work. The odds of not returning were significantly increased among those treated with combinations of chemotherapy and trastuzumab, and other significant factors included arm morbidity and depression.
This is an important study not just for physicians but also for society as a whole, which identifies the vulnerable members in hopes of changing policies to better support them through different strategies.
{Two Medpage articles:}
-
“City of Hope scientists have identified an unlikely way to potentially prevent or slow the progression of aggressive breast cancer: target one's internal clock.
Often taken for granted, the circadian rhythm is gaining traction as a potential catalyst or brake for the onset of disease. For example, studies have shown that women who take frequent night shifts have disrupted internal clocks and increased risk of developing breast cancer. Now, City of Hope's David K. Ann, Ph.D., and his colleagues think they may have found a new role for the "clock gene": It is linked to triple-negative breast cancer, an aggressive form of the disease that often results in a poorer prognosis.“
https://www.cityofhope.org/breakthroughs/internal-clock-key-to-slowing-cancer -
The Impact of Dietary Supplement Use on Survival Outcomes in Breast Cancer
- Journal of Clinical Oncology In this observational correlative study, the authors evaluated the impact of dietary supplements during cancer treatment in 1134 patients with metastatic breast cancer queried at registration and during treatment in a randomized phase III trial of chemotherapy treatment schedules.
- The authors found a signal of potential negative impact in terms of recurrence and overall survival with the use of antioxidants, iron, and vitamin B12 during chemotherapy. Multivitamin use was not associated with survival outcomes.
- CONCLUSION
Associations between survival outcomes and use of antioxidant and
other dietary supplements both before and during chemotherapy are
consistent with recommendations for caution among patients when
considering the use of supplements, other than a multivitamin, during
chemotherapy.
doi/10.1200/JCO.19.01203 -
Chemotherapy for Cancer Treatment Could Be Unviable Because of Antibiotic-Resistant Superbugs, Doctors Fear
British oncologists fear antibiotic-resistant superbugs may someday make chemotherapy an unviable treatment option for their cancer patients. (Newsweek)
An estimated one in five cancer patients need antibiotics during their treatment, according to existing research cited by the authors of the report, and cancers including multiple myeloma and acute leukaemia can't be treated without them.The survey revealed that 46 percent of doctors believe drug-resistant bugs will make chemotherapy unviable.
...since we know chemotherapy suppresses the immune system, leaving patients vulnerable to infections...
86 percent of the doctors said the bugs Staphylococcus, E. coli and pseudomona put cancer patients at the most risk of serious harm.
"Oncologists are right to be concerned about growing levels of antibiotic resistance being experienced by their patients post-surgery or those undergoing chemotherapy.
-
'Breakthrough' in Fertility Preservation for Breast Cancer Patient
First successful case using eggs frozen after in vitro maturation
French physicians on Wednesday described the first case of an infertile cancer patient giving birth after her immature eggs were further matured via in vitro maturation (IVM) and subsequently frozen.
"IVM enables us to freeze eggs or embryos in urgent situations or when it would be hazardous for the patient to undergo ovarian stimulation. In addition, using them is not associated with a risk of cancer recurrence."
"...for the average patient, experimental advances in precision medicine should be taken with caution, given that we don't have enough data at this time,"
-
Thanks Lumpie for the supplement article-my MO was smart enough to tell me to stop antioxidants and other supplements during chemo, and I'm glad she did.
Claire in AZ
-
Mayo researchers recommend all women with breast cancer diagnosis under age 66 be offered genetic testing
A study by researchers at Mayo Clinic published this week in the Journal of Clinical Oncology suggests that all women with a breast cancer diagnosis under the age of 66 be offered germline genetic testing to determine if they have a gene mutation known to increase the risk of developing other cancers and cancers among blood relatives. Current guidelines from the National Comprehensive Cancer Network (NCCN) recommend germline testing for all women diagnosed with breast cancer under the age of 46 regardless of their family history and breast cancer subtype.
https://medicalxpress.com/news/2020-02-mayo-women-breast-cancer-diagnosis.html
-
Mammograms not helpful in women 75 and older, study finds
Although studies clearly show mammograms starting at age 50 prevent breast cancer deaths, until now, doctors have had little evidence about when to end screening, Dr. Otis Brawley of Johns Hopkins University and former chief medical officer of the American Cancer Society, wrote in editorial in the Annals of Internal Medicine.
"The study is important because a third of all American women die of breast cancer are diagnosed after the age of 70," Brawley said in a telephone interview.
The U.S. Preventive Services Task Force, which sets screening guidelines, currently states that the evidence is insufficient to assess the harms and benefits in women 75 and older. Recommendations by other groups vary.
https://news.yahoo.com/mammograms-not-helpful-women-75-220427892.html
-
As a women diagnosed at age 77 due to a mammogram, with a nonpalpable tumor near the chest wall and grade three, I cannot help but wonder where that cancer would be now (lung, through the skin, bones) without that post age 75 mammogram! As my PCP says, that is herd mentality and he prefers to treat on an individual basis.
-
Pertuzumab (P) + trastuzumab (T) with or without chemotherapy both followed by T-DM1 in case of progression in patients with HER2-positive metastatic breast cancer (MBC) - The PERNETTA trial (SAKK 22/10), a randomized open label phase II study (SAKK, UNICANCER, BOOG)
Background: We assumed that a strategy with dual blockade of T+P without chemotherapy followed by T-DM1 at progression might be similarly effective in terms of overall survival (OS), but less toxic resulting in better Quality of Life (QoL) in pts with HER2+ MBC. Updated efficacy results by hormone receptor (HR) status and QoL data are given.
Conclusions: Despite shorter 1st line PFS, OS at 2 years was not affected for P+T alone followed by T-DM1. Side-effects were less frequently seen in the chemotherapy-free arm, although QoL was similar during 1st line in both arms.
Methods: Pts with centrally confirmed HER2+ MBC were randomized 1:1 to receive either P+T alone (arm A) or P+T combined with weekly paclitaxel or vinorelbine (arm
") , followed by maintenance treatment with T+P until progression. After progression, T-DM1 was given as 2nd line therapy in both arms. The primary endpoint was OS at 24 months (mo), among secondary endpoints progression free survival (PFS) was included. QoL was assessed every 3 mo up to 24 mo during 1st line by the NFBSI-16 (summary score and subscale scores for disease-related symptoms, treatment side-effects, function/well-being). Two single items assessed treatment burden and coping.
, followed by maintenance treatment with T+P until progression. After progression, T-DM1 was given as 2nd line therapy in both arms. The primary endpoint was OS at 24 months (mo), among secondary endpoints progression free survival (PFS) was included. QoL was assessed every 3 mo up to 24 mo during 1st line by the NFBSI-16 (summary score and subscale scores for disease-related symptoms, treatment side-effects, function/well-being). Two single items assessed treatment burden and coping.Results: Between 05/13 and 01/16, 210 pts were enrolled. Median age was 58 years, 63% of pts had lung or liver metastases, 36% of tumors were HR-, paclitaxel/vinorelbine was given in 46/59 pts. Efficacy results are shown in table. No difference in OS was observed. HR status did not affect PFS for 1st line. During 1st line, changes from baseline showed small improvements in QoL (NFBSI-16 summary scores) in arm A, while QoL scores remained stable in arm B. Patients in arm B reported more treatment burden during the first 6 months, but not thereafter, while coping improved clinically relevant in both arms.
Annals of Oncology : Official Journal of the European Society for Medical Oncology 2019
https://www.meta.org/papers/pertuzumab-p--trastuzu...
https://www.annalsofoncology.org/article/S0923-753...(19)30418-1/fulltext
DOI: https://doi.org/10.1093/annonc/mdz100.001
-
Trastuzumab Deruxtecan With Nivolumab in Advanced Breast Cancer
— Charles Shapiro, MD, on new study building off drug's recent approval
The FDA recently announced approval of fam-trastuzumab deruxtecan (Enhertu) for the later-line treatment of unresectable or metastatic HER2-positive breast cancer. Investigators at Mount Sinai Hospital, led by Charles L. Shapiro, MD, are now testing the safety and efficacy of this new agent in combination with an anti-PD1 checkpoint inhibitor, nivolumab (Opdivo).
Shapiro discusses both the DESTINY-Breast01 results and his current study.
https://www.medpagetoday.com/meetingcoverage/sabcs...
{Brief video.}
-
The art of innovation: clinical development of trastuzumab deruxtecan and redefining how antibody-drug conjugates target HER2-positive cancers
Annals of Oncology : Official Journal of the European Society for Medical Oncology 2020
A systematic evaluation of all identifiable shortcomings of previous Antibody-drug conjugate (ADC) designs led the team... to create the proprietary linker and payload technology with seven key attributes. {Critical features}, combined with the short half-life of DXd in vivo, limits systemic exposure of the payload, with the aim of reducing toxicity. {The authors suggest that} innovative advantages ... may allow for further customization of the ADC development process.
Conclusion
The promising efficacy of T-DXd across HER2-expressing tumors, along with its potential broad scope of indications and rapid development, led DS to invest in clinical development capabilities, scaling development functions to support an ambitious development program. A comprehensive review of the potential of T-DXd and the organizational model of DS revealed that entering into a collaboration would serve the dual objectives of accelerating and expanding clinical development of T-DXd. With the objective of bringing T-DXd to more patients faster, DS entered into an equal co-development and commercialization collaboration with AstraZeneca in March 2019, with the goal of combining DS's scientific and technological excellence with AstraZeneca's global experience and resources in oncology to efficiently advance the development of T-DXd in HER2-expressing cancers.https://www.meta.org/papers/the-art-of-innovation-...
https://www.annalsofoncology.org/article/S0923-753...(19)43225-0/fulltext
DOI: https://doi.org/10.1016/j.annonc.2019.11.019
{A rather technical discussion of trastuzumab deruxtecan, the mechanisms which have made it a successful therapy, prospects for development of variants in the future and movement of the drug to market.}
-
Progress in Breast Cancer: 'What Would Bill Think?'
— At SABCS, the McGuire Award recipient asked what the late pioneer might have thought of the newest research advancements
At the recent San Antonio Breast Cancer Symposium (SABCS), Joseph A. Sparano, MD, received the William L. McGuire Memorial Lecture Award for his leadership, collaboration, and practice-changing achievements in breast cancer research. Sparano is the study chair of the landmark TAILORx study, the largest ever breast cancer treatment trial, and in his talk he discussed his study -- and how McGuire might have viewed the work.
https://www.medpagetoday.com/meetingcoverage/sabcs...
@{Video discussion of encouraging advances in treatment. @ 5 minutes long.}
-
Genomic Analysis Reveals That Immune Function Genes Are Strongly Linked to Clinical Outcome in the North Central Cancer Treatment Group N9831 Adjuvant Trastuzumab Trial
Purpose
To develop a genomic signature that predicts benefit from trastuzumab in human epidermal growth factor receptor 2–positive breast cancer.
Results {abbreviated}
Immune gene enrichment was linked to increased RFS in arms B and C, whereas arm B and C patients who did not exhibit immune gene enrichment did not benefit from trastuzumab.
Conclusion
Increased expression of a subset of immune function genes may provide a means of predicting benefit from adjuvant trastuzumab.
https://ascopubs.org/doi/full/10.1200/JCO.2014.57....
DOI: 10.1200/JCO.2014.57.6298 Journal of Clinical Oncology 33, no. 7 (March 01, 2015) 701-708.
Published online January 20, 2015.
{This article has some age on it but it an interesting topic which I have not seen discussed elsewhere.}
-
Prospective Decision Analysis Study of Clinical Genomic Testing in Metastatic Breast Cancer
Purpose: To evaluate the impact of targeted DNA sequencing on selection of cancer therapy for patients with metastatic breast cancer (MBC).
Conclusion: In this prospective study, genomic profiling of tumors in patients with MBC frequently identified potential treatments and resulted in treatment change in a minority of patients. Patients whose therapy was not changed on the basis of genomic testing seemed to have a decrease in confidence of treatment success.
"...suggests a need to better understand barriers to implementation of mutation-directed therapy as well as a need for improved understanding of patient perception of somatic genomic testing."
https://www.medscape.com/viewarticle/924847?src=wn...
JCO Precis Oncol. 2019;3
https://ascopubs.org/doi/abs/10.1200/PO.19.00090
DOI: 10.1200/PO.19.00090 JCO Precision Oncology - published online November 18, 2019
{Discusses some benefits and challenges of personalized medicine.}
-
For those who may be interested in advocating around breast cancer and healthcare related issues, I have set up a new thread. You can find it here:
https://community.breastcancer.org/forum/110/topic...
Thanks.
-
Study warns drinking [cow] milk may drastically increase breast cancer risk
The study was recently published in the International Journal of Epidemiology; it evaluated the potential breast cancer risk associated with drinking dairy milk and soy milk. The results call current US Dietary guidelines into question — the public is advised to drink three cups of milk daily, but as little as 1/4 to 1/3-cup of daily cow milk was found to increase breast cancer risk by 30-percent...
The study's first author Gary E. Fraser explained, 'By drinking up to one cup [of cow milk] per day, the associated risk went up to 50%, and for those drinking two to three cups per day, the risk increased further to 70% to 80%.'
-
okay so if the average woman has a risk of 12 percent than a glass of milk could increase risk 30 percent would mean 4 percent additional risk -correct?
I have not been running around drinking glasses of milk since I was like 10. :-) If anyone is looking for a good milk sub -Silk Oat Yeah! Is delicious
-
For years now, I have only had organic milk. It irritates my husband, because it is more expensive, but I feel that it's a better option. Not crazy about other "milks," and I only use it in my coffee and occasionally in either cooking or in cereal.
-
Super skeptical about the "milk and increase in b.c. risk" study. Here's one comment at the bottom: (paid for and conducted by a borderline religious cult that doesn't believe in science nor eating or drinking animal products. I'm sure that didn't impact their findings though
); it was provided by a .com website that I've never heard of before (like Science Daily). I'll wait till Mayo, or Sloan Ketterling, or Science Daily releases the same findings and endorses them.I, however, haven't drank cow's milk in decades. No need to once you're a grown up. We were sold a bill of goods by the dairy lobby in the early 20c century to sell their product--"everybody needs milk", which isn't true, and we've been drinking the "kool-milk" message ever since
-
Oy. I've recently been thinking about my dairy intake. I'm starting with trying to drink my tea and coffee black. Still have some cheese (although allegedly that has no negative impact??) but cutting back a bit on that too. I also get a little sad reading about the beef/dairy industry. Those poor cows. I dunno. . . I've been in a mood lately that there's nothing that I enjoy eating/drinking that isn't bad for me, or for the environment (which non-dairy milk is it that's killing bees??). (Also recently read some research on eggs--that > 5/week is bad for us. What ever.)
-
Dairy Milk or Plant Milk....... It is so hard to find consistent information on nutrition. Very contentious. Interesting article in Consumers Report on plant milk. They do not have an opinion on cow vs plan, but advise, read the label. They are not all the same. They may or may not add vitamins, minerals, protein, and add at different amounts. Sweeteners - generally something to avoid. For years I've heard that soy (as food, not supplements) is ok for ER+ BC, but now that is being questioned. Many advocate cutting back on dairy and meat. I've eaten/drunk dairy my entire life. Does it contribute to my BC?
https://www.breastcancer.org/research-news/soy-may-turn-on-genes-linked-to-cancer
https://www.breastcancer.org/research-news/soy-may-offer-benefits-for-hr-neg-disease
https://www.consumerreports.org/plant-milk/are-plant-milks-more-healthful-than-cows-milk/
-
Had a great appt with my MO this week and I asked him about several topics that have come up in the articles mentioned on this board ...
— if no heart damage was detected after chemo, would/could damage occur later? Answer - yes but it is very very rare.
--does chemo affect the structure of our brain icells i.e. are we stuck with that forever? Answer - both chemo and AIs do affect brain cells but studies show that over time we go back to baseline.
—The newest drugs developed for stage 4 patients are showing great promise in removing or slowing further metastases - will they be made available, either during chemo or post chemo to help prevent metastases in stage 1, 2, and 3 patients? Answer - protocol recommendations, if any, should come out by the end of this year. Could be based on whether there was node involvement or any number of other factors. If recommended, patients that have completed treatment would take the appropriate drug along with their AIs - they are in pill form. There are side effects, for example low blood counts, so all this has to be figured in any new protocol recommendations.
On a personal note, I'm a little over 2 years past chemo, surgery, and rads, and have started to obsess over what may happen in the future. Since itt doesn't seem to be the “standard of care" to get any scans post treatment (unless or until new symptoms arise), i'm finding It pretty hard to move on with things without having at least some confirmation that treatment seems to have worked. I know this is irrational bcs nothing might show today but could in a month or year or 5 years from now - but I'd still like a new baseline (and frankly a new baseline every year or two to know what is or isn't going on in my body). Anywho, my sweet MO said he'd be doing me a disservice if I needed a scan to move forward - so I'm getting one. Whoop! Hope insurance pays ...
Also, heard a story on NPR about development of an “MRI lite" used instead of mammograms. These 15-second MRIs were hugely more successful at finding cancers, especially in women with dense breasts, than 3D mammography. I'm hoping the new MRIs will be developed enough so that we CAN all get affordable post treatment scans at regular intervals.
Lanne
-
Ingerp, I'm kind of like you-, every time I put cheese or eggs in my shopping cart at the supermarket I try to find out if it is a local, small family farm that treats their animals humanely. I've even gone so far as to email the company asking them how they treat their animals. I don't eat meat of any kind; opt for wild-caught fish only from time to time (I guess fish is meat). I know that growing almonds uses the most water, and I'm concerned about our over-use of that resource. Mostly I don't use any kind of plant milk much at all. I have been cautioned against eating a lot of calcium rich foods anyway-my MO tells me this because the AC chemo I had, coupled with a lot of calcium intake, increases my risk for heart disease. I take a 1000 mg tums every night. That's my calcium intake, which is enough according to my MO. I'm sure I get more in my plant-based diet as well.
Claire in AZ
-
The only info I got from 3 MOs and my BS was to stay active, at least 150 minutes per week Cardio and Strength. Get my BMI under 25, no smoking, limited alcohol and try to follow the Mediterranean Diet. High level the diet includes 2.5 servings of fruits & veggies daily, 3+ servings of fish weekly, 2-3 servings of Chicken/Turkey weekly, limited red meat (once per month) only use Olive Oil, cut down/out butter, whole grain only and increase healthy nuts (almonds, walnuts, cashews and Pistachios))
No mention of dairy, or soy or whatever i find online which seems to swing from good to bad every few years.
I don't drink a lot of milk but, I'm switching to Almond milk anyway since I need to take in more healthy nuts. I'm also looking at some vegan cheese recipes since they're made with cashews but, a lot of that will depend on the taste.
I'm going to do the best I can but, not going to make myself miserable. I want to do everything I can to live a long life but, that includes living happily while being healthy.
-
[University of Waterloo] researcher finds new, simple way to screen for breast cancer
A professor of electrical and computer engineering by trade, Ramahi and his team have created a prototype that uses micro-waves and artificial intelligence to detect abnormalities in the breast within minutes...
Ramahi said he hopes the device will be straightforward enough for any health care provider to use.
The prototype is also less harmful than traditional ways of breast cancer screening, Ramahi said, because it eliminates exposure to radiation.
"Our device uses a tiny, tiny fracture of what our cell phones emit," he said.
Ramahi and his team were able to build the device with less than $5,000 and its software can be uploaded to any Microsoft laptop. The versatility and affordability could help bring the technology to developing countries.
-
High [injected, not oral] doses of vitamin C found to enhance immunotherapy in combating cancer in mice
The researchers [of this new study in the journal Science Translational Medicine] found that adding high doses of vitamin C without immunotherapy resulted in delayed tumor growth in test mice. When it was given as part of an immunotherapy regimen with the mice, they found it slowed or stopped growth of melanoma, colorectal, pancreatic and breast cancer tumors. Furthermore, they found that it did so by providing support to T cells. They also found that vitamin C boosted the effectiveness of PD-1 and CTLA-4 checkpoint antibodies. And they found that in some cases, adding vitamin C to the immunotherapy regimen resulted in some breast cancer tumors disappearing completely.
https://medicalxpress.com/news/2020-02-high-doses-vitamin-immunotherapy-combating.html
Another article about the study: https://european-biotechnology.com/up-to-date/latest-news/news/vitamin-c-boost-checkpoint-inhibitor-efficacy.html
-
Good news about genomic testing -- just a proof of concept now, but hopefully it comes to market.
https://www.cancer.gov/news-events/cancer-currents...
-
interesting read, thanks for the link
-
ChristianaCare research shows radiation therapy for cancer can be both good and bad
Jennifer Sims-Mourtada, Ph.D., is director of Translational Breast Cancer Research at ChristianaCare's Helen F. Graham Cancer Center. Her research shows the inflammation caused by radiation meant to reduce the size of a tumor can in some cases create a pathway necessary for [triple negative] cancer stem cells to survive...
She notes there are inflammation inhibitors currently in clinical trials that could be paired with radiation therapy to reduce the inflammation and ensure cancer stem cells die from the treatment. Her team also identified an anti-inflammatory drug used to treat rheumatoid arthritis that could also be used to inhibit the growth of cancer stem cells and triple-negative breast cancer tumors.
-
FDA Accepts BLA for Subcutaneous Fixed-Dose Pertuzumab/Trastuzumab in HER2+ Breast Cancer
The FDA has accepted a Biologics License Application (BLA) for a fixed-dose combination (FDC) of pertuzumab (Perjeta) and trastuzumab (Herceptin) with hyaluronidase, administered by subcutaneous (SC) injection in combination with intravenous (IV) chemotherapy, for the treatment of eligible patients with HER2-positive breast cancer.
https://www.onclive.com/web-exclusives/fda-accepts...
-
Stick to breast imaging evidence, radiologists implore: 'Lives are at stake and compromise is unethical'
The Feb. 26 Journal of the American College of Radiology commentary implored docs to begin mammography testing of women at age 40, and at annual intervals. Recommendations from healthcare administrators or other nonradiologists that say otherwise should not dictate women's care, wrote lead author Harvard Medical School's Daniel Kopans, MD...
The team pointed to models from the National Cancer Institute, which have found that if women in their 30s wait until age 50 to receive screenings, as many as 100,000 could die from breast cancer that could have been caught earlier.
"The bottom line is that members of the ACR should support evidence-based guidelines in which most lives are saved by annual screening starting at the age of 40," the writers concluded.
-
Rapid MRI Tops 3D Mammo for Dense Breast Screening
— Accelerated breast MRI finds an additional 7 cancers per 1,000 women
A 10-minute MRI for breast cancer screening in women with dense breasts was associated with improved cancer detection compared with digital breast tomosynthesis (DBT), a cross-sectional study found.
Meaning Among women with dense breasts undergoing screening, abbreviated breast MRI was associated with a significantly higher rate of invasive cancer detection than DBT.
https://www.medpagetoday.com/hematologyoncology/br...
https://jamanetwork.com/journals/jama/article-abst...
doi:10.1001/jama.2020.0572
-
Lumpie - thanks for the article about abbreviated MRI. I read carefully to answer my question about contrast, and unfortunately it seems that will still be required. I can't imagine how 10 minutes will work for tech/nurses to put in an IV, position the patient, take the films w/o contract, start the gadolinium running & take the pictures with contrast, etc. Still, it's an interesting advancement. I suppose the chances that it will be cheaper are negligible.
-
MinusTwo:
Glad you found it helpful.
I get regular CT scans and they have me in and out of the room - complete with IV contrast - in WAY less than 10 minutes. {They're not just half-fast
} If they start using these fast MRI's for large segments of the population, I bet they will become more efficient and less expensive. Of course, there are many complex issues driving the cost of care. Sorry it sounds like you have a contrast issue. I know that will be a barrier for some. -
Lumpie - Love the "half-fast".... Not a specific contract issue, but lymphadema so I have a "stick" issue. They're hesitant to put the IV in my foot whether for a CT, MRI or PET.
Edited to say - we are so appreciative of the benefits of your research. Thanks so much.
-
I see...yes, most places have special rules for non-conventional (depending on how the institution defines it, that can be non-arm or below the belt) placement of IV's because they are deemed an elevated risk for infection. It can be a huge issue for those who have contraindication in both arms.
-
-
FDA Approves Neratinib Combo for HER2+ Breast Cancer
The FDA has approved a supplemental new drug application (sNDA) for neratinib (Nerlynx) in combination with capecitabine (Xeloda) for the treatment of adult patients with advanced or metastatic HER2-positive breast cancer who have received ≥2 prior anti–HER2-based regimens in the metastatic setting.
The approval is based on findings from the phase III NALA trial, which showed that the combination of neratinib and capecitabine reduced the risk of disease progression or death by 24% compared with lapatinib (Tykerb) plus capecitabine.
...neratinib in combination with capecitabine offers a significant improvement over currently available therapies in this heavily pretreated patient population and can be added to Nerlynx's established role in the treatment of early breast cancer."
https://www.onclive.com/web-exclusives/fda-approve...
Additional References
- Puma Biotechnology Receives U.S. FDA Approval of Supplemental New Drug Application for Neratinib to Treat HER2-Positive Metastatic Breast Cancer [news release]: Los Angeles, CA. Puma Biotechnology. Published February 27, 2019. https://bwnews.pr/2I02Xx8. Accessed February 27, 2019.
- Saura C, Oliveira M, Feng Y-H, et al. Neratinib + capecitabine versus lapatinib + capecitabine in patients with HER2+ metastatic breast cancer previously treated with ≥ 2 HER2-directed regimens: Findings from the multinational, randomized, phase III NALA trial. J Clin Oncol. 2019;37 (suppl; abstr 1002).
-
The Cancer Industry: Hype vs. Reality
Cancer medicine generates enormous revenues but marginal benefits for patients
"Today I'm giving a talk at my school, Stevens Institute of Technology, titled "The Cancer Industry: Hype Versus Reality." The talk focuses on the enormous gap between the grim reality of cancer medicine in the U.S. and the upbeat claims made by the cancer industry and its media enablers. Below are points I plan to make in my talk, which expand upon ones I've made in previous posts.—John Horgan"
https://blogs.scientificamerican.com/cross-check/t...
-
Casting for Recovery - Time to Apply
The 2020 retreat season kicks off in March and runs through November. Do you know someone who would benefit from a CfR retreat?
Please encourage them to apply!
Retreats are provided to women with breast cancer of any age and any stage of treatment or recovery, at no cost to the participants.https://castingforrecovery.org/breast-cancer-retre...
{Not research but I wanted to share the word! I have had the good fortune to attend a retreat. It was great!}
-
The Questionable Practice That Permeates Oncology Clinical Trials
{The problem is} a practice known as the 3-plus-3 approach, which is a type of rule-based design.
Rule-based designs identify the maximum-tolerated dose (MTD) on the basis of toxicity seen in a very small group of patients, and of the rule-based designs, the 3-plus-3 approach has been the most popular choice for decades. "It's ludicrous,"
The 3-plus-3 approach works like this: 3 patients are given a dose, which is often based on preclinical data, and if no dose-limiting toxicity (DLT) occurs, the next-higher dose is given to 3 different patients. This continues until one or more DLTs is seen.
"For the hundreds, if not thousands, of patients that are then being treated in later-stage trials, you're sort of stuck with that dose that's really based on 6 patients,"
...the decision to use the 3-plus-3 approach when other designs are available is a matter of ethics. "To my mind, that is ethically dubious to be using an outmoded design that is exposing more patients than needed to an unsafe and ineffective drug,"
other designs can be complex and pose a challenge for ... researchers
When cytotoxic agents were being developed, the belief was that efficacy and toxicity were correlated with dose.5 "For a long time, the approach to curing cancer has been to give the largest dose possible,"
{With newer drugs} the right dose could be one that exposes a patient to a therapeutically relevant amount, which can be determined by measuring the drug concentrations in the plasma — a practice also known as therapeutic drug monitoring.
{The article discusses alternative approaches.}
https://www.cancertherapyadvisor.com/home/cancer-t...
{The site did not require me to register. No subscription required.}
-
Lumpie - thanks again for your posts, questions on effectiveness/hype/max tolerated dose etc. It can be so hard to make the decisions on what to do. In 2016 for chemo a DR wanted to add a 3rd drug to the cocktail. When I asked, she said it would be a much more aggressive treatment, but that she thought I was young enough(58) and strong enough to tolerate it. SEs - over 10% women end up with heart problems. No thanks. As it turns out, the chemo did not do much to the tumor on the left side, and then 3 years later, the R-side has one, even after a bi-lateral. Would the 3rd drug have helped? Not convinced. And now, because of another medical condition, genetic counciling not realted to BC is recommended because it could indicate/recommend/get health insurance to pay for more screening and possible prevention of other non-BC cancers. Not convinced any of it would be more than diagnostic, without any real treatment. Do I want to be a F#*!#! lab rat ? No. Knowing what quesitons to ask. When to question the experts. So hard.
Ibrance and Arimidex. Supplements include Mg, D, biotin, C, Turmeric(Curcumin), Gluchosamine-Chondroitin,BoneUp(multi with Coligen),Thorne (another multi), Melatonine(at night).
2009 ER+ left breast. 52 yrs. Lumpectomy, Sentinel node removal, negative. Radiation 6 weeks, tamoxifen 5 years. Dense lumpy left breast, normal right. Acupuncture offered at facility as part of integrative medicine. It really helped with anxiety/stress during radiation treatment.
2016 ER+ left breast. Probably a new cancer, but unknown. 4 rounds TC Aug-Oct 2016, Bi-lateral (my choice) Nov 2016, no reconstruction. 2 sentinel nodes remove, negative. Cold Capping using Chemo Cold Caps (DIGNICAP not available). Anastrozole 1 mg starting May 2017. Joint issues noticed immediately. Stopped Anastrozole after 3-4 months due to joint stiffness in. After several months of no AIs, fingers were feeling better. Started tamoxifen March 2018
10/2018 noticed stiffness and some trigger finger again. Was eating meat a lot more (daily) than normal. Usually 1-2 /wk. Have cut way back on the meat, seems to help, but one finger still very prone to trigger finger. Trigger finger seemed to be getting better, but now 4/2019 seems worse, is it the break from added turmeric to meals?
6/18/2019 Noticed Swelling in R-arm, opposite side from where lymph nodes removed. . Could have been swelling earlier but wearing long sleeves. Ultra sounds for clots, Trip to urgent care. They did ultrasound, concerned that there might be a clot, there was not. 7/2/2019 lymphatic therapist recognized that there was something very wrong and sent me back to the DR.
8/2019 CT, Breast/chest , neck/thyroid ultra sound
9/2019 DR ordered biopsy, said it could be lymphoma, cancer, benign lymphatic. Biopsy R-axilla. Cancer. Genetic test showed no known markers (20+ looked for)
9/29/2019 PET scan, no indication of spread. Arimidex and Ibrance prescribed to shrink tumor prior to surgery, if needed.
10/2019 – Stopped Tamoxifen. Started Arimidex and Ibrance. Brand name Arimidex so far does not seem to have the SEs that generics did, but stiff/trigger finger on left middle finger returned.
1/2020 CT showed tumor in Axilla shrunk (hooray!!) from 2.3 to 1.1 but picked up something in lower bowel. DR consulted a DR I saw in 2011 who compared it to 2011 image, said they had not grown, but one has changed and was starting to obstruct.
2/14/2020 Happy Valentine's Day. Surgery removed to remove, waiting for pathology. 2/25/2020 – Pathology. Not cancerous. Hooray
-
BlueGirl: wow. That's a lot. And you are correct that, so often, it is difficult to discern the best course of action. I am glad that the recent pathology said not cancerous!
-
Immunotherapy Super-Responder: What Is Life, Not Exactly Cured?
— Lisa Geller's cancer has been gone nearly 4 years, but life has been far from normal
{Interesting piece on young-ish non-breast metastatic cancer patient who has responded to treatment but is living in limbo. Many will relate.}
https://www.medpagetoday.com/special-reports/exclu...
-
Thanks for this Lumpie. Effectively it appears that Lisa is exhibiting signs of PTSD... frankly I am not in the least surprised. I hope she receives the support she needs and deserves.
-
interesting story about Lisa Geller. My sister has been on opdivo for 5 years for metastatic lung cancer. She has stable mets. She is a walking miracle for many reasons. I keep telling her she should contact the mftr and be a paid spokesperson.
Dee
-
Do Proton Pump Inhibitors Exacerbate the Cognitive Effects of Breast Cancer Treatment?
The OSU researchers reviewed data from 3 prior unrelated studies. Rather than focus on specifically on PPI use, the studies focused on fatigue, yoga practice, and vaccine response in breast cancer survivors and patients. However, participants in each study self-reported use of prescription and nonprescription medications and provided regular self-reports of any cognitive symptoms they experienced.
When they examined the data, Ms Madison's team found that participants in 2 studies (labeled as study 1 and study 2) who used PPIs reported more severe problems with concentration compared with the nonusers, but did not report problems with their memory. In the third study (labeled as study 3), the women who used PPIs reported more severe memory problems compared with those who did not take PPIs. Participants in this group also reported an overall lower quality of life related to cognitive problems.
-
New drug combination could support better cancer treatments
Researchers have identified a promising new drug combination that could significantly help the immune system target cancer cells and kill them.
The study published in Cell, describes a treatment that works by combining an intravenous dosage of a well known anti-nausea drug, prochlorperazine (called Stemetil in Australia), with existing cancer treatments...
"Our long-term vision is to use this approach to not only clear a patient's cancer in the immediate term, but to prevent their cancer coming back in the future by establishing protective 'immune memory'," Dr Wells said.
Dr Simpson's team is now completing a safety trial of the combination of Stemetil and cetuximab in head and neck cancer, triple-negative breast cancer and adenoid cystic carcinoma patients at the Princess Alexandra Hospital.
This study is published in Cell (DOI: 10.1016/j.cell.2020.02.019).
https://www.miragenews.com/new-drug-combination-could-support-better-cancer-treatments/
-
New insight into breast cancer resistance to hormone therapy
An international team of researchers led by scientists at Baylor College of Medicine has new insights into the function of neurofibromin, a tumor suppressor produced by the NF1 gene. It is well known that neurofibromin keeps cancer growth in check by repressing the activity of a cancer driver called Ras. The new research reveals a previously unknown function of neurofibromin — directly repressing gene expression controlled by the estrogen receptor-α (ER). Thus, when neurofibromin is lost, Ras and ER functions are both activated, causing treatment resistance and metastasis for ER+ breast cancer.
These findings, appearing in Cancer Cell, suggest that a therapeutic approach must combine two different drugs, a SERD (e.g., fulvestrant) to degrade ER and a MEK inhibitor (e.g., selumetinib or binimetinib) to inhibit Ras downstream signaling, in order to effectively treat neurofibromin-depleted ER+ breast cancer. When this combination therapy was tested in animal models, the result was tumor regression. The next step is to begin clinical trials of the effectiveness of this therapeutic approach in patients.
https://community.breastcancer.org/forum/73/topics/860294?page=64&post_creation=true
-
debbew - Thanks for putting the article about the PPIs on here. I had read this before and was trying to find it again but couldn't find it. The article you linked also says that PPIs, if I understood it correctly, says that PPIs could be beneficial to chemotherapy. I wish the article provided more information about the studies. I know a couple of years ago PPIs were listed as one of the drug groups that could cause dementia but my gastroenterologist said that it was later shown that there was no link. I shared an article a week or so ago on I think the Ibrance thread about omeprazole may keep breast cancer from spreading. It's quite a quandary on whether it is beneficial or not.
-
A fascinating article about the abscopal effect and research that's currently being done to see how to induce/replicate this effect, using radiation coupled with other treatments, including immunotherapy
https://www.cancer.gov/news-events/cancer-currents...
-
bevjen
That would be such a great discovery if the flu vaccine could shrink tumors. I wish there was a clinical trial.
-
^You're welcome, cowgal! The article mentions that they are just starting to study the possibility that PPIs might be helpful to chemo, so for now I have not heard of any evidence of that yet.
-
Study reveals breast cancer cells shift their metabolic strategy to metastasize
New discovery in breast cancer could lead to better strategies for preventing the spread of cancer cells to other organs in the body, effectively reducing mortality in breast cancer patients. According to a study, published today in Nature Cell Biology, breast cancer cells shift their metabolic strategy in order to metastasize. Instead of cycling sugar (glucose) for energy, they preferentially use mitochondrial metabolism.
"This has important potential clinical implications because it suggests that drugs targeting mitochondrial metabolism may have efficacy for preventing metastatic spread in patients," said Devon A. Lawson, Ph.D., assistant professor in the UCI Department of Physiology and Biophysics and a member of the Chao Family Comprehensive Cancer Center at the UCI School of Medicine. "Historically, tumors were thought to contain dysfunctional mitochondria and be principally sustained by anaerobic glycolysis, or Warburg metabolism. Our work challenges that dogma and shows that breast cancer cells use mitochondrial metabolism during metastatic spread."
https://phys.org/news/2020-03-reveals-breast-cancer-cells-shift.html
-
Could cancer immunotherapy success depend on gut bacteria? [not bc-specific]
Using mouse models of malignancy, the scientists found that the intestinal microbe Bifidobacterium accumulates within tumors, transforming anti-CD47 unresponsive tumors into responsive ones.
The team's study, published today in the Journal of Experimental Medicine, discovered that the response to treatment depends on the type of bacteria living in the animals' guts. They then identified the mechanism, finding that the combination of antibodies against CD47 and gut bacteria works via the body's STING pathway of innate immunity—the body's first line of defense against infection...
The findings suggest that a probiotic might someday be used to improve anti-CD47 therapy, says Fu, a Cancer Prevention and Research Institute (CPRIT) Scholar and holder of the Mary Nell and Ralph B. Rogers Professorship in Immunology at UT Southwestern.
https://medicalxpress.com/news/2020-03-cancer-immunotherapy-success-gut-bacteria.html
-
Cancerous tumors, surrounding cells illuminated by new imaging agent
The imaging agent, referred to as LS301, has been approved for investigational use in small clinical trials at Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of Medicine. The first trial will investigate its use in imaging breast cancer.
"This unique imaging agent identifies cancer cells as well as other compromised cells surrounding the tumor," said Samuel Achilefu, PhD, the Michel M. Ter-Pogossian Professor of Radiology...
Achilefu expects that with a tumor and its surrounding fiefdom illuminated by the new imaging agent, doctors would have a better chance of removing the entire tumor as well as any areas that are likely to harbor microscopic cancer cells...
"There seems to be a type of immune cell that carries the imaging agent into the core of the tumor. So we now see the tumor margin and the core light up. This allows us to imagine a situation in which we could deliver a drug to the outside and the inside of the tumor at the same time. This dual targeting is not something we purposefully designed — it's not something we ever anticipated."
With this in mind, Achilefu's team conducted mouse studies to show that the researchers can attach a chemotherapy drug to the compound and use it to image the tumor and treat the disease simultaneously.
https://medicine.wustl.edu/news/cancerous-tumors-surrounding-cells-illuminated-by-new-imaging-agent/
-
Study Finds Potential of Whole Breast Ultrasound Tomography to Improve Breast Cancer Risk Assessment
This study demonstrated that increasing quartiles of whole breast volume-averaged sound speed were consistently and more strongly associated with increasing breast cancer risk than quartiles of mammographic percent density. These findings were statistically significant and suggest future opportunities for utilizing UST-breast cancer risk assessment, particularly in younger women with the absence of ionizing radiation.
"It is well-established that dense breast tissue is a breast cancer risk factor. This study suggests that whole breast ultrasound tomography may provide stronger and more specific information about that risk than mammography, which may ultimately help to stratify the risk in order to suggest more personalized screening and interventions," said Dr. Rachel Brem, Director, Breast Imaging and Intervention at The George Washington University and the Program Leader, Breast Cancer, at The George Washington Cancer Center. "We are encouraged by the study results that indicate the potential use of whole breast ultrasound to improve the accuracy of breast cancer risk assessment with a non-ionizing breast imaging modality."
-
Just wanted to let those who may be interested in a Washington Post subscription know that they are currently running a special. Info here: https://subscribe.washingtonpost.com/acq/?promo=e_.../offers/promo/e_nl_coron_gift_mar0920?utm_campaign=wp_to_your_health&utm_medium=email&utm_source=newsletter&wpisrc=nl_tyh&wpmk=1
{Disclosures: I do NOT have any pecuniary interest in either the Post or subscription purchases or links. Excuse the semi-commercial nature of the post. Just sharing info. Thx.}
PS: As a public service, the Post is making much of their coverage of Covid-19 available to the public without subscription.
-
Surgical Treatment of Breast Cancer Liver Metastases
- European Journal of Surgical Oncology
- In this Swedish National Patient Register study, the authors compared outcomes of 29 patients undergoing isolated liver resection or ablation for breast cancer metastases with outcomes of a control cohort of 33 patients with hepatic metastases receiving systemic treatment only. The median survival was 77 months in the procedural cohort compared with 28 months in the control cohort (P=.004). The intervention appeared to be safe, with no mortality reported at 90 days.
- The use of liver resection or ablation for breast cancer metastases warrants prospective evaluation.
-
Lumpie: Thanks for the Post link. Unfortunately I just renewed my digital subscription for $50.00. Urg. But glad they are making virus coverage available.
-
Cancer cells spread using a copper-binding protein
Previous studies have shown that, like other cancers, breast cancer coincides with higher levels of copper in the blood and in tumor cells... Researchers at Chalmers University of Technology have now identified a copper-binding protein that clearly affects breast cancer cell migration...
Further experiments revealed that Atox1 drives cell movement by stimulating a reaction chain consisting of another copper transport protein—ATP7A, and the enzyme lysyl oxidase (LOX). Atox1 delivers copper to ATP7A which in turn delivers the metal to LOX. LOX needs copper in order to function, and it is already known that LOX is involved in extracellular processes facilitating breast cancer cell movement.
"When Atox1 in the cancer cells was reduced, we found LOX activity to be decreased. Thus, it appears that without Atox1, LOX doesn't receive the copper required for its cell migration activity," says Stéphanie Blockhuys...
This indicates that Atox1 could be a biomarker for assessing how aggressive a breast cancer is. Such information could be used, for example, to determine if treatment to remove copper from the body could be appropriate. Atox1 could also become a target for drugs to block metastasis and thereby increase survival times.
https://medicalxpress.com/news/2020-03-cancer-cells-copper-binding-protein.html
-
Older women with breast cancer may benefit from genetic testing
About 1 in 40 postmenopausal women diagnosed with breast cancer before age 65 have cancer-associated mutations in their BRCA1 or BRCA2 genes, according to a study led by researchers at the Stanford School of Medicine.
The prevalence of the mutations in this group is similar to that of Ashkenazi Jewish women, whom the U.S. Preventive Service Task Force suggests should discuss their cancer risk with their physicians to determine if genetic testing is warranted. Currently, most guidelines don't address testing postmenopausal women with breast cancer in the absence of other risk factors.
The finding is the first to suggest that postmenopausal women who have been newly diagnosed with breast cancer but who don't have any hereditary risk factors, such as close family members diagnosed with breast cancer before age 50, may still benefit from genetic testing for inherited cancer-associated mutations.
-
Higher concentrations of IGF-1 are a probable cause of breast cancer
A growth hormone called insulin-like growth factor-1 (IGF-1) is likely to play a role in the development of breast cancer, according to new research published in the leading cancer journal Annals of Oncology [1] today (Wednesday).
IGF-1 is already known to encourage the growth and proliferation of cancer cells. Now, two analyses of information from several hundred thousand women enrolled in the UK Biobank study have shown that not only is there an association between higher levels of IGF-1 circulating in the blood and the development of breast cancer, but also, for the first time, that IGF-1 is likely to be a cause of the disease...
Dr Anika Knüppel, a nutritional epidemiologist at the University of Oxford, said: "The association between IGF-1 and breast cancer was first investigated in the 1980s and our findings are in line with various studies since then. But clarifying the direction of the association using Mendelian randomisation in our study leads the way for research into how the IGF-1 pathway can be harnessed in breast cancer prevention."
It may be possible to modify IGF-1 concentrations in the blood through changes to the amount and types of protein in a person's diet. In addition, drugs that target the IGF-1 system have been developed. There may be other, as yet unknown factors that can affect IGF-1 concentrations too.
https://www.eurekalert.org/pub_releases/2020-03/esfm-hco030920.php
-
That new imaging discovery is exciting stuff. Cancer is so friggin' sneaky.
-
These 30 drugs are in short supply in the US right now
The outbreak of the novel coronavirus has revealed the vulnerability of the supply chain of drugs that originate in China, which is the main supply source of raw ingredients for penicillin, ibuprofen, and aspirin.
However, drugs are frequently announced to be in short supply. In fact, the FDA has a running list of drug shortages due to anything from increasing demand to regulatory factors as well as supply disruptions.
24/7 Tempo has compiled a list of drugs in short supply from information provided by the Food and Drug Administration.
https://www.usatoday.com/story/money/2020/03/10/fd...
{I didn't see any cancer therapeutics on the list.}
-
Coronavirus hospital ward staffed by robots opens in Wuhan to protect medics
A coronavirus hospital ward staffed by robots to protect medics from the deadly bug has opened in Wuhan.
The program, ...will see the 5G-powered bots carry out tasks including taking patients' temperatures, delivering meals and disinfecting the facility.
It will also enable doctors to read patients' vitals remotely, reducing their exposure to the virus.
https://nypost.com/2020/03/10/coronavirus-hospital...
{That's one way to address a staffing shortage. Not very technical but since it relates to patient care, I thought others might be interested in this topic.}
-
Public Health and Law Experts Issue Guidelines for U.S. Response to Coronavirus Transmission
Monday, March 2, 2020
Widespread transmission of the COVID-19 coronavirus within the United States is "inevitable" and a successful response to the epidemic must protect the health and human rights of everyone in the country, over 800 public health, human rights, and legal experts and organizations warned today in an open letter to ... government officials.
Announcement/article here:
https://law.yale.edu/yls-today/news/public-health-...
Complete letter (mostly signatures):
https://law.yale.edu/sites/default/files/area/cent...
-
3 COVID-19 Cases as Described by Doctors in Wuhan
— True stories of what really happened
by Dr. Bernard March 11, 2020
{This is a somewhat technical description of the pathophysiology of what can happen with covid 19 patients. It will be *way too much* detail for many readers - but interesting for healthcare wonks. Proceed at your own risk! There is a video (13 minutes) and a transcription. Also a link to this doc's YouTube channel if you want even more.}
https://www.medpagetoday.com/infectiousdisease/cov...
https://www.youtube.com/channel/UCKOvOaJv4GK-oDqx-...
{Site may require users to register but in the past has not charged.}
-
Egads Lumpie! That’s frightening but thanks.
-
Statins starve cancer cells to death [not bc-specific]
Devreotes and his team began the new study with an unbiased screen of about 2,500 drugs approved by the U.S. Food and Drug Administration (FDA) to see which ones had the best kill rate of cells genetically engineered to have a mutation in a cancer gene called PTEN. The gene codes for an enzyme that suppresses tumor growth. Among the thousands of drugs, statins and in particular pitavastatin, emerged as a top contender in cancer-killing ability. Most of the other drugs had no effect or killed normal and engineered cells at the same rate. Equal concentrations of pitavastatin caused cell death in nearly all of the engineered cells, but very in few normal cells...
Devreotes and his team then looked at the molecular pathways that statins were likely to affect. It's well known, for example, that statins block a liver enzyme that makes cholesterol, but the drug also blocks the creation of a small molecule called geranylgeranyl pyrophosphate, or GGPP, which is responsible for connecting cellular proteins to cellular membranes...
Devreotes says, the scientists then measured the statin-treated cells' intake by adding a fluorescent tag to proteins in the cells' environment.
Normal human cells glowed brightly with the fluorescent tag, suggesting that these cells ingested protein from their surroundings regardless of whether the scientists added statins to the mix of nutrients and cells. However, human cancer cells with PTEN mutations took in almost no glowing proteins after the scientists added statins. The inability of the statin-treated cancer cells to make the protrusions needed take up proteins leads to their starvation.
https://medicalxpress.com/news/2020-03-statins-starve-cancer-cells-death.html
-
How Gilead's blood cancer med Zydelig might also address triple-negative breast cancer
Triple-negative breast cancer (TNBC) is hard to treat, because it lacks three common markers for drugs to target. Now, instead of going after the tumors directly, a research team led by the University of Sussex in the U.K. has found a target in their surrounding environment and identified an existing blood cancer med as a possible treatment.
The researchers found that using Gilead Sciences' FDA-approved Zydelig to target the PI3K pathway in the healthy tissues that surround cancerous cells could slow TNBC growth and reduce tumor metastasis in mice. They reported the findings in the Journal of Clinical Investigation...
To verify the effects of PIK3C-delta, the team tested Zydelig in two mouse models of TNBC. They observed a significant reduction in tumor growth following the treatment. Compared with control mice, animals that got Zydelig also saw significant decreases in the number of lung metastasis nodules...
"Our results suggest that repurposing already available drugs which act as inhibitors for [PIK3C-delta] could stop the progression of [TNBC]," Georgios Giamas, the study's senior author, said in a statement. "As the drugs are already available and FDA approved, clinical trials could begin immediately to further investigate the use of these inhibitors for triple negative breast cancer treatment."
-
Cancer Cells Go Down in Flames When Spark Returns to Gasdermin E
Gasdermin E appears to encode a protein that suppresses tumors. The problem, however, is that the gene is often mutated or silenced in many cancers. With hopes of rekindling gasdermin E's antitumor activity, scientists based at Boston Children's Hospital induced ectopic expression of gasdermin E in mouse models of cancer. The scientists not only demonstrated that this intervention could inhibit tumor growth, they also learned that gasdermin E suppresses tumors by converting apoptosis, a relatively subdued form of cell death, to fiery pyroptosis.
Detailed findings appeared March 11 in the journal Nature, in an article titled, "Gasdermin E suppresses tumor growth by activating anti-tumor immunity." According to this article, GSDME in tumors suppresses tumor growth by increasing the number and antitumor functions of tumor-infiltrating natural-killer (NK) and CD8+ T killer lymphocytes. It also enhances the phagocytosis of tumor cells by tumor-associated macrophages...
The scientists, led by Judy Lieberman, MD, PhD, chair, cellular and molecular medicine at Boston Children's Hospital and professor, pediatrics at Harvard Medical School, showed that in live mice, pyroptosis sounds a potent immune alarm that recruits killer T cells to suppress the tumor. When they reintroduced gasdermin E to mouse models where gasdermin E had been lacking, they were able to trigger pyroptosis and suppress growth of a variety of tumors (triple-negative breast tumors, colorectal tumors, and melanoma)...
"We have shown here that many cancer-related GSDME mutations reduce pyroptosis, and that mutations of D270, the shared GzmB/caspase 3 cleavage site and a prominent cancer mutation, have enabled tumors to evade tumor suppression by GSDME," the authors of the Nature article concluded. "Therapeutic strategies to induce GSDME—such as use of the DNA methylation inhibitor decitabine, an approved leukemia and myelodysplasia drug—are worth exploring."
https://www.genengnews.com/news/cancer-cells-go-down-in-flames-when-spark-returns-to-gasdermin-e/
-
Younger Cancer Survivors Far More Likely to Experience Food and Financial Insecurity than their Cancer-Free Peers, According to Researchers from American Cancer Society
- Online Publication Date: Mar 2020
Conclusions: Younger cancer survivors experience greater financial worry and food insecurity. In addition to coping with medical costs, cancer survivors with low income and multiple comorbidities struggle to pay for daily living needs, such as food, housing, and monthly bills.
https://www.nccn.org/about/news/newsinfo.aspx?News...
https://jnccn.org/view/journals/jnccn/18/3/article...
- DOI:
- https://doi.org/10.6004/jnccn.2019.7359
- Complimentary access is available until June 10, 2020.
-
Genes may predict cancer patients at highest risk of chemo brain after BMT
In the first study of its kind, researchers at the University of Alabama at Birmingham have identified genetic factors associated with cognitive impairment related to blood and bone marrow transplants. That information can better pinpoint patients at the highest risk for cognitive issues compared to using demographic or clinical characteristics alone. These findings were published in the Journal of Clinical Oncology on Feb. 21{, 2020}.
CONCLUSION
Inclusion of candidate genetic variants enhanced the prediction of risk of post-BMT cognitive impairment beyond that offered by demographic/clinical characteristics and represents a step toward a personalized approach to managing patients at high risk for cognitive impairment after BMT.
https://www.uab.edu/news/research/item/11167-genes...
https://ascopubs.org/doi/full/10.1200/JCO.19.01085
https://doi.org/10.1200/JCO.19.01085
{This article pertains to bone marrow transplant for leukemia, but given the topic, chemo brain, I thought the research might be of interest to others here.}
-
Blood biopsies offer early warning of cancer's return
Tests that look for hundreds of tumor mutations may detect residual disease in patients after treatment
Date: March 13, 2020
Personalized blood biopsies, which scan patient blood samples for genetic traces of cancer, could potentially provide an earlier warning of metastatic cancer before it is picked up through standard monitoring. Researchers in the Gerstner Center for Cancer Diagnostics at the Broad Institute of MIT and Harvard and Dana-Farber Cancer Institute have increased the sensitivity of blood biopsies, demonstrating that they can monitor up to hundreds of different cancer mutations in blood samples from individual patients, with the potential to detect cancer recurrence — and inform treatment decisions — years before traditional approaches could.
Conclusions: Tracking large numbers of individualized tumor mutations in cfDNA can improve MRD detection, but its sensitivity is driven by the number of tumor mutations available to track.
The study appears in Clinical Cancer Research, a journal of the American Association for Cancer Research.
https://news.harvard.edu/gazette/story/2020/03/per...
https://clincancerres.aacrjournals.org/content/ear...
DOI: 10.1158/1078-0432.CCR-19-3005
-
Lumpie - thank you for posting the blood biopsies links. BC for the 3rd f*#$#* time, twice left, now on the right. My DR thinks each is a "new cancer" rather than recurrence, but when pressed, said there is no way of really knowing. No evidence of mestasis. I wonder if these tests would also help indicate if the drugs, surgery, radiation really got it or if there are still rougue cells roaming around.
-
Blue girl: I'm so sorry! Have all of yours been the same type of cancer? (Hormone status, HER2, etc) Have your docs ordered genomic analysis on your specimens? (Foundation One is one such test.) That would tell them if it's the same cancer that keeps coming back or something different.
I think that the theory behind the blood biopsies described in the article is that it would tell whether there is cancer still lurking in your body and allow intervention before it "takes hold" and starts growing again. This technology is still in the research phase. Wonder if there is a way to get in a clinical trial? Even if there is, it may be too early in the development phase to benefit you, but what they learn could benefit others later.
This research is being done at the Broad Institute. Read about their premier project at MBCproject.org. https://www.mbcproject.org/
Those with MBC should be able to sign up to participate in the study if interested.
{I am in the MBC Project and another blood study at Johns Hopkins.}
Her is info about the study at Hopkins in case anyone is interested:
"The Breast Cancer Program Longitudinal Repository (BCPLR) is being established to fulfill the research mission of the Breast Cancer Program at Johns Hopkins and to serve investigators affiliated with it - to develop a repository of specimens with corresponding characteristics from patients seen in the breast care and cancer clinics."
Poster comment: This is a study rather that a clinical trial. In Baltimore Maryland. It is studying markers in blood and possible other tissue as well. They basically just want some blood and for you to fill out a questionnaire. The material notes that they may request medical records and even tissue samples. The program coordinator told me that they aren't requiring the tissue samples at present (@2018) so, while they could at some point in the future, do not allow that part to deter participation. They would like additional blood specimens if you change treatments or have a change in status. You do not have to be receiving treatment at Johns Hopkins to participate. If I can get us closer to a cure with a few vials of blood, I would do it every day of the week.
ClinicalTrials.gov identifier (NCT number): NCT01937039
and here is the link:
Johns Hopkins Breast Cancer Program Longitudinal Repository - Full Text View - ClinicalTrials.gov
-
It's interesting to read about earlier detection of MBC when my understanding is that doctors are often not in any rush to detect MBC before it is symptomatic with the tools they already have. I hope this bodes well.
-
It is pretty crazy how modern imaging techniques let see what was not seen before: up to 20 % of BC patients with stage II to III diagnosis were re-staged to MBC when scanned with FDG-PET-CT. It pretty well coincides with later relapse rates after treating for early stages. Means MBC de novo might be not 6 but >25 %. Very scary actually. Saulius
-
I’m pretty sure I fall into that fatality. I had metastatic disease within 6 months of finishing treatment, I think it was always there, they just didn’t know it. ill never know
-
I was told that Pet-CT was not standard for my DX but, I asked if they could make the attempt and see if my Healthcare Provider would cover it. I was lucky they covered most of it and the Pet-CT was clear.
Although, I have heard that Pet-CT will only catch something if its over a certain size so i guess there's still a possibility that something was too minor to see and even with getting chemo it might not get anything that went wandering.
Just have to hope that everything was caught early during my routine Mammo.
-
Cancer, heart surgeries delayed as coronavirus alters care
By MARILYNN MARCHIONEyesterday
https://apnews.com/c161afff751e36d0cac4b59760288eb...
-
Sorry, forgot to paste the article: https://academic.oup.com/jnci/article/104/24/1879/920222. Saulius
-
i just asked my MO about that yesterday. I'm doing neoadjuvant treatment for my Breast Cancer and, should get scheduled for surgery (BMX) 4 weeks (or so) after my last chemo treatment currently on track for 5/20.
He said my surgery wouldn't be postponed because it's not elective and, they should be able to get it scheduled.
I'm a little worried about delaying the surgery since HER+ is a more aggressive cancer and, can spread. We also need the final pathology to determine my next course of treatment (finishing a year of H/P or switching to Kadcyla - Herceptin combined with taegrted chemo for 14 cycles).
-
Interesting about the elective surgery; I believe surgeries dedicated to tumor removal (benign or malignant) are technically defined as elective - that was one of my first thoughts when they talked about postponing/canceling elective surgeries and the people who need mastectomies and the like. The Surgeon General addressed this a bit; his wife just went through treatment for recurrent skin cancer a year or two ago. He addresses the whole 'elective surgery' thing here saying that cancer surgeries are elective, but it's not something you could put off for 6 months...
-
thanks for the link.
Hoping I don't get delayed if I do it won't be beyond a couple of weeks.
I have an appointment with my BS at the end of April and will address it with him. I will also ask if doing a lumpectomy in the short term would be less likely to be delayed (if its possible to do) and then getting a BMX later.
Not sure if its better than waiting guess it depends on how long I might have to wait and what the cons are for waiting
-
Hoping it doesn't impact you and you can get surgery without any delay!
-
Statins may reduce HF hospitalization after chemotherapy for breast cancer
Among women undergoing chemotherapy for early-stage breast cancer, statin exposure reduced risk for hospitalization due to HF by up to 66%, according to a retrospective population-based cohort study presented at the American College of Cardiology Scientific Session.
-
The bacteria-trapping protein that may provide a new target for tracking and treating breast cancer
Scientists at the Pennsylvania State University and Henan University in China have found a new protein marker that they say could potentially predict the progression of breast cancer or be targeted by drugs designed to treat the disease.
The protein, called PAD4, is key in the immune response against bacteria. The researchers found that its expression in cancer cells can also promote breast cancer metastasis in mice, according to a new study published in the journal Molecular Cancer Research.
https://www.fiercebiotech.com/research/how-a-bacteria-trapping-protein-may-aggravate-breast-cancer
-
Lower breast cancer risk in RA unexplained by hormonal risk factors
"We found a decreased risk of breast cancer in patients with RA, and a similar decrease in risk of RA in patients with a history of breast cancer," Wadström and colleagues wrote. "We did not find evidence to support that the decreased risk of breast cancer was due to known risk determinants. Thus, we were ultimately unable to explain the origins of this association. Antihormonal therapy as used in secondary breast cancer pharmacoprevention does not seem to increase RA risk."
-
BC videos
NBCC is releasing a series of past webinars that give basic information about breast cancer, vaccines and other treatments. To launch this series, they have provided you with a link to a webinar featuring Dr. Keith Knutson, Mayo Clinic, presenting on the state of vaccines for breast cancer in 2019.
Vaccines For Breast Cancer – Where are we in 2019?
Link - https://vimeo.com/401115980/2a5f88254d
After the presentation, you can test your knowledge by taking a brief quiz on key concepts presented in the video.
{I've been taking a bit of a hiatus during the recent unpleasantness but will try to post compelling new finds as I come across them. Stay well, all!}
-
Just posting here because I got an email last evening from the Metastatic Breast Cancer Project, in which I am a participant (meaning I gave them samples and access to my medical records.) They are not exactly a clinical trial, but a data aggregator and interpreter.
In part the email said this:
We are continuing to process and analyze data, obtain clinical data from medical records, and prepare datasets for public release. We continue to engage with the scientific community to make sure the project data that are currently publicly available can help drive their research forward. We are also hard at work behind the scenes upgrading our infrastructure, designing new surveys and websites, and developing pilot projects to explore new ways for the MBCproject to collect and analyze data.
While these efforts remain underway, our laboratory operations at the Broad Institute of MIT and Harvard are on hold. As a result, saliva and blood kits will not be sent to patients until normal operations resume. If you have recently sent one in, we will be able to process kits that are already in transit. We will provide updates on kit delivery when we are back to being fully operational. The Broad Institute has paused these and other operations to convert a CLIA-certified testing center into a laboratory that can process COVID-19 patient samples.
So, sadly, it seems, Covid 19 is interfering with MBC research.
-
Notre Dame Developing 'Grain of Rice'-Size Breast Cancer Sensor
[Marker clips being designed that actively analyse breast cancer tumors.]
-
Pre-diagnostic 25-hydroxyvitamin D concentrations in relation to tumor molecular alterations and risk of breast cancer recurrence
-
My BS swears low Vit D levels are a huge contributor to BC. He's done an unofficial study of just his patients and finds this consistently. My levels were 28 when I diagnosed. I now run about 82 so here's hoping that's keeping BC away!
-
i read a study (when I was first diagnosed) done in Ireland and they believed Low Vitamin D played a role in Breast Cancer and well.
-
My level was 10 when I left a sunny state for a rainy state! I have several doctors that check my D level which is now in the 50s. It really jumped when I switched to a brand with flax oil. And yet one doctor I got by default and head of a big department said to me that they don’t regularly test for vitamin D! I left her in my rearview mirror after two visits.
-
I'm glad that they are looking at this more closely but just want to push back a little and say that all of this is still in correlation phase rather than causation here. Even if lower vitamin D were associated with breast cancer, it doesn't by any stretch mean that increasing vitamin d levels would reduce the rate.
-
Statins Appear to Protect the Heart Against Breast Cancer Treatment Toxicities
https://www.cancerhealth.com/article/statins-appear-protect-heart-breast-cancer-treatment-toxicities
-
Hepatic Resection for Breast Cancer Liver Metastases
- European Journal of Surgical Oncology April 02, 2020
- In this matched cohort study, the authors compared outcomes of patients with breast cancer liver metastases who received either systemic therapy alone (n = 763) or in addition to hepatectomy (n = 136). After propensity score matching, the 5-year overall survival rate was superior in the surgical group (56% vs 40%; P=.018). Among patients undergoing hepatectomy, the median overall survival was longer among patients with luminal B and HER2-enriched subtypes compared with luminal A and basal-like subtypes, and progression-free survival was significantly longer among patients with the HER2-enriched subtype compared with others.
- The authors concluded that these findings support the incorporation of surgery into appropriately selected patients with isolated breast cancer liver metastases.
- Conclusion:
Surgical resection of BCLM yielded higher OS compared with systemic
therapy alone and prolonged PFS among patients with the HER2-enriched
subtype. These findings support the use of surgical therapy in
appropriately selected patients, based on intrinsic subtypes.
- Commentary by Lillie D Shockney RN, BS, MAS, ONN-CG
This enlightening information needs to get into the hands of breast cancer tumor boards and surgical oncologists everywhere. It is common for a patient to only be in the hands of medical oncologists and occasionally also radiation oncologists once diagnosed with stage IV breast cancer. Note that I did not say "breast surgical oncologists" but instead "surgical oncologists" because the surgeons doing this type of procedure need to be the hepatobiliary surgical team members.
Identifying liver metastases when they are isolated and small becomes more important now. Trying to surgically remove multiple lesions of various sizes and in various locations within the liver usually isn't recommended, but one or two isolated lesions usually can be successfully excised and the recovery can be fairly quick, too.
https://www.practiceupdate.com/C/98424/56?elsca1=e...
https://www.ejso.com/article/S0748-7983(20)30373-5/fulltext
-
https://www.swissinfo.ch/eng/medical-innovation_sw...
Smart bra to detect breast cancer. This would probably work as a back up system. I'll have to ask the company if this takes mastectomies into consideration.
-
Lumpie,
Thanks for posting the report on resection of liver metastases. I saw that a few days ago and sent it to my MO. She was resistant when I wanted to do a microwave ablation of my largest liver lesion last summer, wanting to go into systemic treatment immediately instead. But it seems to have helped me, and this article is very helpful for others.
-
And I'm saving it for when I have future progression from bones to liver. Thank you!
-
I had a partial liver resection in 2015 for a solitary liver met. I have been very happy with that choice.
-
Thanks Lumpie for posting the study of hepatic resection for breast cancer mets. I had a liver resection for one liver met in June 2019. I have not regretted that decision, even though I now have more liver mets. The area that was resected has no evidence of disease. For people having a liver resection, I'd advise being aggressive about preventing constipation.
-
Sounds like several have had resection or ablation. They attempted ablation of my lesions in 2019. Were not able to complete due to proximity of lesions to colon. Bummer. I really wish we could have gotten rid of the only ones visible at the time. They had to incise me and attempt it before figuring out that it was not feasible. Mine was an out patient procedure with a tiny incision. In my experience, there was virtually no recovery. When it goes well, it is far less expensive than chemo and may result in fewer side effects. It seems that the improved outcomes are becoming better documented all the time. If this continues to be the case, it may be a more frequently used therapy for suitable candidates.
-
High fibre diet linked to lower breast cancer risk
Consuming a diet high in fibre is linked with a reducing in incidence of breast cancer, according to a random‐effects meta‐analysis published in the journal CANCER.
-
Immunomedics' Triple-Negative Breast Cancer Trial Halted Early Due to Compelling Efficacy
Positive results for clinical trial of sacituzumab govitecan for TNBC
-
The Development of CDK4/6 Inhibitors
For those who appreciate webinars, NBCC is "sharing a very special President's Council webinar conducted by a hero in the breast cancer community, Dr. Dennis Slamon, professor of medicine, chief of the Division of Hematology/Oncology and executive vice chair for research for UCLA's Department of Medicine, and the 2019 Lasker Award winner.
In this 45-minute webinar recording Dr. Slamon discusses, in very accessible language, the development of and the science behind CDK-4/6 inhibitors, a class of drugs that interrupt tumor cell proliferation.
We hope you enjoy this outstanding discussion about one of the most important therapeutic discoveries in the field of breast cancer since the development of Herceptin."
-
Association between early informed diagnosis and survival time in patients with lung cancer
Background: As a malignant tumor with high mortality, lung cancer (LC) often causes great trauma to patients, and a series of negative emotions and a heavy psychological burden accompanies poor prognosis. Whether or not to inform the patients of their condition has always been a controversial topic in the medical community. This retrospective cohort study investigated the association between early informed diagnosis and survival time in patients with LC.
Methods: A total of 29 825 patients with LC were enrolled between October 2002 and December 2016. The potential factors influencing LC survival were registered, including knowing their cancer diagnosis status, age, gender, pathological type, clinical stage, surgical history, hospital grade, and patient occupation. All participants were followed up every 6 months until June 2017.
Conclusions: Knowing their cancer diagnosis contributed to longer survival time in patients with LC, providing clear evidence that medical staff and patients' families should fully disclose cancer diagnoses to patients.
Funding information: National Science Foundation of China, Grant/Award Number: 81602734; National Social Science Fund of China, Grant/Award Number: 17ZDA327
https://onlinelibrary.wiley.com/doi/10.1002/pon.53...
https://onlinelibrary.wiley.com/doi/full/10.1002/p...
https://doi.org/10.1002/pon.5360
{Note: This research was done in China. In contrast to western practices, it has not always been the custom there to inform patients of their diagnosis.}
-
Immunomedics Announces ASCENT Study to be Stopped for Compelling Efficacy
A phase III clinical trial of the antibody-drug conjugate sacituzumab govitecan in triple-negative breast cancer stopped early because of "compelling efficacy across multiple study endpoints,"
"Triple-negative breast cancer (TNBC) is a disease with extremely limited treatment options beyond classic chemotherapy. The remarkable results we observed across multiple endpoints in the ASCENT study warranted early discontinuation of the trial and are indicative of a potential major advance in the treatment of this devastating disease that affects younger women and African American women at higher rates. I look forward to the release of the full and final analyses of these study data when they are available for public presentation."
ASCENT is a Phase 3 confirmatory study designed to validate the promising safety and efficacy data of sacituzumab govitecan observed in a Phase 2 study of heavily pretreated patients with metastatic TNBC (mTNBC). The primary endpoint for the study is progression-free survival, and secondary endpoints include overall survival and objective response rate, among others.
The Company hosted a conference call on April 6, 2020, to provide a clinical development and general corporate update. a webcast replay of the conference call will be available on the Company's website for approximately 30 days. at https://immunomedics.com/investors/.
https://www.immunomedics.com/our-company/news-and-...
-
Cancer Research UK, which funds about half of all cancer research in England, announced a £44 million ($54 million) cut in research support as a result of fundraising shortfalls.
https://www.cancerresearchuk.org/funding-for-resea...
-
Differences in Stage of Cancer at Diagnosis, Treatment, and Survival by Race and Ethnicity Among Leading Cancer Types
Question Do stage of cancer at diagnosis, use of definitive therapy, and survival differ by race/ethnicity among patients with 1 of the most common cancers?
Findings In this cohort study of 950 377 patients with cancer, stage at diagnosis, treatment, and survival varied by race and ethnicity. Overall, compared with Asian patients, black patients were more likely to have metastatic disease at diagnosis, black and Hispanic patients were less likely to receive definitive treatment, and white, black, and Hispanic patients had worse odds of cancer-specific and overall survival.
Meaning The findings of this study may lead to different management strategies based on race and ethnicity to improve outcomes.
https://www.upi.com/Health_News/2020/04/08/Black-p...
https://jamanetwork.com/journals/jamanetworkopen/f...
doi:10.1001/jamanetworkopen.2020.2950
-
Revolutionary Machine Learning Company Identifies Two Possible Treatments for Intractable Breast Cancer Type
The two therapy treatments successfully completed final in vitro organoid testing at Lawrence Berkeley National Laboratory, demonstrating "significant synergistic interaction" in killing malignant tumor cells, with statistically "low-to-no adverse effects" on healthy cells. With these results, Pattern Computer will proceed to the next phase of preclinical testing.
-
Seattle Genetics Announces U.S. FDA Approval of TUKYSA™ (tucatinib) for People with Advanced Unresectable or Metastatic HER2-Positive Breast Cancer
04/17/2020
-Approved for Patients with HER2-Positive Metastatic Breast Cancer Who Have Received One or More Prior Anti-HER2 Therapies in the Metastatic Setting-
-First HER-2 Tyrosine Kinase Inhibitor in Combination to Improve Overall and Progression-Free Survival in Patients with Metastatic HER2-Positive Breast Cancer With or Without Brain Metastases-
-Application Approved Four Months Prior to Action Date Under FDA's Real-Time Oncology Review (RTOR)-
BOTHELL, Wash.--(BUSINESS WIRE)-- Seattle Genetics, Inc. (Nasdaq:SGEN) today announced the U.S. Food and Drug Administration (FDA) granted approval to TUKYSA™ (tucatinib) tablets in combination with trastuzumab and capecitabine for adult patients with advanced unresectable (cannot be surgically removed) or metastatic HER2-positive breast cancer, including patients with brain metastases (disease that has spread to the brain), who have received one or more prior anti-HER2-based regimens in the metastatic setting. The FDA previously granted Breakthrough Therapy designation and Priority Review for TUKYSA and reviewed this application for approval under the Real-Time Oncology Review (RTOR) pilot program. The TUKYSA New Drug Application (NDA) is also part of Project Orbis, an initiative of the FDA Oncology Center of Excellence that provides a framework for concurrent submission and review of oncology drugs among participating international health authorities. TUKYSA is an oral, small molecule tyrosine kinase inhibitor (TKI) of HER2, a protein that contributes to cancer cell growth.
https://investor.seattlegenetics.com/press-release...
-
Urban vs. rural residence and outcomes in older breast cancer patients
Kelly M Kenzik, Gabrielle B Rocque, Wendy Landier and Smita BhatiaDOI: 10.1158/1055-9965.EPI-19-1414Abstract
Background: 20% of the US population resides in rural areas, yet is served by 3% of oncologists, and 7% of non-oncology specialists. Access to care issues can be compounded by lower socioeconomic status (SES) in rural areas, yet this issue is unexplored among older patients with breast cancer. Methods: Using SEER-Medicare, 109,608 patients diagnosed at ≥65y with breast cancer between 2000 and 2011 were identified. Residence status was combined with Federal Poverty levels: urban (high-, medium- and low-poverty); rural (high-, medium- and low-poverty). Five-year overall survival (OS) and healthcare utilization (HCU: visits to primary care provider [PCP], oncologist, non-oncology specialist, emergency department) were examined using urban/low-poverty as reference. The residence, HCU, mortality association was examined using mediation and moderation analyses. Results: Median age was 76y; 12.5% were rural, 15.6% high-poverty. 5y OS: 5y OS was 69.8% for rural and 70.9% for urban. Both urban- and rural/high-poverty patients had a 1.2-fold increased mortality hazard. Rural/high-poverty patients had a higher rate of PCP (Y1: IRR=1.23; Y2-Y5: IRR=1.19) and ED visits (Y1: IRR=1.82; Y2-Y5: IRR=1.43), but lower non-oncology specialist visit rates (Y1: IRR=0.74; Y2-Y5: IRR=0.71). Paucity of non-oncology specialist visits mediated 23%-57% of excess mortality risk. The interaction between residence/SES and paucity of non-oncology specialist visits accounted for 49%-92% of excess mortality risk experienced by rural/high-poverty patients vs. urban/low-poverty. Conclusions: Urban-rural residence mortality differences among older breast cancer patients are highly predicated by poverty level. Impact: Rural/high-poverty patients demonstrate less use of non-oncology specialists compared to urban/low-poverty, with disparities moderated by specialist use.
- Received November 12, 2019.
- Revision received February 12, 2020.
- Accepted April 10, 2020.
- Copyright ©2020, American Association for Cancer Research.
-
Paucity of non-oncology specialist visits mediated 23%-57% of excess mortality risk
Wait, does this mean that since they were not properly treated for other issues they died from those things instead of from cancer, and that's why their risk was mitigated??
For-profit medicine is killing us
-
Salamandra: yeah... Upon reviewing the article, I think the take away is "it is better to be rich and healthy than to be sick and poor" which was one of my grandfather's favorite "philosogisms." I think that lack of access to care is killing plenty of people. Much of the state of health care is mind-boggling. I read these reports of how life expectancy has not improved in decades... with a slight exception for herceptin... it's demoralizing... but then I think that there is no doubt in my mind - and plenty of clinical evidence - that available meds have kept me alive longer and with better QOL... so is there something killing off others faster so that they are offsetting my gains? The improved screening which started in the late 20th century was supposed to improve outcomes. So how the heck did unimproved outcomes happen and what can we do about it?
And then there is the problem of for-profit medicine. I'm not sure.... is it killing us or "just" making us bankrupt (literally... and figuratively)? And does that really help anyone? This one we definitely need to do something about.
-
Lumpie I think many bad health practices are on the rise, and so is childhood trauma-- things like this make for worse health outcomes society-wide, offsetting other gains. There is so much more obesity, depression, and anxiety than when I was a kid. Mental health struggles impact physical health a lot -- from the surging cortisol itself to the poorer self care practices which depressed people can have.
-
santabarbarian: Too true. Sadly, many aspects of health seem to have deteriorated. It is interesting, or perhaps I should say telling, that as we see financial security and aspects of the social fabric, including kinship ties, deteriorate, we see a deterioration of physical health. Of course, there is a greater recognition and acknowledgement of mental health challenges today than there was in the past but we can't ignore that our (post?) modern society does seem to have a troubling effect on mental health.
-
Just processing the speed, the change in a 24/7 news day is far more stressful mentally than a cave-human would ever be expected to deal with. The way stress responses are supposed to work is a cortisol surge that then drops away when you are safe. the kids of dangers and stresses we have now do not RESOLVE and so that becomes a toxic level of stress.
We have a "grandmother effect" -- human menopause is evidence that nature wanted more hands on deck to care for babies. So, lost kinship ties WOULD likely have a negative impact on child health.
-
PS read Dr Bruce Perry on tribal man. In a hunter gatherer tribe you'd have about 40 people, all of whom you knew INTIMATELY. If you were a baby you'd never be put down but rather carried by mom or elder sibling.... There would be a ratio of 4 adults to every kid under 6. So there was much better adult modeling/ time spent with adults and a more body-contact kind of upbringing. I can imagine a lot of anxiety is alleviated by the presence of trusted adults all the time.
-
May favorite prof in college taught Anthropology, so I took lots of anthro. We covered a South American indigenous tribe for a good year. (Thanks for the trip down memory lane.) Then I did a lot of maternal-child nursing. So I get the spaced pregnancies and kinship groups from both perspectives. (We clearly need more hands on deck!) And you are right: the intentionally anxiety-producing, relentless news cycles do nothing for our health!
-
I like the grandmother effect explained. It corresponds with what I read about native Americans culture with sisters, aunts, mothers and grandmothers. So many kids move away, have 2 income households and are in daycare, before care, after care. It's often good quality care but it's still not the same family they are around nights, weekends, ,etc. It's also reassuring that menopause is not natures way of saying "you've served your purpose - be gone".
-
Indeed, I think of it more like: "Hey you, with the experience and skills and patience: you are needed to help launch a baby!"
-
Interesting chat. Takes a village to raise a child
-
Interesting article on chemotherapy causing an immune suppression and the risk of ARDS which is what normally causes death in Covid19 patients. Actually, if I'm reading this correctly, it's good news for the immune suppressed group.
-
Jessie, this is fascinating and surely counter-intuitive! I read the article, and this could be my husband and I, though we're in our 70s rather than 60s. I was on fulvestrant and abemaciclib (Ibrance and Faslodex) for 23 mo before being switched to Xeloda. My husband and I have assumed that I am the more at risk of the two of us, but based on this article, it may be the reverse. The "cytokine storm" affect, which appears to be the cause of death in many Covid-19 cases, is lessened in this example because the woman is immunosuppressed whereas her husband is not, and it is he who suffers its affects. Thank you for posting this. I have sent it to my infectious disease professor/guru for his perusal!
-
The 10th Annual National Conference on Work & Cancer has gone virtual! This free, full-day online conference is open to patients, survivors, caregivers, healthcare/HR professionals* and anyone else touched by cancer. Stay tuned for the finalized agenda.
Cancer and Careers
Friday, June 19, 2020
8:45 AM - 5:00 PM Eastern TimeThe 10th-year anniversary of our National Conference on Work & Cancer will be held virtually on Friday, June 19, 2020!
This free, online daylong conference explores the complexities of balancing treatment and recovery with employment and is open to patients, survivors, caregivers, healthcare professionals, employers/HR professionals and anyone else touched by cancer.
Complimentary CEUs/PDCs are available for nurses, social workers and HR professionals. For more information on accreditation, click here.
Note: This event was previously scheduled to be held at the CUNY Graduate Center in NYC. Due to COVID-19, the National Conference will be hosted virtually instead.
Date:
Friday, June 19, 2020
Time:
8:45 AM-5:00 PM
Please log/dial in 10-15 minutes priorLocation:
Online
Webinar & phone options available
Login and dial-in info will be emailed to registrantshttps://www.cancerandcareers.org/en/community/even...
-
Joy -- I know --- it really is good news for those who are immunosuppressed. I have been thinking a lot about the people in that category and the people going through treatment now. I was hoping this article would relieve some of the additional stress. So glad it helped you -- will you let us know what your infectious disease professor says? I know two young people who have had ARDS -- one from the flu and the other from pancreatitis. Both were young with very strong immune systems.
-
I'm walking with the guru's wife this AM and will find out what he had to say. He's busy doing webinars almost every day on the coronavirus.
-
FDA approves pill for aggressive breast cancer that's spread in the body
Another article re Tucatinib. Easy to read. Includes OS and cost numbers.
-
Staying at One's Job to Maintain Employer-Based Health Insurance Among Cancer Survivors and Their Spouses/Partners
Many cancer survivors experience challenges related to employment, including limitations in ability to work. Given that most health insurance coverage for working-age individuals in the US is employer-based, a challenge is the inability to freely leave a job given limitations on health insurance portability, also called job lock. Job lock can negatively affect career trajectory and quality of life. Likewise, spouse/partner job lock can also affect family well-being. We examined job lock prevalence among cancer survivors and their spouses/partners and associated factors in the US.In this study, approximately 1 in 3 cancer survivors in the US reported job lock for themselves or their spouses/partners, suggesting that job lock is common and has implications for the well-being and careers of both survivors and their families. Given higher prevalence of job lock among younger survivors and those with incomes near the poverty level, it is important to note that those earning between 138% and 400% of the FPL are ineligible for Medicaid and may have fewer employment alternatives with comprehensive health benefits. Clinicians, social workers, and navigators have opportunities to identify job lock and other employment concerns throughout treatment/survivorship care and connect survivors with employment and health insurance counseling.Kent EE, de Moor JS, Zhao J, Ekwueme DU, Han X, Yabroff KR. Staying at One's Job to Maintain Employer-Based Health Insurance Among Cancer Survivors and Their Spouses/Partners. JAMA Oncol. Published online April 23, 2020. doi:10.1001/jamaoncol.2020.0742 -
Fight or Flight: Does Stress Make Radiation Therapy Less Effective?
— Suppressing beta-receptor signaling enhanced tumor control in preclinical study
-
mysticalcity - that is fascinating. So possibly the women who experience the most stress from the process of radiation also get the least benefit. ARGH but also so glad they are studying this.
-
Triple negative breast cancer might not actually be 'breast cancer'
....Researchers have discovered...that the molecular mechanisms involved are more closely related to non-breast cancers, and two specific gene mutations may be responsible for the tumor development.
The research team found the presence of a mutated p53 (a tumor suppressor gene whose mutation often leads to cancer development) and a mutated PARP (a gene that maintains DNA integrity) in a large majority of patients with triple negative breast cancer. Specifically, they found that p53 would interact with replicating DNA and PARP, driving cell growth and division.
"Our new findings suggest that the presence of both [p53] and PARP could serve as a good identifier of breast cancers that would respond to combined treatment with talazoparib — a PARP inhibitor that was developed to treat breast cancers with the BRCA mutation — and temozolomide — a chemotherapy agent that is used to treat some brain cancers," said Professor Jill Bargonetti, whose lab conducted the research. "This is an exciting finding because it could lead to the first targeted therapy for triple negative breast cancer, enabling more precise and effective treatment of a very aggressive form of the disease."
...this group plans to test if this combination of drugs can successfully block replication of triple negative breast cancer cells in xenographed animal models. If the therapy can prove to be successful, it would very likely lead to the reclassification of triple negative breast cancer to a category of cancers called mutant p53/PARP1 positive cancers, which are treatable with a combination PARP inhibitor therapies.
This study gives doctors two new biomarkers to test for in patients, and many new potentials in clinical trials, which can be fast tracked since so many drugs already exist that target these specific genes. While this study only tested out two drugs, there are many other drugs that specifically target p53 and PARP, and many more which can be developed, which may give even better results. Hopefully, there will be many new, positive developments for this disease following this discovery.
https://www.clinicalomics.com/topics/precision-med...
https://cancerres.aacrjournals.org/content/early/2...
DOI: 10.1158/0008-5472.CAN-19-1036
-
that's very exciting news
-
It is exciting. And p53 and PARP mutations are pretty common among other types of breast cancer. So maybe the research may lead to new tools for treating other sub-types, too.
-
A couple of days ago I stumbled on a piece of research that might have been linked here before, as it came out in July 2019. But I hadn't seen it and thought it was exciting news about recurrence risk for TNBC. TNBC has a relatively high recurrence risk (in the past week I've seen research numbers such as 22%, 25%, and 42%, so who knows what the real figure is. Regardless, it's high.) Since we don't know which patients will recur and which won't, almost all of them go through the whole range of treatment, including chemo. If we could identify the patients least likely to recur, they could perhaps be spared some of the more aggressive treatment. Here is the abstract and link.
"Approximately 40% of patients with stage I–III triple-negative breast cancer (TNBC) recur after standard treatment, whereas the remaining 60% experience long-term disease-free survival (DFS). There are currently no clinical tests to assess the risk of recurrence in TNBC patients. We previously determined that TNBC patients with MHC class II (MHCII) pathway expression in their tumors experienced significantly longer DFS. To translate this discovery into a clinical test, we developed an MHCII Immune Activation assay, which measures expression of 36 genes using NanoString technology. Preanalytical testing confirmed that the assay is accurate and reproducible in formalin-fixed paraffin-embedded (FFPE) tumor specimens. The assay measurements were concordant with RNA-seq, MHCII protein expression, and tumor-infiltrating lymphocyte counts. In a training set of 44 primary TNBC tumors, the MHCII Immune Activation Score was significantly associated with longer DFS (HR = 0.17; P = 0.015). In an independent validation cohort of 56 primary FFPE TNBC tumors, the Immune Activation Score was significantly associated with longer DFS (HR = 0.19; P = 0.011) independent of clinical stage. An Immune Activation Score threshold for identifying patients with very low risk of relapse in the training set provided 100% specificity in the validation cohort. The assay format enables adoption as a standardized clinical prognostic test for identifying TNBC patients with a low risk of recurrence. Correlative data support future studies to determine if the assay can identify patients in whom chemotherapy can be safely deescalated and patients likely to respond to immunotherapy.
Significance: The MHCII Immune Activation assay identifies TNBC patients with a low risk of recurrence, addressing a critical need for prognostic biomarker tests that enable precision medicine for TNBC patients."
-
Adjuvant Chemotherapy Associated With Early, But Not Sustained, Cognitive Impairment in Women With Early-Stage Breast Cancer
he
addition of chemotherapy to endocrine therapy in the treatment of early-stage
hormone receptor-positive, HER2-negative breast cancer was associated with a
significant increase in the level of perceived cognitive impairment, according
to results of the TAILORx trial published in the Journal of Clinical Oncology.At the 3-month assessment, 36.7% and 26.3% of
patients treated with and without chemotherapy vs no reported cognitive
impairment. While a
significant difference in patient-reported cognitive impairment was also
observed when these respective groups were compared at 6 months, it was no longer seen at 12
months and beyond....neither patient age nor menopausal status was associated with changes in perceived cognitive impairment.
https://www.oncologynurseadvisor.com/home/cancer-t...
Wagner LI, Gray RJ, Sparano JA, et al. Patient-reported cognitive impairment among women with early breast cancer randomly assigned to endocrine therapy alone versus chemoendocrine therapy: results from TAILORx [published April 9, 2020]. J Clin Oncol. doi: 10.1200/JCO.19.01866
-
cfDNA Test May Detect Disease Among Patients Who Are Suspected of Having Cancer
A plasma cfDNA test was able to detect cancer in patients who had a high suspicion of cancer, and was able to predict tissue of origin among patients with confirmed cancer, according to results presented at the American Association for Cancer Research (AACR) Virtual Annual Meeting I 2020.
In the overall substudy 2 cohort, the cfDNA test had 99.8% and 99.3% specificity for detecting cancer in training and validation, respectively. In the HCS subgroup from substudy 2, the specificity increased to 100% for both training and validation.
https://www.cancertherapyadvisor.com/home/cancer-t...
Thiel DD, Chen X, Kurtzman KN, et al. Prediction of cancer and tissue of origin in individuals with suspicion of cancer using a cell-free DNA multi-cancer early detection test. Presented at: American Association for Cancer Research (AACR) Virtual Annual Meeting I; April 27-28, 2020. Abstract CT021.
-
Meet My Loved One: Making palliative connections in times of isolation
...she wrote down all the little personal details she would have told the nurses and staff as if she were there in person. The fact that he liked to watch "Animal Planet." His love of ice cream, and his distaste for rice. His preference for cold drinks that felt better when he swallowed. And that no one needed to make him wear his oxygen if the canula made him uncomfortable. She emailed it to her dad's social worker and asked that it be taped on the wall.
The effort, and the health care team's response, brought her some peace of mind.
"It's the little things that mean so much," {his daughter} Harding said.
https://www.uab.edu/medicine/palliativecare/patient-care/covid-19-resources
{Not therapeutic research but I thought this might be helpful to someone.}
-
Congress must tackle patient matching amid COVID-19, says Pew Charitable Trusts
Persistent flaws in the ability to accurately ID and match patient records are hindering two must-haves on the road to reopening: contact tracing and, eventually, vaccine administration.
Detailed contact tracing in the short term and a nationwide vaccination program in the long term "hinge on having correct patient demographic data," according to the letter, but "current flaws in the identification and matching of patient records inhibit the nation's ability to accomplish these efforts successfully."
The need for better patient matching is a drum that Pew has been beating for a long time....
{An interesting is slightly wonky, discussion of a current public health issue.}
-
Lumpie - love the article about the Dad in palliative care and what his daughter wrote to post by his bedside. Great ideas. Something we should all pay attention to even when there is no virus.
-
Killing 'sleeper cells' may enhance breast cancer therapy
The research, which used breast cancer cells taken from patients, was the first to show that venetoclax could kill sleeping, or "senescent," cancer cells.
The promising preclinical results for this "triple therapy" have underpinned a phase 1 clinical trial in Melbourne that is combining venetoclax with hormone therapy and CDK4/6 inhibitors in patients with ER+ breast cancer.
https://medicalxpress.com/news/2020-05-sleeper-cells-breast-cancer-therapy.html
-
Hypofractionated Breast Radiotherapy for 1 Week Noninferior to 3 Weeks
- The authors report the 5-year efficacy data from a phase III trial designed to compare hypofractionated breast radiotherapy for 1 week versus 3 weeks for localized breast cancer. A radiotherapy schedule of 26 Gy in 5 fractions over 1 week was found to be noninferior to 40 Gy in 15 fractions over 3 weeks in terms of local tumor control. In addition, the 1-week schedule had similar tissue effects at 5 years compared with the 3-week schedule.
- Patients prescribed adjuvant local radiotherapy following primary surgery for early-stage breast cancer may consider a 1-week hypofractionated radiotherapy schedule.
DOI:https://doi.org/10.1016/S0140-6736(20)30932-6
-
Quality-of-Life Outcomes in Surgical vs Nonsurgical Treatment of Breast Cancer–Related Lymphedema
- The authors of this systemic review found that health-related quality-of-life outcomes in patients with breast cancer–related lymphedema were associated with improvement following treatment with vascularized lymph node transfer in 2 studies. However, complex decongestive therapy studied in 14 trials had variable associations, and diverse outcome measures and varied protocols limited interpretation.
- Additional studies comparing outcomes with surgical and nonsurgical management of breast cancer–related lymphedema are needed.
doi:10.1001/jamasurg.2020.0230 -
Prediagnostic serum selenium levels in relation to breast cancer survival and tumor characteristics
...The Malmö Diet and Cancer Study, a population‐based cohort study of 17,035 women recruited between 1991 and 1996, was used for breast cancer cases and controls. After exclusion, they assessed 1,066 cases. Among breast cancer free women, they selected controls both from matching (n = 694) as well as randomization (n = 492). Analysis revealed no correlation between serum Se quartile and any tumor characteristic or intrinsic subtype. Women in the highest Se quartile had lower overall mortality than those in the lowest. They identified similar results for breast cancer‐specific mortality. Findings thereby support the association of Se with a lower mortality in breast cancer.
-
Cancer screenings drop upward of 94% during pandemic, with concerns of lingering sluggishness
Routine cancer screenings have dropped precipitously during the COVID-19 pandemic's initial spread, a trend that has experts concerned about an explosion in more severe diagnoses in the coming months.
Epic recently made this discovering after analyzing data from about 2.7 million patients, treated at 190 hospitals across 23 states. The electronic health record vendor specifically targeted cervical, colon and breast cancer, and found a roughly 86%-94% drop in screening levels when compared to previous care volumes logged between 2017-2019.
-
While I'm sure there are people who felt safer to skip, I know a lot of my friends had their Mammos canceled by the facility, they weren't happy
-
I'm an ICU nurse. I know I need an end-of-life directive. So why can't I bring myself to write it?
{Not research but one of the best articles I have found on issues surrounding advanced directives. We all know, at some level, that we need them but the cookie-cutter approach just does not seem to fit. So we do nothing.}
https://www.washingtonpost.com/health/im-an-icu-nu...
{Wa Po may allow access to a limited number of articles per month without subscription.}
-
"Hypofractionated Breast Radiotherapy for 1 Week Noninferior to 3 Weeks"
Wow, this will make a big difference in the experience of treatment for many people, and I think make compliance much more feasible for women with less flexible work options.
-
Salamandra: I agree. I had to read it twice (or more) to be sure I understood it correctly. Many women have foregone lumpectomy owing to the burdens of the follow up radiation schedule. Travel and transporation to care, time off work and numerous other complications can be issues. A dramatically shortened schedule would make this less invasive surgery a more feasible option for some.
-
Carbohydrate quality index and breast cancer risk in a mediterranean cohort: The SUN project
(Summary of Clinical Nutrition — Romanos-Nanclares A, Gea A, Martínez-González MA, et al. | May 11, 2020, https://www.mdlinx.com/ct.cfm?cid=7686001&typ=js&rdr=https://www.clinicalnutritionjournal.com/article/S0261-5614(20)30211-9/fulltext?rss=yes&mor=1)
In this study, the relationship between an a priori defined carbohydrate quality index (CQI) and the incidence of BC were tested in a Mediterranean cohort study. A validated semi-quantitative 136-item food-frequency questionnaire was applied in a prospective follow-up study of 10,812 middle-aged women. Researchers assessed the CQI following 4 criteria at baseline: dietary fiber intake, glycemic index, whole grain:total grain ratio and the solid carbohydrate:total carbohydrate ratio. Subjects were classified into quartiles according to the final CQI score. This Mediterranean cohort exhibited a significant inverse association with the incidence of BC after a better quality of dietary carbohydrate intake, which imply that strategies for cancer prevention should demonstrate the quality of this macronutrient.
https://www.mdlinx.com/journal-summaries/breast-cancer-nutrition/2020/05/11/7686001/
-
Caution on prolonged wearing of masks for those with cancer:
People with cancer, especially if the cancer has spread, will be at a further risk from prolonged hypoxia as the cancer grows best in a microenvironment that is low in oxygen. Low oxygen also promotes inflammation which can promote the growth, invasion and spread of cancers.8,9 Repeated episodes of hypoxia has been proposed as a significant factor in atherosclerosis and hence increases all cardiovascular (heart attacks) and cerebrovascular (strokes) diseases.
https://www.technocracy.news/blaylock-face-masks-pose-serious-risks-to-the-healthy/
-
That website- technocracy.news is not an credible news site and the article doesn't contain accurate scientific information.
-
The writing has some real slips of logic.
-
Hi All, We are wondering how many of you read our research news articles. We're thinking of getting a group together to get some feedback. Would you PM us Mods to let us know if you do? Thank you!
-
would be good if you put it in a thread so we could mark it under favourites
-
Kanga - there is a thread. Here's the link. Interestingly I mostly read the articles, either here or there, that are relevant to my diagnosis & treatment.
https://community.breastcancer.org/forum/73/topics...
-
New Map Reveals Distrust in Health Expertise Is Winning Hearts and Minds Online
Researchers warn scientists are fighting health misinformation in the wrong place.
Communities on Facebook that distrust establishment health guidance are more effective than government health agencies and other reliable health groups at reaching and engaging "undecided" individuals, according to a first-of-its-kind study published today by researchers at George Washington University and other institutions in the journal Nature.
The researchers tracked the vaccine conversation among 100 million Facebook users during the height of the 2019 measles outbreak. The new study and its "battleground" map reveal how distrust in establishment health guidance could spread and dominate online conversations over the next decade, potentially jeopardizing public health efforts to protect populations from COVID-19 and future pandemics through vaccinations.
https://www.nature.com/articles/s41586-020-2281-1
Johnson, N.F., Velásquez, N., Restrepo, N.J. et al. The online competition between pro- and anti-vaccination views. Nature (2020). https://doi.org/10.1038/s41586-020-2281-1
-
Impact of Stopping Trastuzumab in Early Breast Cancer
- Journal of the National Cancer Institute This retrospective study was designed to evaluate the impact of early discontinuation of adjuvant trastuzumab on outcomes in patients with early-stage HER2+ breast cancer. Early discontinuation of trastuzumab was associated with an increased risk of relapse and death.Adjuvant trastuzumab should be continued for a year in patients with early-stage breast cancer.CONCLUSIONS: BC patients in Ontario who did not complete adjuvant trastuzumab had a statistically significantly higher risk of BC relapse and death and low incidence of cardiac death. These findings support one year of adjuvant trastuzumab in early stage BC.https://www.practiceupdate.com/C/100061/56?elsca1=emc_enews_topic-alerthttps://academic.oup.com/jnci/advance-article-abstract/doi/10.1093/jnci/djaa054/5826355?redirectedFrom=fulltexthttps://doi.org/10.1093/jnci/djaa054
-
A sincere and very interesting article: https://www.onclive.com/publications/Oncology-live/2020/vol-21-no-10/looking-forward-to-a-new-wave-of-breast-cancer-therapies
-
BSandra, thanks for sharing that very interesting article. My MO informed me that I am now HER2-low, so that trial especially piqued my interest.
-
Dear Bliss, dear ShetlandPonny, I htink you could well chat together about Her2low. ShetlandPonny just got a PhD in Her2low/Her2mut:>, and could really help with explaining how to use this situation to make you benefit. Might be you are eligible for the same clinical trial, if they still recruit? Saulius
-
'They killed her': Why are breast implants still putting millions of women at risk?
Allergan's "medical aesthetics" products helped persuade AbbVie to buy the company. But what if the devices driving profit are also endangering women's health?
Press coverage of breast implant issue: "The causes of the various problems with breast implants are still poorly understood, which public health experts blame on a lack of testing or objective, long-term studies that do not rely on manufacturer-provided data or funding. Device makers also have yet to fully report the data the FDA required as a condition of allowing silicone implants back on the market in 2006."
https://fortune.com/longform/breast-implants-dangerous-allergan-abbvie-acquisition/?j16sc8
-
I'm also low her2. Her2- by fish. I've been reading articles about how they are starting clinical trials for us using some of the her2 drugs. It's very promising as I know there are quite a few her2 women out there that have done well. Shetland, are you low her2 or did yours mutant to her2?
-
An arm of the DS8201a/Enhertu trial was taking low HER2 patients.
-
Thanks Lumpie. I'll pull up the trial and take a look at it.i've been on I\L for a year and a half and have been doing well. I also know that the combo has an avg of 27 months, so I know it's just a matter of time before my cancer wakes up again. I am interested trying a clinical trial so I'll check it out.
-
Here's a link:
ClinicalTrials.gov Identifier: NCT03734029 Trastuzumab Deruxtecan (DS-8201a) Versus Investigator's Choice for HER2-low Breast Cancer That Has Spread or Cannot be Surgically Removed [DESTINY-Breast04]
https://clinicaltrials.gov/ct2/show/NCT03734029?term=DS-8201a&cond=Breast+Cancer&draw=2&rank=4BTW, It's for unresectable, and/or metastatic breast cancer.
PS: Simone80: Hope you don't need to change Tx for a long time. I was on a different branch of the Destiny trial. It was a great experience. The clinical trial staff and medical director at my site were fabulous. Good luck!
-
Interesting information as always. Lumpie thanks for the article on the PALVEN trial, that’s a hopeful one for those of us on I/L
-
Thanks Lumpie. I hope to get another year out of I\L, but just in case.
-
Simone, to answer your question, the cancer acquired a mutation in the HER2/ERBB2 gene. It is still HER2 negative (non-amplified).
-
Wallygal posted this in Clinical trails/research. I am reposting it here. Interesting report on Genome Study (no the original study) in ScienceDaily, more DNA variations found that might be linked to BC. https://www.sciencedaily.com/releases/2020/05/200518144849.htm . Has anyone else had a genetic profile done that insurance denied ? My DR ordered one Sept 2019 when 3rd BC found, specific to BC, looking at at over 20 markers (none found). Insurance sent me an official denial, the lab who did the work is fighting it,
-
BlueGirl: denied after your 3rd BC? That is outrageous! It's standard of care! How can insurance get away with that? I hope that you will let your legislators, both state and federal, know about this. How insurers can get away with not covering standard of care is beyond me! It should not happen.
-
Shetland, MO said the pathologist told her she labeled me HER2 negative because there were fewer than 10% cells; the report says 8%. Does that mean non-amplified? MO is keeping me on current tx for now.
-
Reading all the posts in various forums, it is increadible what is covered/what it not, the care, advice etc people get. The denial is being appealed, and one patient support advocate felt confident that insurance would cover all or most of it. Contacting my representatives is a waste of time. I have contacted them on several issues including health, and their replies often do not address what I wrote about, or are non-commital, or tell me why I am wrong. We passed an initiative on the ballot to expand Medicaid in this state, and legislators made an attempt to weaken or get rid of it (they failed). They also made an attempt to make the initiative process much more difficult. ( We know more than you do). So far that has failed as well. I do not celebrate the idea of "Medicare for All", because the focus is on insurance/who pays/how much, and not on health care itself. I know some people have no or poor coverage and this would be a chance to pay for treatment they cannot afford. So Medicare is certianly is part of the equation. The other day there was an interview on NPR with a woman whose surgery for BC had been postponed because of covid-19. Her tumor has grown a lot, and the treatment she now requires, is much more invasive. It sounded less hopeful as well.
-
Dear all, these are not breaking news but we have to keep an eye on Tesetaxel, an oral Taxane. It achieved high response rates in clinical trials even in patients pretreated with other taxanes. I know ow amazing Docetaxel was for my wife, and Tesetaxel (not to mention it is oral) seems very promising:
https://www.ascopost.com/issues/july-25-2018/oral-...
https://www.odonate.com/tesetaxel.
Saulius
-
Saulius, thanks so much for the article. I was not aware of Tesetaxel. I will investigate further with my own MO. Very encouraging!
-
DHA Affects Microtubule Dynamics Through Reduction of Phospho-TCTP Levels and Enhances the Antiproliferative Effect of T-DM1 in Trastuzumab-Resistant HER2-Positive Breast Cancer Cell Lines
May 23, 2020
Publication: Cells (Open access)
Trastuzumab emtansine (T-DM1) is an anti-human epidermal growth factor receptor 2 (HER2) antibody-drug conjugated to the microtubule-targeting agent emtansine (DM1). T-DM1 is an effective agent in the treatment of patients with HER2-positive breast cancer whose disease has progressed on the first-line trastuzumab containing chemotherapy. However, both primary and acquired tumour resistance limit its efficacy. Increased levels of the phosphorylated form of Translationally Controlled Tumour Protein (phospho-TCTP) have been shown to be associated with a poor clinical response to trastuzumab therapy in HER2-positive breast cancer. Here we show that phospho-TCTP is essential for correct mitosis in human mammary epithelial cells. Reduction of phospho-TCTP levels by dihydroartemisinin (DHA) causes mitotic aberration and increases microtubule density in the trastuzumab-resistant breast cancer cells HCC1954 and HCC1569. Combinatorial studies show that T-DM1 when combined with DHA is more effective in killing breast cells compared to the effect induced by any single agent. In an orthotopic breast cancer xenograft model (HCC1954), the growth of the tumour cells resumes after having achieved a complete response to T-DM1 treatment. Conversely, DHA and T-DM1 treatment induces a severe and irreversible cytotoxic effect, even after treatment interruption, thus, improving the long-term efficacy of T-DM1. These results suggest that DHA increases the effect of T-DM1 as poison for microtubules and supports the clinical development of the combination of DHA and T-DM1 for the treatment of aggressive HER2-overexpressing breast cancer.
-
PD-L1 And What It Means In Cancer Treatement
https://www.whatnext.com/blog/posts/pd-l1-and-what-it-means-in-cancer-treatement
{Not research, per se, but an brief and accessible article about PD-L1, a bit of history of immunotherapy research, and a very brief explanation of how immunotherapy attempts to work.}
-
As of May 2019 TDM-1 is now used for residual disease after neoadjuvant treatment in early stage HER2+ BC.
I did also see a study that TDM-1 (Kadcyla) and Perjeta cuts Risk Reccurance in half compared to Herceptin/Perjeta. I'm not sure if that's for very small/low risk BS where they just give H/P without Chemo.
I am wondering if there isn't any eventual plan to replace TCHP and AC+THP with Kadcyla (instead of Herceptin)
-
I am not aware of any standard protocols for giving H&P without a cytotoxin (chemo). (There may be instances in which physicans moderate or minimize the chemo for particularly frail or intolerant patients. There may have been clinical trials on this.)
Regarding "replace TCHP and AC+THP with Kadcyla," I personally think this would have many advantages; however, a recent clinical trial found that Kadcyla did not provide better outcomes than TCHP, nor was it deemed meaningfully less expensive, so they plan to make patients keep on getting TCHP. This assessment makes a huge error in appreciating patient experience, in my opinion. While "everyone is different" my experience of TCHP was on a different planet vs Kadcyla. Kadcyla was much easier for me to tolerate. Plus there is the issue of hair loss vs. not - which has implications beyond mere vanity. The trial was reported on this board. It would probably show up by searching for Kadcyla for early stage BC or something similar.
I thought AC was only given for TNBC now, but maybe that is not the case.
Thanks.
-
BlueGirl: I'm still catching up from an overwhelming schedule. I know it is very frustrating. Sorry you are dealing with that. I am very disappointed that your/our legislative representatives are so unresponsive. The interview you mentioned sounds just heartbreaking. We all keep plodding along.
-
" am not aware of any standard protocols for giving H&P without a cytotoxin (chemo). (There may be instances in which physicans moderate or minimize the chemo for particularly frail or intolerant patients. There may have been clinical trials on this.)"
I read a post here or maybe on a Facebook group I belong too where the person mentioned her IDC was so small the MO felt she didn't need Chemo, just a year of Herceprin. But honestly I can't recall if this was recent or an older post.
"thought AC was only given for TNBC now, but maybe that is not the case."
I went to 3 MOs (ended up going with the first one). 2 of the 3 told me TCHP. The 3rd gave me the option of TCHP or AC+THP. She said the results were the same but, TCHP had more toxicity. I was planning on doing Cold Capping which doesn't work well with AC+T. Plus the money of doing weekly taxol with Cold Capping would have been too expensive.😁
I'm happy to hear Kadcyla treated you better than TCHP that seems to be the majority sentiment on the Kadcyla thread. I didn't have any awful time with TCHP, tolerated it well but, I'm worried about 14 Cycles of Kadcyla since it's got Chemo in there. I'm hoping for a pCR when I get my surgery so I can avoid Kadcyla but, I'll do it if I have to, no question
-
morrigan_2575: Good luck! Hope all goes well and you have no repeats!
-
-
Lumpie - thank you so much for posting the results from the FAST-Forward trial aka “Hypofractionated Breast Radiotherapy for 1 Week Noninferior to 3 Weeks“. I just emailed my radiation oncologist about it (I’m still going through chemo but plan to start radiation in late July/August). This couldn’t come at a better time for so many given the costs (both real and time-related) and possible COVID-19 exposure from repeated visits to the clinic for radiation.
-
sunandsea: Glad that is helpful. If widely adopted, that treatment option would be huge news for lots of people. Less travel, less time off work, and away from family and other obligations. Less reconstruction - or less going without reconstruction. Many forgo the less invasive option of lumpectomy because of challenges with accessing radiation therapy. We can hope that this may make the entire array of options more accessible to the people who need them. Good luck with your treatment!
-
Off Target: Investigating the Abscopal Effect as a Treatment for Cancer
The abscopal effect occurs when radiation treatment—or another type of local therapy—not only shrinks the targeted tumor but also leads to the shrinkage of untreated tumors elsewhere in the body. Although the precise biological mechanisms responsible for the abscopal effect are still being investigated, the immune system is thought to play an important role.
https://doi.org/10.1186/s13014-016-0693-8. CC BY 4.0.
-
Lumpie,
This is fascinating stuff. I've read about it before, but this is a great article. Thanks for posting!
-
Pyrotinib or lapatinib plus capecitabine for HER2+ metastatic breast cancer (PHOEBE): A randomized phase III trial.
Lillie Shockney's takeaways:
Take-Home Message
- Patients with HER2+ metastatic breast cancer previously treated with trastuzumab and taxanes and/or anthracyclines were randomized to receive pyrotinib or lapatinib, and both arms received concomitant capecitabine. The median progression-free survival (PFS) was 12.5 months in the pyrotinib arm versus 6.8 months in the lapatinib arm (HR, 0.39; P < .0001). Common grade 3+ adverse events included diarrhea and hand–foot syndrome.
- Pyrotinib plus capecitabine was associated with significantly improved PFS compared with lapatinib and capecitabine in patients with pretreated HER2+ metastatic breast cancer.
Citation: J Clin Oncol 38: 2020 (suppl; abstr 1003)
DOI: 10.1200/JCO.2020.38.15_suppl.1003 -
Thanks BevJen, I thought so too. I was just this week looking at radiation as a Tx option so it really caught my attention. Sure would be great if they could pin down a way to get that immune response to it work reliably!
-
Heat excites the Immune system and pushes cancer cells into being recognized by causing them to give off heat shock protein....
-
Lumpie,
Thanks for your posts. I just had a chance to read the one about using radiation. That is very interesting and promising. I wish they could get studies\trials going on some of these findings. It just seems like some of the more promising things happening are still in the labs.
-
Simone, I agree there seems to be a lot 'on the cusp' with promise, which is frustrating. Still other things are pretty well validated but hard to make $$ from so they never receive the gold standard of a double blind clinical trial. So they hover at the edge of breaking through to more widespread use but remain "untested".
Hyperthermia/ aka Heat is a very good immune activator, & is safe to healthy cells in a temp range that hurts cancer. And sometimes it can be self administered. If your lump is right by the surface of your skin, a hot hot water bottle will heat it up. External heat can penetrate into tissue, that's how Vets do it for dogs.
In clinical settings, ultrasounds can bring heat as well or probes or heating the whole body externally or heating the blood and recirculating it, or medically inducing a fever. Whatever the method, if the cancer cells hit 108+ for an hour, they die or get very damaged, giving off heat shock protein, and due to HSP they become recognizable by the immune system. Normal cells are good to about 112. So there is a range of temp safe to us but not cancer.
I did this to the point of magenta boob and armpit (mildly burned but not painful) throughout chemo. It took me about four months to fully go back to normal after chemo but healed perfectly. I think it helped me and it was easy to do while watching TV or chilling.
-
Santabarbarian, Simone80 and others: It can seem discouraging that there is so much promise from bench research but things don't move to the clinical trial phase. As many of you know, Metavivor funds research on metastatic breast cancer. Someone from the organization said within the last week, there are promising proposals, just not enough funding for all of them. Other organizations fund promising research, too. Unfortunately, I am not able to fund much beyond lunch! But I try to do my part with small donations here and there and fundraising and advocacy work where I can. I don't have to tell readers here how important research is. I think if we all do a little, we can accomplish a lot.
-
Important new research from England on DCIS:
Study Gives New Data on Long Term Risks of DCIS
(If that link doesn't work, please speak up and I'll provide another.)
-
"Still other things are pretty well validated but hard to make $$ from so they never receive the gold standard of a double blind clinical trial. So they hover at the edge of breaking through to more widespread use but remain "untested"."
Isn't that the worst part?! 😕
-
Liver Metastases–Directed Therapy in the Management of Oligometastatic Breast Cancer
- This study was designed to evaluate the outcome and toxicity of liver metastasis–directed therapy in the management of oligometastatic breast cancer. The rate of liver progression-free survival (LPFS) was 52.4% at 1 year and 38.8% at 2 years. The number of metastases predicted LPFS while PFS correlated with the use of systemic therapy prior to metastasis-directed therapy.
- Combination liver-directed therapy and systemic therapy resulted in durable disease control in patients with breast cancer and liver metastases.
-
Surgical Intervention for Isolated Breast Cancer Liver Metastasis
- The authors of this study evaluated 148 women with isolated breast cancer liver metastases, comparing outcomes between the 95 patients who underwent intervention (hepatectomy or radiofrequency ablation) and the 53 who did not. After a median follow-up of 36 months, there was no significant difference in progression-free survival between the treatment groups in the overall population. Subgroup analyses suggested a benefit with surgical intervention among patients who received systemic therapy and did not have preoperative progression.
- Hepatic surgery should be considered as a treatment option for select patients with isolated breast cancer liver metastases.
-
this is a better link to the British study on DCIS long term risk of invasive bc posted above by Hopeful82014 https://www.bmj.com/content/369/bmj.m1570
-
New Clue to Anti-PD-L1 Activity in Breast Cancer?
— Survival benefit with durvalumab in patients with PDL1 copy number alteration
A novel biomarker identified a large subgroup of metastatic breast cancer patients who benefited from an immune checkpoint inhibitor....
Almost a fourth of patients with no identified actionable mutations had copy number alteration (CNA) in the PD-L1 gene. Patients without PD-L1 CNA had a median progression-free survival (PFS) of 9 months when treated with the PD-L1 inhibitor durvalumab (Imfinzi), whereas median PFS had yet to be reached in patients whose tumors had copy number gain (three or four copies) or amplification (more than four).
Data for the CNA analysis came from the SAFIR02 Breast Immuno trial...
https://cslide.ctimeetingtech.com/breast2020/attendee/confcal/session/calendar/2020-05-24
https://clinicaltrials.gov/ct2/show/NCT02299999
-
First-Line Pembrolizumab Plus Chemotherapy Improved PFS in PD-L1–Positive mTNBC
Combining pembrolizumab with chemotherapy resulted in significant improvements in progression-free survival compared with chemotherapy alone among women with previously untreated PD-L1–positive metastatic triple-negative breast cancer (TNBC), according to results from the KEYNOTE-355 trial.
Cortes J, Cescon DW, Rugo HS, et al. KEYNOTE-355: Randomized, double-blind, phase III study of pembrolizumab + chemotherapy versus placebo + chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer. Presented at: ASCO20 Virtual Scientific Program. J Clin Oncol. 2020;38(suppl):abstr 1000.
ASCO conference reporting here:
{Seems like there are lots of PD-L1 studies in the news right now!}
-
HCQ Linked to Harm in Cancer Patients
— Combination with azithromycin associated with three-fold risk of mortality, registry study shows
Use of hydroxychloroquine in cancer patients who are also diagnosed with COVID-19 provided no benefits, and may have worsened outcomes, researchers suggested.
Treatment with the combination of hydroxychloroquine and azithromycin to treat COVID-19 in cancer patients was associated with a 2.89-fold greater risk of 30-day mortality than use of neither drug, reported Jeremy Warner, MD, of Vanderbilt University in Nashville, in a late-breaker abstract at the virtual American Society of Clinical Oncology (ASCO) annual meeting.
ASCO conference coverage here:
https://www.medpagetoday.com/meetingcoverage/asco
-
Patient Age, Use of Checkpoint Inhibitors in Cancer Linked to COVID-19 Severity
A study by researchers from the Memorial Sloan Kettering Cancer Center estimated that 40% of the 423 patients with cancer who were symptomatic for SARS-CoV-2 were hospitalized for COVID-19.1 Looking at these patients, the researchers identified several characteristics that conferred risk.
A multivariable analysis showed that patients 65 years or older and those who had been treated with immune checkpoint inhibitors (ICIs) within 90 days of admittance had a higher likelihood for hospitalization and severe disease. ***In contrast, receipt of chemotherapy within 30 days and prior major surgery did not increase the risk of developing the virus.*** {emphasis added}
These data were published online on medRxiv.org. The data were not peer-reviewed, and the results of the study should be considered preliminary.
"Until more extensive studies are available, it is prudent not to alter treatment decisions, but consider SARS-CoV-2 testing for patients initiating or continuing treatment with ICIs irrespective of symptoms."
Robilotti EV, Babady NE, Mead PA, et al. Determinants of severity in cancer patients with COVID-19 illness [preprint published online May 8, 2020]. medRxiv. doi: 10.1101/2020.05.04.20086322
-
Thank you for sharing that Lumpie! it Is so good to have some studies/data about risks and cancer. And of course we owe gratitude for that information to our sisters and brothers who went into this unknown first
-
Study Challenges the Association Between Surgical Margin Size and Breast Cancer Recurrence
Surgical margin size did not appear to be associated with locoregional recurrence for patients with breast cancer who underwent breast-conserving surgery and *neoadjuvant* chemotherapy, a retrospective, single-institution study found. The results were recently reported in BMC Cancer.
Patients with breast cancer who received neoadjuvant chemotherapy between January 2008 and April 2018 were identified from an institutional database.
Lin J, Lin K, Wang Y, Huang L, Chen SL, and Chen D. Association of surgical margins with local recurrence in patients undergoing breast-conserving surgery after neoadjuvant chemotherapy [published online May 20, 2020]. BMC Cancer. doi: 10.1186/s12885-020-06955-6
-
Disconnect Between FDA Approval of Oncology Drugs and Publication of Results of Registration Trials
During 2000 to 2019, no peer-reviewed publication of registration trial results was available for nearly half of oncology drugs granted accelerated approval by the US Food and Drug Administration (FDA) at the time of authorization, according to findings of a retrospective study released as part of the ASCO20 Virtual Scientific Program.1
No systematic investigations have evaluated the timing of oncology drug registration trial publication relative to the approval of these drugs by the FDA.
Although package inserts include data from these studies, "FDA labels can be highly variable in the amount of information that they provide, and they rarely contain the information that is found in published manuscripts, in particular details such as the study protocol [and] inclusion and exclusion criteria,"
In their concluding remarks, the study authors noted that because "trial publications help with adoption of new treatments and mitigation of adverse effects … efforts are needed to ensure trial results are published in a timely manner."
- Khaki AR, Desai A, Schoen MW, et al. Timing of US Food and Drug Administration (FDA) cancer drug approvals relative to publication of clinical trial results. Presented at: ASCO20 Virtual Scientific Program. J Clin Oncol. 2020;38(suppl):abstr 2071.
- HemOnc.org. https://www.hemonc.org/wiki/Main_Page. Accessed May 27, 2020.
-
From the PALLAS trial: Ibrance for early stage hormone receptor positive breast cancer failed to meet the primary endpoint.
-
Machine Learning Algorithm Predicts Financial Burden Due To Cancer Treatment
A machine-learning algorithm was able to predict the rate of financial stress on patients who underwent treatment for their breast cancer, according to a retrospective survey and algorithm-modeling study. These findings were presented during the ASCO 2020 Virtual Scientific Program.
The machine learning algorithm predicted financial burden with a high accuracy (83%), sensitivity (81%), and specificity (82%), and area under the receiver operating curve (0.82)
The study authors concluded that their machine learning model could accurately predict financial difficulties due to treatment of breast cancer. These predictions may aide in the decision-making process and that with careful planning, financial distress may be avoided. As financial toxicity is associated with poorer clinical outcomes, avoiding this stressor would ultimately lead to better quality of care.
Sidey-Gibbons C, Asaad M, Pfob A, Boukovalas S, Lin YL, Offodile. Machine learning algorithms to predict financial toxicity associated with breast cancer treatment. Presented at: ASCO20 Virtual Scientific Program. J Clin Oncol. 2020;38(suppl):abstr 2047.
-
CMS to make some pandemic telehealth waivers permanent
CMS Administrator Seema Verma said use of telehealth has grown dramatically during the pandemic, and some provisions that temporarily expanded access to telehealth during the pandemic will be made permanent. She said the agency is working on rulemaking now.
FDA: Some COVID-19 policies could be here to stay
FDA Commissioner Stephen Hahn said the agency is considering permanently implementing some of the policies and processes adopted in response to the COVID-19 pandemic. Most of the changes "represent an acceleration of where we were headed before," including increased use of telemedicine in clinical trials, support for decentralized clinical studies and work on laboratory-developed tests, Hahn said.
-
Interesting article on how cancers mutate to get around targeted treatments --
https://scienmag.com/revealed-how-cancer-develops-...
-
BevJen, thanks for sharing that article on bc cell mutation and resistance. Very interesting.
-
New Clue to Anti-PD-L1 Activity in Breast Cancer?
— Survival benefit with durvalumab in patients with PDL1 copy number alteration
A novel biomarker identified a large subgroup of metastatic breast cancer patients who benefited from an immune checkpoint inhibitor, according to an exploratory analysis of a prospective clinical trial.
Almost a fourth of patients with no identified actionable mutations had copy number alteration (CNA) in the PD-L1 gene. Patients without PD-L1 CNA had a median progression-free survival (PFS) of 9 months when treated with the PD-L1 inhibitor durvalumab (Imfinzi), whereas median PFS had yet to be reached in patients whose tumors had copy number gain (three or four copies) or amplification (more than four).
"This exploratory translational analysis suggested a higher efficacy of durvalumab as maintenance treatment for patients with PD-L1 copy gain or amplification," Bachelot said in a statement. "PD-L1 copy number alteration could be an important predictive marker for PD-L1 inhibitor efficacy. If confirmed in larger series, this could have important implications for the development of immunotherapy in patients with metastatic breast cancer, enabling us to better identify patients that are sensitive to PD-L1 inhibitors than current testing for PD-L1 positivity on immune cells."
Link to the clinical trial:
https://clinicaltrials.gov/ct2/show/NCT02299999
Primary Source: ESMO Breast Cancer Conference
-
TRAIN-2 Highlights Questions Around the Use of Anthracycline-Based Neoadjuvant Chemotherapy in HER2-Positive Breast Cancer
Long-term follow-up of a phase 3 study showed that anthracycline-based neoadjuvant chemotherapy did not improve event-free survival (EFS) or overall survival (OS) in patients with HER2-positive, nonmetastatic breast cancer compared with a taxane-platinum regimen when trastuzumab and pertuzumab were coadministered with chemotherapy. These findings were presented during the ASCO20 Virtual Scientific Program.
At a median follow-up of 19 months, a previously published analysis of results from 418 patients in this trial showed no difference in the primary study end point of pathologic complete response (pCR) rate when patients treated with an anthracycline (67%) and without an anthracycline (68%) were compared (P =.95).In addition, a significantly higher rate of at least grade 3 febrile neutropenia were observed in the anthracycline-containing arm (10%) compared with the anthracycline-free arm (1%; P =.0001).
References
- Van der Voort A, van Ramshorst MS, van Werkhoven ED, et al. Three-year follow-up of neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2-blockade for HER2-positive breast cancer (TRAIN-2): A randomized phase III trial. ASCO20 Virtual Scientific Program. J Clin Oncol. 2020;38(suppl):abstr 501.
- van Ramshorst MS, van der Voort A, van Werkhoven ED, et al. Neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2 blockade for HER2-positive breast cancer (TRAIN-2): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2018;19:1630-1640.
-
Cancer Care Costs in the United States Are Projected to Exceed $245 Billion by 2030
The national healthcare bill for cancer will exceed $245 billion a year by 2030, a 30% increase from 2015. (American Association for Cancer Research)
The national cancer-attributable costs in the United States are projected to increase by over 30 percent from 2015 to 2030, corresponding to a total cost of over $245 billion, according to a study published in Cancer Epidemiology, Biomarkers & Prevention, a journal of the American Association for Cancer Research.
https://www.aacr.org/about-the-aacr/newsroom/news-...
https://cebp.aacrjournals.org/content/early/2020/0...
DOI: 10.1158/1055-9965.EPI-19-1534
-
Has the Time for At-Home Cancer Care Finally Come?
"...patients have routinely received home treatments using infusion pumps for other conditions, including autoimmune diseases and diabetes. "We asked why this couldn't be a real option for cancer patients, too," ..."The idea of hospital-at-home has been around for years and already has a successful track record."In November 2019, his team got to work creating a model so doctors could prescribe 13 drugs for {cancers for administration} at home.When the program was launched in February 2020, 40 patients signed up. By the beginning of June {2020}, the program had more than 400 patients. "It's skyrocketed," he said. "We scaled that quickly because it became clear that we needed to decrease density in the hospital and infusion suites to have capacity for COVID-19."ReferenceLüthi F, Fucina N, Divorne N, et al. Home care—a safe and attractive alternative to inpatient administration of intensive chemotherapies. Support Care Cancer. 2012;20:575-581.
-
High Medical Costs Associated With Metastatic Breast Cancer
- In this study, the authors used 2003–2014 North Carolina cancer registry data linked with administrative claims to develop an algorithm for identifying patients with breast cancer who progressed to metastatic disease. Medical costs due to metastatic breast cancer were estimated by age group and by phase of care. Monthly costs were significantly higher for women with metastatic breast cancer compared with earlier-stage breast cancer and patients without cancer for all age groups and phases of treatment except for initial treatment among women with stage III disease at diagnosis. The highest expected costs were for women aged 18 to 44 during the continuing phase of care, totaling over $200,000.
- These findings highlight the importance of determining whether the excess costs among younger women and during the continuing and terminal phases of treatment provide high value for these women.
(There is a discussion about cost of care by Lillie D Shockney. It seems to focus on the merits of limiting expensive care in order not to bankrupt the patient rather than addressing why we allow medical care in the US to bankrupt patients in the first place.} -
FDA Approves Pfizer's Oncology Supportive Care Biosimilar, NYVEPRIA™ (pegfilgrastim-apgf)
June 11, 2020 NEW YORK--(BUSINESS WIRE)-- Pfizer Inc. (NYSE: PFE) today announced the United States (U.S.) Food and Drug Administration (FDA) has approved NYVEPRIA™ (pegfilgrastim-apgf), a biosimilar to Neulasta® (pegfilgrastim).1 NYVEPRIA is indicated to decrease the incidence of infection, as manifested by febrile neutropenia, in patients with non-myeloid malignancies receiving myelosuppressive anti-cancer drugs associated with a clinically significant incidence of febrile neutropenia.
https://investors.pfizer.com/investor-news/press-r...
-
New Protocol on Breast Cancer and Breastfeeding
New Rochelle, NY, June 10, 2020—Managing women with breast cancer who are breastfeeding is a complex issue. The Academy of Breastfeeding Medicine presents new recommendations in the peer-reviewed journal Breastfeeding Medicine. Click here to read the article now.
"The aim of this new protocol is to guide clinicians in the delivery of optimal care of breastfeeding women as it relates to breast cancer, from screening to diagnosis, treatment, and survivorship," state coauthors Helen Johnson, MD and Katrina Mitchell, MD.
It addresses the spectrum of care, including oncologic breast surgery, chemotherapy, and adjuvant and endocrine therapy. A section on breastfeeding women who have a previous history of breast cancer is included.
Arthur I. Eidelman, MD, Editor-in-Chief of Breastfeeding Medicine, states: "This protocol is a guide for mothers who are undergoing diagnosis and treatment for breast cancer. It emphasizes that they do not have to categorically give up on their nurturing role as breastfeeding moms."
Breast cancer is the most common malignancy in women worldwide. One in 20 women will develop breast cancer in their lifetime.
https://home.liebertpub.com/news/new-protocol-on-b...
https://www.liebertpub.com/doi/10.1089/bfm.2020.29...
Published Online:9 Jun 2020 https://doi.org/10.1089/bfm.2020.29157.hmj
-
City of Hope - Ultrasound to a kill Cancer Cells (apologies if this has been posted already)
https://www.cityofhope.org/breakthroughs/using-ultrasound-to-kill-cancer-cells -
Olma the links do not work
-
Olma61 - the links did not work for me either. I knew ultrasound was used in detection, but had not heard of using for treatment, so asked Dr. Google. Maybe there is hope
-
Live stream: Chasing Cancer
Stephen M. Hahn, U.S. Food and Drug Administration commissioner, will lay out his agenda for the FDA and discuss critical steps the government is taking to approve innovative, life-saving drugs, therapies, and clinical trials for COVID-19 and cancer. As an oncologist, Hahn has spent his career dedicated to advancing cancer treatment. James P. Allison, the 2018 Nobel Prize winner in Medicine for his immunotherapies at MD Anderson Cancer Center, will discuss the next steps in his ground breaking research, one of the most important advances in cancer treatment in 100 years. We'll also focus on DNA and genetic testing, groundbreaking immunotherapies and drugs that topline researchers hope will combat the deadliest cancers.
In a segment presented by Pfizer, Andy Schmeltz, global president & general manager of Pfizer's Oncology division will discuss the challenges, barriers, and inequities within the current healthcare system, and what we can do to fix it.
Join us on Wednesday, June 17 at 10:30 a.m. ET.
Stream here: wapo.st/chasingcancerjune
https://chasingcancerjune.splashthat.com/?utm_medi...
-
Hi ladies, sorry about the broken link I edited the post just now to fix it and here is the correct link to the City of Hope article:
https://www.cityofhope.org/breakthroughs/using-ultrasound-to-kill-cancer-cells
Good to see those other links too!
-
Lumpie -
Thanks for posting the Post talk -- that sounds like a good one. And they've got two good people -- I've heard interviews with Allison before and they were fascinating.
-
Study Finds Wide Variation in the Natural History of Untreated ER-Positive, HER2-Negative Invasive Breast Cancer Tumors
Results of a retrospective study evaluating multiple characteristics of a cohort of individuals with untreated estrogen receptor-positive, HER2-negative invasive breast cancers showed a broad range of tumor growth velocities across patients. This study examined the in-vivo tumor growth kinetics for patients presenting with "missed" ER-positive, HER2-negative invasive breast cancer that had been present, but unidentified, on 1 or more previous serial screening mammographic images performed at least 6 months prior to the diagnosis of breast cancer. Changes in tumor volume over time (ie, tumor growth velocity) and tumor doubling time were estimated for these tumors.The study authors noted that these results "demonstrated a variation of in-vivo growth kinetics in an untreated subset of breast cancers and found that the volume change over time could not be predicted."
They further commented that these results show that more difficult-to-measure factors such as host immune response, tumor microenvironment, and molecular heterogeneity may play a larger role than solely tumor subtype.
https://www.cancertherapyadvisor.com/home/cancer-t...
Reference
Rojas KE, M D-M, Rojas M, et al. The natural history of untreated estrogen receptor-positive, Her2-negative invasive breast cancer. Breast Cancer Res Treat [published online May 12, 2020]. doi: 10.1007/s10549-020-05666-7
-
The Chasing Cancer Postponed until June 24th. IF you register, they will send reminder https://chasingcancerjune24.splashthat.com/
-
Probably something about "driving" genes: http://news.mit.edu/2020/counting-your-antigens-cancer-immunotherapy-0602. One can see targeted/immunotherapy treatment revolution is not far away...
-
BSandra, this is very exciting! That "grad student" must be something! Thanks for posting.
-
I'm not sure how I found this subscription or who recommended it (probably someone on this string), but it is excellent. I'm sorry if it's fuzzy. It seems to originate from "Practice Update":
<img src="data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAACdkAAA0ACAYAAACCFYfUAAAgAElEQVR4AezdibdU1b3u/fun3DvGuSN535z7Ju/ISWPOyTUnjSYx5pjGaByaRI9R1NhEpFNERCQ2KCA2CGIbrxpjh4pdoiAqJAjY00qjHFEaBRWQ3c13PJUx650192+1tapqbfiuMfao2rWr1prrM+eaq3Q+zPnfHBsCCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCJgC/818lRcRQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQMARsqMRIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIJAgQMguAYaXEUAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEECBkRxtAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAIEGAkF0CDC8jgAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAgggQMiONoAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIBAggAhuwQYXkYAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEECAkB1tAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAIEEAUJ2CTC8jAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAAhO9oAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAgkChOwSYHgZAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAUJ2tAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEgQI2SXA8DICCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAAChOxoAwgggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggkCBCyS4DhZQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQI2dEGEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEgQIGSXAMPLCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCBCyow0ggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAgggkCBAyC4BhpcRQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQIGRHG0AAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAgQYCQXQIMLyOAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCBAyI42gAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggECCACG7BBheRgABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQICQHW0AAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAgQQBQnYJMLyMAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAACE72gACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCQKE7BJgeBkBBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABQna0AQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQSBAjZJcDwMgIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAKE7GgDCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCQIELJLgOFlBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBAjZ1bAN7N+/3z38yAL3u7PPdVdeebXbsuWdGpaSIiHQO4E9e/a4O+68y40adaa7+eZ5bseOHb0rDEdGAIERLUB/MqKrj8IfogJ9fX1u7bp17k/3/9ldceVV7pcnnOj+45ifNn8mTpzk5t0y3y1fvtzpGmdDAIFDS0DX/bZt29yWLVvc22+/zc8INFDdqQ7pww+ta5ezRQABBBBAAAEEEEAAAQQQQAABBBBAoO4CtQ3Z3fen+91//x//1PGff/23w9369Rta6unDDz90x/zkZy3H1gBeN7a9e/e680ePaTn2F7/0ZffCiy924/BtHWPhwidayq36u2TyFNc/MNDWfj/99FP329NGtez7y//yNffGG2+2td/PPvtsmPU//c/Pu2XL/tbWfkfyh3vZ9vO6ffDBdnfc8Se0tId///b3GoPtefdR9/epDSb1f1OnTmv7mso6/0WLFjtdC1YZ1DezIXCwCBzs/UlaX2Jd3/Fr3/zf32rcJ5988in38ccfHyzVznmMUAH9I5S/Pvtc4zvh5z7/BfMeFbdh//vRRx/TCOTt3btvhJ49xUYAgTwCuldt3ryZUN0IDNWlhSFVp3wPyXMF8B4EEEAAAQQQQAABBBBAAAEEEEAAAQQQ6LQAIbuaheysoJoGCDVjlwJ4dd4UVlRo0Q9o6vHnPz/OffTR7raKvXr1ave1r3+jZb/a9513/bGt/W7b9r774VFHt+xXv+v1Q3UbCSG762+4saXOfHvrRvisW+0iLRjz3e8d6d55592OFeXAgQNu7NjxprGsCdl1jJ4d90DgYO9P0voS33fmfVTgX16ElHrQUA/xQypcpxnrDvvGNxPvTXnb8Ve+epibO+8W2vEh3qY4/YNTYOfOnYTrDrJwXRy8Ux2zIYAAAggggAACCCCAAAIIIIAAAggggAACvRQgZFezkJ1mzLMGCjWzngJQdd46NeNc0qyG5577e7dvX/kZSbSEWDxb1/gJFzktQXaobnUP2am+Ve/WNdJue6hTnWcFYxYseLRjxbXCsqE3IbuO0bPjLgscCv1JVl8SXtt5nx9xxA/cq6++2uXa4nCHosDQ0JBbuXKVU5vL2z7zvk/71L51DDYEEBj5AgTsDp0lcQnajfzrlTNAAAEEEEAAAQQQQAABBBBAAAEEEEBgJAsQsqtZyC4pUHbiSb92e/bsqX1bs2YFevDBh0qXO21WrXZn9Lr11tuHDdrqtUN5q3vIToPhV101fVi9aVD9YApIZgVjOjmzpWaITAsp1D1kV/c2XKf+JQ51j4Qwd+gX3y+t5d/D98fPD4X+JKsvSbvW0/42Upaxj+uc39MF6tR/6vvfnDlzh/1jiLhdatnYo37048ayxtfOmOn0o77tlyec6DRrXfz+8Hd9VjPkDQ4OpsPwVwQQqLWAlhGNZzzj94M7dMfSsbW+JCkcAggggAACCCCAAAIIIIAAAggggAACB7VAbUN2Wg7xhRdezPVz+bQrWgbRvvwvX2ssaZjn80uXLnOffPJJSyX3cpDxvffeawwWhoOAmm3tgQcebCljXX/RgH48O9wlk6e4/oGBUkVWO1CYLvQIn//12edK7Vez1SmUFe7rC//8Rbdq1Sul9newfKiXbT+v4euvvzFs+WAFPtT2DpYtKxjTqbaqpZ1POOGklusivEb0nJDdwdLKXCOIEtbvoRayU00e7P2J1ZfcMv/WXN+t9B1KwfNjf3G82Sf8+7e/59auW3fwXBCcSWPGZPUDYb+gwFq3t71797px4ya0lCMsk5aNnTnzOrdx48bU75cK0r7//gfu3nvvc4d/6zvm/vSdde7cean76fb5czwEEMgvoOt88+bNhOwO8mVi49Ck6lx1z4YAAggggAACCCCAAAIIIIAAAggggAACCHRboLYhuyIQ7c5mEx+r10GjrVu3ujPOOKsRVtMgtgJ2ZUNq8bl1+vdt2953Pzzq6JaBzJ///Din8E6ZTSG6cGA1fj516rRSNlY5f/qzY92uXbvKFPOg+Uyv235eyNdef70ZBjv66GPc4sXPH1QDLVYwJm77s6+/ofJz1nHjkGx8XEJ2eVtp/d93qM9k52voYO5PrL5ErxXZNIidtGTnwbRMdxGTg/W9dfgOoIDd+aPHmN/9NDOd7kH79+8vXAWaGU+z1lmz2+m+98wzfym8Tz6AQG8FhtzQ4H7nBj5xQ/17OvqjY7jBfc4N9fX2lI2ja6b3OIDF7wf3LHa+fkfCLP9Gk+UlBBBAAAEEEEAAAQQQQAABBBBAAAEEEBjhAoTsjAqswyCjUawR8ZI1Q5xmFnzjjTcLl1/BQs2CF4d8wt/LBuM0Y51mAwv31c6Me4VPrqYfoO3Xo2LiYIzaqsKEYXs9+sc/aczQU1WJdb0ptBoe4/DDv+30E75GyK4q8d7vh5Bd7+ug0yWI+xJdy0VDdr6MmrVOwf+wP1Df9MKLL/q38DjCBXr9HUD3IS33GrYx/1zBux07drQtvGnTJqd//OH3q8fp18xwCuGxITCSBBSwG9jxtOvfdJ3rWz+1gz+Xu75Ns13/e392gx+/5pyr1/LK27ZtI2R3iM1i50N2qns2BBBAAAEEEEAAAQQQQAABBBBAAAEEEECg2wKE7AzxXg8yGkUaUS/FMwtqAHPhwicKn4NmlVOILhwIPX3UmS1LhZZdNvOee+5t2W/ZMhY+qZp/gLZfjwqKgzH/+m+HN5a7i4OhZZdLts5y85YtwwI0N910s9NMVeE1SMjO0huZrxGyG5n1VqTUcV+ia7lsyE7H1ayhcT9UdkbZIufBe7sj0OvvAJq5OZ5NVb9radgqQ3AffLDdnfSr3zSONWvW7FIzInenRjgKAikCQwNuaP9W1//uHa5v7SR3YPXYzv2suegfIb7NN7mBnX91QwN7nXP1WKpzy5YthOwO0ZCd6p4NAQQQQAABBBBAAAEEEEAAAQQQQAABBBDotgAhO0O814OMRpFG1EuatU6z14XBnDKzxCkIEA62ap967benjWrZ96233l7Ix5ptTyGm9es3FNrPwfhm2n49ajUOxqh9vvLKq27UqDNb2v7YseMrCx7E4VjNWLV69WpCdvVoEh0pBSG7jrDWaqdxX9JuyE5Lecb90Ikn/dqxZFutqr10YXr5HWDDhreHBb3VXjWznWa4q3pT0E73vU7su+qysj8EkgUG3eDula7/nbnuwOrxnQvZ+QDfmotc/8YZbnD3y871f5xcrC7+xc9qxuOhsURsXM9dbGocCgEEEEAAAQQQQAABBBBAAAEEEEAAAQQQaAgQsjMaQi8HGY3ijLiXNNiuQfcwZFd0EH5oaMjNvv4Gcx/X33Bjy+sa8NfAf95t586dTktthuVTcO/TTz/Nu4uD9n20/XpUbRyM8SHQBQsebWm3X/v6NxpBuHZLbQVnxk+4yCmEEC+rx0x27WrX5/OE7OpTF50qSdyXtBuyUzkVbA/vn9/93pHunXfe7dQpsN8uCvTqO4CCbpdOuaylXamNaYnYIt/vukjFoRCoj8DAp25g12LX9/bVnQ/ZKWy35kLXv2WOG/zkLecG9/fcIQ5d1eX3O++805122mmNn4ULFzLbXodm2+t5A6QACCCAAAIIIIAAAggggAACCCCAAAIIIHDICRCyM6o87yCjBgXXrFnj5syZ604++VT3H8f8tPGjQcF5t8xv/K1XM2RoUFKD6wqkKYTmy6Zyzp59Q+NvnRq4VEDuqqumtwyWahY6zXCXd7OCetqn9q3zCme48wGkvPteteqVYcvdyanIptnwtB/Vc+j7yxNOdNOnX+u0jOdHH+0ussvc7x0cHGwEGv50/5/dxImTmnWrOtbvel2BB72v6Ja37Rfd70h4v7+e4zrV9XzHnXe5devWd23GmzgY46+f99//YFhAtOhMjlZdvLxiRcs1oetr0aLFzmoP7YTsfL+kPijsM6vsl6wyK0xWxaZresmSF4b1q7rudQwti71t27ZS155VPu/VqX68UyE79Y+vvfZa47qx+ihdT2vXrXN6XztbPPti0XtBO8dO+mzYP0+5bGojpOrvv7pXqH9Zvnx514JDcV9SRciuE+7bt293WipU/a33Utt5+ulncs/W2Yv7sr6TqF9+5pm/uBkzZw3r1/Savg/s2rWr8f0lqd0UeV39kPYZH8+3L303KXttdbL/TDtHzZqq0HgY3jzqRz927733XtrHevq3bt8PrJNVGZ588ikX9jWd/h6adF9SIF/lePTRx0p/B7XOUa+F/ap1T2nne2/SMePX9+/f37j/Xz7tima/rmtO9zNd373ehj573w1sf8L1aVnX1eO6Erbrf+9+N7h3k3NDxf97o0qvoqG6V155xV1wwQWN8NuUKVPcW2+91ZEAHCG77sysV2VbYl8IIIAAAggggAACCCCAAAIIIIAAAggggEAeAUJ2hlLWIOOBAwfcIwsedYd/6zstA4Lh4KB/ftg3vunuv/+B3IPEKk47wYctW95x48ZNcJ/7/Bcyy6b36L36TNWbBoC9gX9UACXvFi85q9CPwgLatm173/3wqKNb9l9k33FAINx3Vvl27NjRCNF98Utfbjm+P8f48YQTTnJLly6rJHTj292R3z8q17HV9u6++x63d+++rNNq/j2r7TffmPJEYTUt7xZbyFkDoQoltLPt27dv2BKm5577e6fXrc06pzAo5l3zXM96z3PPLaqkPq2y+teSgjFWgFVtTAPtZbe0fWbZ5T1mkX5J7eSMM85ya9euzWwrVvnidpf1e9gWrPPR4P7f/77cnXb6GS3h3rT96hrVPUJtq8xWxCtvPx7fV9LKb/0t7Rrz5/juu1sb96+8/aPep1Cy+tWsLe63rTKmvXbMT37WCI3Gxynan8Sf978rgPHQw4+4vP1z3nrz+y/7mNSXlN2fPldkJjvrGg2vOdX9pEmTE6+tpHoLy9+L+7Ku7b/85a/u2F8cP+xel9QO9d7nn19S6v6hfvr119/I3Q/lubasukkqe9LrYV2GdVLkub4zTJ06bZhjFfsuUo487+3W/SDu7+LrQPeIC8aMTbxufH3pfqrrK08fm3b+an+bNm3K/d8XOn6790GVx38/y9uvlvneq+PE98fwfqcy6LvrV7562LA26p39f5+kGXb8b0MDbmjfZtf/7m2NoN0Bv7xrBx/71l7iBj543A31fdjx00s7ACG77oTZijp36/1pbYO/IYAAAggggAACCCCAAAIIIIAAAggggAACnRAgZGeoWgOPfraorVu3ulNOOTVxoMUPuMSPmp3lww8/Mo42/KV4sCceXBv+iX8MRM2dd0uucF1cNg3267NlAyFWedav3+A0q1B4LM3+oIG6PFs8iK/lXTVbjDYNyF4yeUrLvvW7Xs/aNLuLlsEMy5VnqTsNrD78yILUQbZwn/Fz1X87g5ya9anIYH54/COO+IFbuXJVLnur7as95t1UB7NmzR428FtVwE7lKBqKsc7JD95rxj+F1EKvPM8nXzqlozNRpQVjkmady1tH8fus2fHuvOuPjbel2cX7sX5Xn1K2X1KbUdtLC4la5ctTf+F7fFuwyq/+XuG68P1Fnuua1bWbd2vHK6sfj+8rRc5D7w1DB/H5KGCm2fZUhqL71fsVXlD/qn42aYtDJ0WPk3QfLdqfxOXTPe1vf/t7rtC9VeaseouPV/T3tL6k6L70fs1ipdmbwnNJWw7eukb9Nafwavw9IdyvnifVm8rSq/vya6+/Xvp+rHM686yzm99n8tTBJ5980lhKVX1i7JP1e9q1ZdVN1v7iv/u6zHMeSe+x7kHthseTjtXO6928H8T9nb8O9B1L/3iiaF+r60zXW5mtnfan9lL0PujL2K3vvTpefH/097udO3e63542KvO6q0XITicysM8NfrLG9W2c0aWg3TjX9/Y1bmDnX93Q4AHncv43nq/jqh6LhrmYye7gCuVV1Y7YDwIIIIAAAggggAACCCCAAAIIIIAAAgggkFeAkJ0hZQ08asDr7bc3NpYxiwcZ8/6uoJUGqLO2eLDHD64lfU6DbtbMYXnL5d+nWe3ylC+pHOHrn3766bCBqbSB+PCzVughDtFp5jpfbj3+9GfH5lquSUs66b3hZ/1gWliG8LkCJNP+cEXLZ8LP532usJuWHC2yKcCh5fLyzgyVVBYNyGopvqyQo9X21R7zbN0I2KkcVvtIq0PrnHQ9awD337/9vdL1qllkVJZObGnBGCvkEl8fRcq0YMGjLQbhkptJdnn2r1Dx2eec17LvpPaZ9vpJv/qN++CD7eYhrfKl7cv6W1JIREsuttM+/LHyhhs63Y/H9xVfvryPSddYVfWsANHcufMSw9Jx6CRvuf37ku6jRfuTsCGqzlTmMuEnXy7/OGbMOKcwS9VbWl9S5liLFz/fsrS0yu+Xcrf2Z12jRfrfpHrrxX25qvuxzLQkrr5TZm3q7/Xd0beTMo9qnwq/q72Gm1U3Rfef1H+Gx8l6bs187IPeWZ/t1t+7fT+I+ztdB7oPtvNdX98ji4bB2v3vHt+eFPbUUutZ30FVn1VdZ3m/9+qY8f1R9zsF7PJee0VdO9duh5wb3OcGdi12B96e7g50Y9nYNRe6vs03uME9q/4RtOvcySXumZDdwRWaK1qfiQ2DPyCAAAIIIIAAAggggAACCCCAAAIIIIAAAh0SIGRnwFoDjzfddLNT2MMPGOlRA5ea1U7LCL3wwotOA4UzZs5KXS7u9tvvyBxkigd7kgaZfdEVnrIG+TXApBkY7rjzrkb5VEY912tJs2BoAC8eiPXHKfqomY1CLy3jlGdWJ2sWvHg52Pg9Ov88g1zxMrQqn5+l0Dq/tOCLr//QV21h4sRJiTPeKbSTx8CX5YUXX0wM2Gn5LLU3tTvV7ZNPPtVYevHoo49pcfd1oPJmLddqtf08IbuksImOee99f0qdocqfa97HoqEY65yuu+76YTPYaQD6ookXu0cffazpqdkXk4JWOjdde53YsoIxcTBOZdy8ZUvholiWY8eOb85qadnlCVWkBUPU92gA2/ebvl867/ejE9v6ccefYAbtrPL59p730TqftACm2onKGl73Wf1qnuu+0/14fF/J6+PfZ4Xs0upZ18cvTzjRzZ59Q7OP0rWV1j+m9VFx6MSXK+9j0n3Uugasc40vLvV51qydvjyqc/Uf6pfD7wdJ/bM+lzeIH5cl7fesviTts/HfrOtC14NmSk3arGtUs1vmnSHSqrde3ZfT7scKEalt+35NYcQ5c+Y2rgG1a98uwsekfs1b+jYWfsY/9/1Q3uNZ15ZVN37/eR+t/tOXP+/j9GtmtPh8+V++5vRdrS6b1e69j6+Hqu8HcX+n6+DGm+YM+66vWeLUztTe/L007Tu+ZghUeCzPpn8Uon8c4s81fLT++0JtMe0+LitdQ1lb2nXWie+9Kk98f9Q/EIj/GyY8//h5nv/+yDrvyv4+NOiG+ve4/vcfcn3rL3fdWDb2wNpJrm/LXDe0b4tzmtGuy1vRUBYz2XU2lPfiiy+6GTNmuDfeeMPlqRu9T+/X5/K8P35Pl5sbh0MAAQQQQAABBBBAAAEEEEAAAQQQQAABBBwhO6MRWAOPX/jnL7YMNGmAeMuWd4xP/2MJs+Uvv2wOTuUJw8SDPdYgsz+wtcyWBn8UFkpbnvTjjz9uDCrFg79ZA+b+uHkeNegU7z8Oy1n7iWeps5ZztWbz0oBY1hYPXKpeNUOJtWk2DQ0axueg3ydNmpy63JuWfVSgRAPv8WCcBu9U/qwtaWBXg6oKNSQtrahyv/XW6mEhMpVDs2qtXbs28dBW288K2SkIoFlnLKeqA3YqeNFQjHVO4fWscit0l7QsqZyfe26RuRxkuIxxImqJP2QFY7TMra6LsG2Vmfln9erV7mtf/0ZzP7JYtGhxs8SWXVaoIikAo0F5XaPqe5I21cH8+beZIWDNlqV9h5vq5qOPdjuV0/9s3LjRxUEmLe/r/x4/qj2Fm8pgzcCna1nnrhm0kjZ9VudohZgvvGhiM7wYf74b/bhmF43PXS5hG5Kb/OL36fc9e/YMC4jr+g4/r+d5+se0a0qhDiswqnqKy6XQenh8BblXrFg57H36nNqJ1WcW7U9Ud0n3BpVF/fPSpcvMY/nPbtq0KTFkJlPtv6otqy/Jc5y0+soK5ste32HCevrOd49ouV/o2lJIadu2bU031Yv6J4XgVXd+S7LP0+7auS9v377d/eznv2g5D53T4d/6TiNEGvdNvrx61HcxfWdQGUMHPVdwKqm+4/5Z79c+0u5XOp76E2sGrvja6kT/GZ53nufW9ffznx/XUud59tOp9/TifqBzib+rqt7/r//7fzXbj2ZCfPXVVxPbTlqby/NdQbPmKQQat1fd2xQu1nWdtOkeqfJb339Vt2qfSVsvvveqLPF/d339sH91Cnv685e//rtK12RfX1+j+Lrm33vvPXfvvfe5119/I+mUevb60L5Nrv+//o/rW3Nhd4J2aya6gfcfdEOfvefcUPLS750AiUNXWb8TsutcyG7ZsmVuzJgx7rTTTnNTpkzJDNopYKf36f36nD6fVX/x3zvRptgnAggggAACCCCAAAIIIIAAAggggN4DRjsAACAASURBVAACCCCQJkDIztCxBoX9QIseNeuGBmuzNg2+WINUWQNc8WBPWsjOWmbLCqNYZdUAqwb0w4Ffzcyngbsqtm3b3nc/POro5iCV7DSzT9KAso6pwavxEy5q+UzSrEIafA/rRbN3KEiStGlATMtqhp9JW2ZWg2ZhAEmfk1WR4JjCUBpUDI+p51lBJQWRrJl+NEtI3iUFk5bTS/KUm9X200J2Mu1mwE5ltAbli56Trw+FSrUcb1qb9O0pafA3T3DU7yPvY1YwRu5Tp05raVdZ7T8+ts559vU3tOxDs9yEgRarPWS1XfVJYZ8iazlrpp08ziqntTSfgpF5ZsGxypzWhmMX/a4lUDWg7tuJZjFVf553+/vflzcCrf7zelT5X16xwtxFr/rxIvcaq+Bqhwoiq351jgpV5F0SUPvTjEpqt6GTnqtd5mkrcRAlXOrYKq/1WtH+RPvYsOFtc4bLSZdcmrt/1ncIzUAVXytxEMoqc5HXrL7klvm3Nma90sxXaT+6Zm+48abE2XnzzLxnXY9hfSvQmvYPAuJz7eV9eevWrY3Zi335iyzxq/asGUj9teL3kfYPL+LvOPpM3hCm2lc4Q5zamZY4twKsobFVX0X7z3B/Wc+t4+k7oA8yZX2+G3/v9v1A5xT3bb696FHXjMqUtal/tpaXPfGkXzdC00mf1+cUpAuPqefqX9Wf5OmbtW99Z1IYMN5PUrC0V997Vdb4XhiWWdeowtt5zzvJteuvD/U3lnDt23xjd0J2Wpp27cVuYNci5/qSQ5idcIhDV1m/5wnZaWY1Bb8uuOACp/frZ86cOe73v/994/XTTz/dTZgwwS1YsMBt2LDBDIbdeeedjfdqPwsXLnSrVq1ys2bNcmeffXbufYTnouM88cQTbvLkye6MM85o7EOPF154oXvwwQfdmjVrzHIsX77cnX/++Y33K8i2YsUK83233HJLs7x6Hh47z3OVb968eU42Omf9XHbZZe6tt94y96XX9Xf/Xn1On0/yTCpDJ9oU+0QAAQQQQAABBBBAAAEEEEAAAQQQQAABBNIECNkZOtagnx9wuXTKZcNmUzJ20XxJoZBw1iztJy0QpA/Ggz1pIbt4IK7oMlsaiFWYRIOvmuGsykEkKzCXNbhnBfOSQj0K4oS2WQELhYfiwJtCdxpQjDe5aOYpX+961CC1AiVFjaxwVtYMaI8/vnBY+CJPoCE+D2s5R51HOFtZ+Bmr7ScNsFshTe+k4J3lGh6r7POioRjrnHw5i9anVS9Jbajs+elzVjBGr4WbAlth+08LcYWf88937drlFDIN23g8G6Rll3Q9ar+6xuJltRUqyROO8+Xyj9aScaNGnZk5C6RV5qQ27I9lPar9qn38+jenmEvVWp8JX7PChgpAW/1Hr/rxIvea8Nzi56+9/nojUF6mnhVePOpHP25ph2nh5/DYsVvWPSD8rH9etD+x7g26hsr0z2pjVggmb8jQn0Pao9WXhNd82ec63zxBH+t69McsambZd/O+LGeF17UE8ugLxmb2RXG96NqPZ1+URVKfGl+f+kcL+o6Ud1N/fPLJp7o/XHGle/fdrbk+ZtVXmf4z18Gca8ycefjh3265/jt5vLzlit/XzfuBjh33bf6ayVpiOC63dU/O+u8EzZQch0HL3set779JwVLr+1XRPkLnX/R7rz4TX2veW2XVOYzUbahvtxv88CXXt36q61szvithu/5NM93gR0udG0ye9bdqz6TwVdLrRUN2CrCdd955zTCYD4X5x+uuu86tW7duWJAsDNnNnDmzGa7znwsfr7rqqsQwms5DAb1LLrkksQza1/jx4xNngrvvvvua4bebbrppWFkXL17cLN/FF1+cOQNdkq0cZs+e3TyWymUF7ayAnT5nOSYdy79edXtifwgggAACCCCAAAIIIIAAAggggAACCCCAQJYAITtDyBpk1ICLggBFZjPSrjWzWjxTT9ZAaTzYUyRkp+Xyig4IdSoMpfOPBwqzQhAKf2nQ3A9waSY5Lc9kbVZIKGmwWp9/4403W5Z/0jGSZiGzlmnLu8xrXNakgXXNamNt1lK4cktb5tXaj3/Nmvln7Njx5myMVtu3Brx7FbDTORUNxVjnpLrXTIFpS5d6v/DRanNFZ5AL95f03ArGxCE7q51odru813Oea82yS7vG4n3KOe/MmrGFzkOhZt8X6DFPkNAqs9WG4+Ml/Z7XM/681U6T2krcT3arHy9yr4nPL/5dfYIVIIzfZ/0en39WCMTvI/5c1v3Ffy58tOopLQhv3RuKBl/C44chQy01q5k105YkDj+b57nVl4TXVNHnMn72ueeay7pmlcG6HnXMMt+nLPtu3ZfD81Q7V3svs2nZ2V8c98uWfi0pqB1fnwrna/bHIlvR/suqr3b6z6yyrl+/Ydisn/fcc2/Wx3r296KevqBWP5N0P9Bn4r5N14y+Gyu8XXSz9pW0H51fPEtu2SCryhl+/1VQT21py5Z3ht0rrO8z3freq3LG11o73kXrp7PvH3LuwAdu4IPH3IG1l7gDmm1u9dgO/0xw/e/Md4Mfv9a1ZWN92CrvY5GQnWZXGzVqlDvrrLPcjTfe6J588snGj57rNYXINJvc008/PSy4Fobs9D6/D733mWeecbfddps755xzmsE5K/ymc3rttdfcxIkTG+9TeaZOneqeeuqpxux6ixYtcldccUUz1DZu3DhzpjrNcveHP/yhsQ+V49lnn22WN+1veU3D92UF7aoM2Om4bAgggAACCCCAAAIIIIAAAggggAACCCCAQLcFCNkZ4tYgowZcspZ5NXbVeEmzQ+nz/icrCBAP9qSF7B588KHmfv3+NaBWl61IsE2DcQrk+PPQY9ogpDUYmLbMWGyVVg9xneUJ96SZWzP0JZU1nqFPDu3MbCSneJnc737vSKelbOPNavvxALvqSTN8hWFIlVG/d3IGO19Wa7A6LRRjnZPKmjSbnz+O9WjNzph2fVr7yPOaFYyJQ3baTzx4nhXg9cfWjFAKWobXmhW8tOyS+hfLJmnGGl+OrEer/4hn24v3YZU5bsPxZzr1e976ifsm1UuSc5VlLXKvqfK48b6soE1SCCT8bOyb1qeHnwufF+lP1PfFSyyrL8lT1vCY8fMXX3qp8plk/TGsviS87os+/9znv+DGjZvgNm3aNCwo448ZPlrXo45Z5vtUL+/L4Tm187zI95xwuVeZ6XtImdkii5TXqq9O9p/Wtd+Nvq+ISVXvjfurtPt1/F7Vf56ZXK2yWt8pk4y1nLDu22G/UOYfJITlUJt66qmn3d69+8KXW55bZezW914VJL4XtuPdcmJ1+GWwzw199l4j+NbXCNp1OmQ31vWtm+z6t/6xcVw3NHy28KpZwoBXnudFQnYKx2mJ1WXLljVDaf4YWipWATy9R6E7/7p/DEN2SfvQ0q0Kxmkf5557rlu6dOmw/Sh8p78rYHfHHXeYy6neddddzaDd1Vdfbc4Ip337GfkU1PPLuD700EPNzyYF/fw55X1U0E4z/Knc/ufyyy93K1eudHr0r+kxaSbAvMequj2xPwQQQAABBBBAAAEEEEAAAQQQQAABBBBAIEuAkJ0hZA0ythMWsQbLrMCML0o82JMW4rFmdvnKVw9zf/nLX3MNgPtjdupxz549TkvEhgN2SUsmWrOEZQVqFG4I9500aGkFzZICfFaZk96b1806flJZ4yBB3lmd0soSO8nMCoZYbT8cYO91wE7nWCQUo/db55Rkn2bo/xZfn2WCPX5fSY9WMMbqM6wB8aQZEsNjxcGGpNChZZc0OK/QpsKb4fWYNENTWJa059ZMoFnXolXmsA2nHa/qv8X1mNRWetWPx2057V5TtU24P6vOktpZ+Ln43prkG34mfl6kP7HuDaf852+dXq/rFrfB8Pps57n6DC2bmjXrnlW3Zb5PWfZZfUFWnRS5L2ftq8jf43abdN1ZM4MeccQP3KuvvlrkcIXea9VXJ/vP+F6kNpnn2i90UjV5c3wtpvVXcRuRy6233l7qTCzjpDrV7M5xv6DZNTu99fJ7r84tvhfKIM93qU67VLb/oT43+PGrTku5dn4mu3+E+PrWT2vMoDc0kByurOr88oax/PuKhOwUotOscf6z4ePrr7/uJkyY0AiMaUlUfZcL/x6G7B544IGWv4Xve+SRR5ohN30m/NvLL7/sRo8e3TjGlClTmsG48D16rlCbwnUKrWmmOi3/Gr9Hv//xj39sHEuBPYXrtAytlpnV53QumjXP+lyZ16yg3Zlnntk4lg/ZtRuwU7nYEEAAAQQQQAABBBBAAAEEEEAAAQQQQACBbgsQsjPErUHG3519buosDMZumi9p5pF40MoKzPgPxIM9SQOwer9mpLrwoonD9q/jnXLKqW7p0mVOM0z1arNmbVHozgolxDNZaNYWvZa2xcEeDfxbttYAfVKAb+PGje7ww7/dYpr03rSyxX/TEmhhO7DCc5999pk7f/SYlvclecX7T/tdSwhrCcrw+NaArdX2/WBsWsBu7tx5uZcpTStnnr8VCcVof9Y5yVjWZbZ48DttoLzM/vWZeDBe9Wa1a4VE4qXd8sx2o1mkwrbw058d6xRyjTfLLikAsXz58mGzGyYtxxwfJ+l3tbnLp13RUtasgKRVZt+Gk46T9brK8f77H7gHHniwMZvQd757REuZFGz+5QknuhkzZ7mXV6xo9rlxPSa1lV7140XuNVlG/u9a9m/Jkhcas2dqSVDNfObbmp7rtYkTJ7knn3zKffTR7sbHrDpLamf+OHqs4los0p/k7UfDMvb6edwGk/qSpHJqWdRt27Y1Zp6L7yHal2a1U50nbVbdlvk+1cv7ctK5yUbfQXQvPfnkU903//e3mm1dNvpdr8+ZM9dpOT7119ridpv0HU/Xx0m/+k3LPrVffc+5YMxY9+abbzX3mVTGoq9b9dVu/5lWBqteO3m8tLLk/Vun7wcqR9xGVOe6x5bZ8tZpmfttmfLEn+n1916VJ74XllmyPT6vWv1OyK4lOFYkZHf22We7JUuWtHzeB840E5yCbwqMWQG4MGS3cOFCcx/al4JuF1xwQWM/06ZNa8xs64+hIJwPpOm5f916VBjQz6x39913m+9VmTWLnfap2fX8ErJJS95axynymhW08+cza9asxr2xyP6s99bqWqMwCCCAAAIIIIAAAggggAACCCCAAAIIIHBICBCyM6o574CU8VHzpaKD3PFgT9IArD+YBv7j5Z00EOt/NDinEM0t8291em+3Q3fxLGpJQZN4Jouk4I8/bz1aAQlrpjxr2UlrJjft06ovDZb/xzE/besnHoBX/ehY4Wa1vS9+6cvu6B//pK1jH/n9o4YFoKyBbOv4ep8GXxUwCgMzvn39+jenuN27/xGWCc+lU8+tOi+6XKx17nnLGw9+J7XnvPuz3me1wbit+M8p1KVAqq8PK7zp36tHBTdOOOGk5vv1uaRl2az2oPO3tthF+1UYrd3rRgE2f256zPK2yly2vtXuNWtU7BWWx3qua3b69GsbM+GEf08rey/6cbmE5cu611j17l/bsWOHu3TKZWYfER4jfK57k5YifO65RY0+LvxbUjvzx9Nj3ObSfMPPhc+L9CdFrsvwGL18XmWZP/zwo2EhcNXZtTNmJoa9qroerfPo1n05rj+F69RmdV8N22zWcwV39D1s/vzbWj6Xdt3pH2moP0nat+7JCuLde+99TjOb+iBfXOa8v1dVX+0cb/yEi7r+PTVPebt5P6iib/PnlLdOi/SFft9VPFrl6+b3Xp1DlffCKkwq3QfLxQ4Lm9UtZBeG9S6++GL35ptvNss8b968RiBOYb/nn3+++boVNtOsd+eff37j/TNmzEh87wsvvNBYmtaH3fQ4e/Zst379+sTPWMfL+5pm/NN5hcfT73o97z7S3lfp9cLOEEAAAQQQQAABBBBAAAEEEEAAAQQQQACBHAKE7Awka8CnbEhDu7cGh/Va0lZmsEcBDYVZkgZiw9cVbNCsS3+6/89u+/btScWo7PV4tjmVJQ64WctCWmE5q1DxYKQ181u8BJaWtVS5rC3eX2hX9XMdK9ysZb2qPqbfnxVMs9r+H664MjFg5/d1401zurY8cdGBYOuc2rme4/ZRJtgT1rn1vEifYV07SaE5HUv7Vh/g6+5rX/9GY4krqxyWXdxm/efifsvvvxOPaf2nVeYy9f3JJ580QmOhVbvnktVWut2Px3WWFvbx9Rw/KnD08CMLXByGbNcqqZ2Fx6/iWizSn1RxvLD83XhepC/JUx7NWhfPtqqQr8Jg1lbV9Rjbt9u+0j6f1vY0o+WZZ53d7D/T9pP3b2nXnYJdqkP1HXn2p9CdltHVTJEff/yxVSWpr1VVX6kHCf5oXX/Wd7jgIz152u37Qdzes+4daSh56zTv+9KOVeZvvf7eqzJXcS8sc+6d/8yQcwc+aCzbemDtJe7A6nEdXy62b82Frv/dW93gntecGxrs/Ck6VzioVbeQnQJk11xzTSOEphntVD4fKlNYTuE0hecUovOvW4/hecUz4sXvv+uuu5pL1Gq5WM2mF7+nit81i6tmrAsDdv75tddeO2yJ3TLH7Eoj4yAIIIAAAggggAACCCCAAAIIIIAAAggggEAgQMguwPBPqx5oKjrIXXawZ+/efU6zwVmzjSUNzipActHEi9277271p1/5ozWIGgfoVq9e7RT28eVUuRYtWpyrLPEsdfFMXhqkjpectAJm/mDx4KYvUyce48H8Xg82Wm1fg7tpM+nIRX9PCz552yoerfaUVp/WOZUJXfmyx+2jncFvv8/4sWifES//qpkPFQaJN2t52bFjxzeWnY7fq98tu7jN+s/F/VYnrhe/z7S2ZpW5aH1rxq6zzzmv2R/544aPCpX5WfrknXWN6LN52ko3+/G4ztLCPr6ew0e1J7W9tCCi7kdaItZbWTN6hq7+eVI7C49fxbVYpD+p4nhh+bvxvGhfkqdM1n0qqR+p4npUmWJ730468ZjU9hTM//nPj0vtF8LZ9eLlkpPKmue600yRkyZNTr3W4v3r2ps1a3ajH89Tr3pPVfWV93h63/RrZrSYxt/hiuyrE+/txf0gbu957h1J5563TvO+L+k4ZV+3+pO4LVf1e9J3xXbvhWXPvdOfG+rb7QY/fMn1rZ/q+taM73jA7sDqsa5v00w3+NFS5wb3d/r0mvsvGswKw2jWMq/anw+3dWO5WM0gd9VVV6WG7EaPHp0ZhAvP67LLLksNsN10003N4JsCfFqOuqhj1vutgN2ZZ57ZPK7CdlUsGdtsCDxBAAEEEEAAAQQQQAABBBBAAAEEEEAAAQS6JEDIzoCueqCp6CB3u4M9mp3uttvucEcffUzLwGXaIJUCIg89/IjTrESd2OKlYDXTimbg8ls8oPjDo45227a97/+c+rhnzx6nmU/C8wsHya2/33rr7Yn7jMsS7rfq55phL9y6OdhoLclmtf34nBWo+cVxv2zx1nu0pObOnTvD0+nI8yKhGBXAOqeioavwROL20c7gd7jf8HnRPkPLBIZLRieFVOP3qd7iWSXDclh24bUVvjfut+J2U9XvmjVr1apXwkO3PLfKXKS+FRxTCNgq7ymnnOqWLl2WuJSh+polS15oLIFqBc+KtJVu9ONxneUJ+4TYixc/37JUsTc7/FvfacyUqqWJrU1LlitYreMnhROT2lm4vyquxSL9SRXHC8vfjedF+5I8ZbLCuocf/m23cePGYR9v93r0O4ztfVvrxGN8X1YZNIOfFbzVdX7BmLHuzTffMpdqVch/165dTvs89hfHm/1K3utO+9qy5R03c+Z1Lf19loH6HbUDfT5rq6q+so4T/l33oPgcFN6tw9ar+0Hc3ovcO2K3vHWa933x/tv9vdffe1X+du+F7Rp05PND/W5wzyrXt/nGroTrGrPkrb3YDexc5Ib6PuzIKSXtNCvsFf89DKPVIWSXd7nYJUuWpAbh8i4X+/TTT7szzjijJex29dVXu3Xr1qXuP3ZM+137uu6661qOoSDhypUrm4FCP6Od3tfOsZPaBa8jgAACCCCAAAIIIIAAAggggAACCCCAAAKdEiBkZ8hWPdBUdJC7ysEeDQzr+FdeeXXmoKwGi7WEbJ6BWIMt9SWVIQydhAOGBw4ccJoFJxxktQJgSQdQebU8Zvj5cLYKLcF42De+2fx7VkinysHNpDInvW4NNqo83dqsth+6+jaigKQVOLh2xkwzaFBl+YuEYnRc65x0jZXdutE+ivYZVujFmlkqLnvSjHfexrJLao9V9lv++GUerTIXqe+XV6wYFhwrGkJWn7Rp0yanUF54/YT9XpFz61Q/3k6dKUCnYG14fno+6ZJLnZZWzLtpScvrrru+5f6g/SS1s3C/cXsu41ukP3nwwYdazrfM8cLyd+N50b4kb5msYJSOFW/tXo9+f1XUtd9XmccFCx5tqXu1UdW/zjnvdyb9I4aVK1c1ZnUMr5u8Ibu43LoGVQ+XTJ6SuVyz+rCkJX3D/VZVX+E+s55r1lXdi0IT9S1JId2s/VX5917dD6ps73nrVN7xTI1F7p1l3Xv9vVflbudeWPa8O/25oX2bXP9//R+n5Vs1w1zHf9ZMdP3bHnRDn73XtWVivWFa2Mv6W91CdlqqVTPVKXQWL/P60EMPNYNqem6dj3/tqaeecqNGjWq8/8477zTf+9prr7kJEyY03qPHOXPmNJaNPf30013W/v1xsh6tgN3ll1/uFCbUZ/Wo333ITo/tBO18O+ARAQQQQAABBBBAAAEEEEAAAQQQQAABBBDolgAhO0M674CU8VHzpaKD3J0c7NEgWtqMKhqItQbKzRMr8KJmpdPsdOEgqp9BS0uwffd7R7b8zZpJJu1wKnMY4tP+tF9t2ld43J/+7NjGzDJJ+ytaX0n7KfN61W2vaBms43s7H7DzgYK1a9c2Qgb+73rMO5BftFzh+4uEYvQ565zaGTiucvA7PK/weZk2GF8DWn5Zs4X5TUGtUaPObLkWFE719enfFz5adjp/a+uGi3Xc+DWrzHnr2worql3fe9+fUp3iMvjf43qsKpRVVT/ezr1Gy3mHfa6cFLxVOyu6WXWW1M7CfVfR5or0J3F96pz1Wp23TpXZ2q9VZ1bd5r0eQ1freN2yt/pOhfU1k2OZLW63ZUN24bHVjyusdu+997kjv39USz+vdqofzXa6YcPb4ceGPa+qvobtOOUFq99V3/L44wtTPtX5P1nlkmM37gdxG2nn3pG3Tov0hVXq5y1flceM99XOvTDeV89/Hxp0Q/17XP/7D7m+9Zd3PlynAN/aSa5vyzw3uG+Lc4MHuk6QFfqK/96LkN0DDzxght5UNoXbFHJT2CwOxy1btsydd955jb8pmKYlWOPz0e8Ktmk2Ou3jrLPOcosXLzbf55eJVRjvscceawTeLr300sbnqlg2Nitg58teZdCu6w2OAyKAAAIIIIAAAggggAACCCCAAAIIIIDAIS9AyM5oAlUP+BQdHO7GYI8GZF999dVhM6poAFFBnDJBCYOy+ZKWB9TsdH6wV4/Tr5nR+HscgiszmJgU4tN5xks/atYXDZ4mbfHMdyrrPffcm/T2Sl/fu3ef+93Z57Y46Xe93o3Navs6/zhgp7LIVoPNYZ3quWZC0WB/p7aiA8HWOZUJefjzqXLw2+8zfizaZ+jzCl7FM4uFS+7FM/LEIby4DPrdsrOCNHqvZkmK20KemZOs47bzmlXmvPVtLS2dNdtfWlnj2b7K9G1p+2+3H2/nXhMvAa4+QsG7MpvVfye1s3D/VVyLRfoTLYeqZVHDdp629HhY1l49L9OX5CmrtV+rztq5HsNy9PK+bP1DgHa+J6nNhG2oipBdaKUZ85597rlhIXgdc+rUaanff6qqr7A8eZ6//vobTvek0OWoH/3Yvffee3k+3pH39PJ+UEXf5lGK1Km+l4d1oH8co/65k1uvv/fq3Nq5F3bSpvi+h5wb3OcGdi12B96e7hpLuHZ4Fru+NRe5/s03usE9r7ihHgTsZOSDW3kfexGyO/fcc93zzz8/rKzLly9348aNa4Tc9J6lS5cOe48PximId8cdd7gNGzYMe49CfH4J2KSlX8NlYsP3PPvss41gngJ64et5Pf37VK4bb7yxGRjU/i677LLmDHb+ff5RQTv9Xe/Tj85Pn7fOz3/Geix+nfAJBBBAAAEEEEAAAQQQQAABBBBAAAEEEECgPQFCdoZfkQEp4+PDXrIGo/Va0tbNwZ4PPtjujjv+hJZBNYUIFCaoeosHDX972ii3e/fuxlJn4aBeuNRr3jJYIT4NJqsuTzzp1y3nlzVLnjWwai29mbdsRd8Xh1c0+8zmLVuK7qbU+622bwXs/M4VxrSWjb10ymWpA/n+82Uei4RitH/rnPKGrqzyxe246uCUjlm0z/DlVKguvJb8kntW2DTPdWbZWUEaHd8KomTNlOfLXeWjVea89W2dQ1YoN6nslnkn2oqOX7YfL3uvsfrbdsIYau/qZ8K2m9TOQu8qrsUi/Yl1bzjlP3/r9Hpdt7J9Sdb5xPaqO+t7TTvXY1gGy75b9+VVq14ZtoR02XCl1d6qDtl5NwUT9f0hvK4UglcgO2mrqr6S9p/0uv7hg743hGXV8/NHj6n8H32EZdBx9Y8C1F/HWy/vB/H11c69o0idxv/oRXXw9NPPxDSV/97L7706mbL3wsoh2t3hwD43+Mka17dxhlP4reNLxK4e5/o2XusGdj7r3FCf/vVNu2dQ6vNW8CrttV6E7BQi0wxzCpE9/vjj7oknnnC33XabO+ecc5ohMwXorHJrOdnx48c3g2hTp051WhpW57Fo0SI3ffr0ZrBNgb0VK1YM288bb7zhLr744sY+NDNeHOYLg3ztLBv74osvugsuuKBxnLSAnT/PMGinz+nz/m95H0s1Gj6EAAIIIIAAAggggAACCCCAAAIIIIAAAgi0IUDIzsArb7nCigAAIABJREFUMiBlfHzYS0UHucsM9rz77lb3l7/8tVSwKR7M06CaNVg+7MQKvvDGG2+6L//L15qDqArz/f3vy52Wbw0HVsPZt4ocIh4c1H51Hhqc9PvPM1CpwVaFg/xn9KgZVjTTSjubQgJ5ZniLZxzT8W+//Q5zEDhveTSQvHnzZqcZbtI2q+1fPu2K1GNby8YqMOOXA047Xpm/WSGFtMCYdU55Q1dW+eLrJU+bsvaT9lrRPsPvS2HMMFThZxdTu9OMbGGbXrDgUf+xxEfLTudvbQcOHHAKvYTHqGImop07dzaCktYxrdesMuet7/XrN7T0FzqXvJ+Ny6IZmHT+oUdWW+l2P17mXqPztK7BskGhpHBNUjsLnau4Fq1zSetP4jBIFX3dW2+tbtyrZFH1VrYvSSuHtXxqUttu53oMy9DL+7JlmKd9huX3z60Z29KuHZ237rEvvvSS30XuR302nsk3qZ78TquqL7+/Io+6fx1xxA9a+kz1n9fOmFnqu23WsfV9SLPx6nupgmTyCrde3g+q6Nv8uRSpUytYeNrpZ7iPP/7Y767wo/rYhU886bZv35742V5+71Whyt4LE0+oF38YGnBD+za7/ndv61LATsvEXuIGti90Q30f9eKMm8fMG8by7+t2yO7ss8928+fPd3r0s7bFj7NmzUpcClblVtDukksuSfy89qcgnpaX9ecZPt5yyy3Nz8ZL0up9CuaNGTOm8R49WkG9cH9pz5csWeKuueaaxBns4s8qaKf363Px3/L83mwIPEEAAQQQQAABBBBAAAEEEEAAAQQQQAABBLokQMjOgC4yIGV8fNhL1gCtXkva8g72aIBQg/NnnHFWYxYgDZ5qMLboVrR8Rffv32/NRHPeeee3zGCkwU6F8cps8YDoF/75i27cuAktA7aaPe/TTz/N3L014NfOjCoKT2ig+HOf/4KbNGmyU5gmabOW/VRwSrPSlN20bOcXv/TlxnKiS5cuSwzblWn7Gpi2lo3VYHknZuArGoopc05pzlUOficdp+w1qXammdfCYJdmdHzwwYdaXsu7BKpllxYuUXAvPHa7AQmFeXTdqe3Onn1DrrCdVea8QTlr2VItc62Z24psuiZuvGnOMAsr4NLLfjzvvSY+d6udffd7RzZmM4zfm/X7ypWrGvUbt5u0dub3WcW1WLQ/Wb169bBlLTUbrGYTLLOFs4Ee9o1vurvvvqetQEtchrJ9Sbyf8HcFqOOZB5OWT23negyPqee9ui/H/0BAbVVhy6KbgsgXXjRxWL9ghex0jb300tLmEuBll2Eveo1UWV9FffT+Bx54cFjbUlubOfM6J7+qNvnqH3T4dqx7TBy068X9wJ9f0Xrzn7Mei9SpXPSdIeyPZfSn+/88LIRoHct6bfHi5xszQWo/+u8V/XdL/A8+evm9V2Uuey+0zrdXrw199r4b2P5EI2DXt3pcF2axG+sGtj3gBvdtdm4o/R/wdNokTxArfE+3Q3bnn3++e/nllxtBueuvv95pWViF4rQ86oQJE9yCBQtyLZG6bt069+ijj7pJkyY1l4bVErH6/eGHH04M6YXLwWo2O81qF3r455rBTmVS2WbOnOl0PP+3Oj92un2xfwQQQAABBBBAAAEEEEAAAQQQQAABBBBAIBYgZBeLdGB5yaKD3HkHe5566umWgTANipUJgsWDeQqnaXm0qjdrVpVwIE/PtbRr2aX3FJ5TiC7eZ/i7ZnWJZyuxzjNpMLzMjCo6ngYo/WCuyqPnGjTu7++3Du8ef3xhy/v1mbJBDmvJODlbs+oVGYwNC+7DUKG1nl8wZmxj1qvwve0+LxqKKXtOSeWMrxcrOJX02byvF+0zwv0uWrS4pe0o2Pm//p//t+W6yLuMq2Wn80/aNFB+0q9+03KssgP0GuzX9Ra2KZ1L2vFVLqvMeYNyVh9SZjY+H2oNy67nVlvpZT8e32uKBOW0XGZ4fqrnorNXWsvc+n1m1bPqOr4Wy9y7ivYnapdVLWtp3Rt0/gpiVRUoaqcvsa5zhQzD2TJ9fSXNjGldj2p3ZbZe3ZetsFXR2b2S6lp+Vsju5pvntVxfel/R7x86ZjyTXdY1btVX3v6zTJ3Gn7H6fd/G9P12x44d8UcK//7hhx+5iyZePMxXQbvHHnu8ub9e3A/8weO+zbp3+PdmPVp1mnYNWrMtykb3taKb1cdrXwpXx1uvvveqHPG90Lom4/LW6veBT93ArsWu7+2ruxKuO7DmQte35WY3+MlqNzSwv+cUdQ6AUba3Ox7U63kDpAAIIIAAAggggAACCCCAAAIIIIAAAgggcMgJELIzqrzogJSxi5aXig5y5x3ssQItGoycdMml7pNPPmkpQ9Iv1gBY3lmukvaZ9rpCGH7A1HosMztMeLw4+BEfo0gIxBpoVJBkzpy5uQMQmq3joYcfGTZTU9Igoz8XLc2lQfy4/AoRWuE4/7n4UQG7/zjmp8P2o1m2NAAfb+20fSvMVzZgFZcr/L1oKKadcwqP659XOfjt9xk/Fu0zws9bM8KE7ajIbJGWXVb4yZrlSu1d10E8e01Y7vC5wjS6ztR+wrLnmR3RmjFToaA8syrqmoiXitbxp18zI9c1r89rNiSdb1hu/9wKSvSyH4+XPlU5k8JSYf3ouTWrmILAWiY3z6ZlCTU7l7eJH7PamY4RLxGufeQNkPoyFu1P9LkNG942g2ZF7r26FhS+VnA0PPcqlib356bHdvqScD8qrwKhX/nqYS3lVdkVrFU7tjarD0kL+Fj7CF/rxX1Z/VG8FLb6Js3gmqdPU3AsnDUtrG89twI91tKpRb9/WPfkpBkHvXE7/affR7uPSaF9Wan9qW/Yv794sEf1oPvT4d/6zrA2rH3HMwb34n7g7ar8nlH0GpTTrFmzhxnp/qX+xPru6MsdPupeEIfu5ayQso4Rb7363qty5P3vrrjM9fh90A3uXun635nrDqwe3/mQ3ZqLXP+mmW5w9wo31F9+GeEq7QiydT7IVmfjKtsS+0IAAQQQQAABBBBAAAEEEEAAAQQQQAABBPIIELIzlIoOSBm7aHmp6CB3kcEevwyTBq7Cn2N/cXxjpoikAWC9rpkkrABW0ZBCy8lm/KJghWZSCcvqn2sAWVbtbJqBT7MZ+X2Gj1kzuMTH1UBiPAOd31+Wr/alMJyWho2DQtpHUsgtLIM1QK7P5hlk1gC0Bmm7GYhI8ooHrsNzLPO8aCim6uu5ysHvpPMv2mfE+1Ggw7fV+DErZBHuy7LT+adtGjyPZ6DzZVBwdNOmTYmD9GpD+rsVMNV1pJlusjYdP14yV8c/7/ejh4WPFZ7RMtPhZi0Hqs9r5qO0WZTSrnd//lbITsfuVT9uhZ51vcog3Hy96Nrzm4Iwakv+3Pyj7imvvvpqYh2n9U1+H3rMamcqh7WMpwKO8lSZw02zkak9x1vR/sR/3lrWUuXW+actya3Pa7lwzQ4Wnq9/nufe4MuQ59HqS26Zf6t74YUXc/3I8oYbb3JHfv8os7xZ/bvVh7QTsku6z8ivk/fleIZQHU990nXXXe/27v3/r4uwTvx1Y/Vnvr71aIXs9FlrGXa9P6sfVR+oa1v9TXgcPc8K0bbbf4bn385z9S/jxk0YVn5/PlpaWbMBb9y40Qxs+WPLUX3zvffel9iGtU8FuON+T/voxf1Ax63ye0aZa3Dnzp3NpYq9uR7V5nV/t/pSb6776pNPPmW2v6ygfC++96rcRf67y59nLR6HBtzQ/q2u/907XN/aSZ0N2K25yPWtn+r6t8xxAzuedW5gn3PRfbZXJnUOgFG2zgcAe9XuOC4CCCCAAAIIIIAAAggggAACCCCAAAIIHLoChOyMui8zIGXspvmSNcidFiYrMtiTFmjRgJgGxmfMnNUYcNWguga+Lp92hTkLj96vmYWKzJTWPMmcT6xAgx/A++nPjnW7du3KuSf7bfq89uP3GT6ee+7vCy9dmuWrENvEiZPco48+1ggsKJCgGbh+ecKJZrhO5Zl86RSnAeQ8W9Kyk9qPZkDSzHZ33HlXMyyhUKDCREkzaSkA8vbbGxMP3W7bT5qBpswyxkmFtNpQWt22e05xOaoc/I737X8v2mf4z/lHBcesgIXaTVbIwu9Dj5ZdnvBTUjvw16OCOeqH1B+pX1IgRP3U0UcfY167GtifO3deapgiLLcViNGxdV3o+lBIQG1S128c+NE1b83iE15zus5U7rTrXec4f/5tLeeTFLLL6mc61Y+rr9fMpb5e/KO81YdNn36tm3LZVPf9H/zIDAKpnSb1NapLhbNkJKukvknH0ox6cTnytjMr6Kfz0PFVt/rRPeHww789LFCpNlO0P/HtTHWmNqnye7fwsWgb12er7Cd9Oa2+JCxnO89V91lLSFp9SHzN+bLmfcy6XjpxX1Y70fLnlpfvV/z3gLT+TLM9xiFkK2Qni6x+VKFCfd/w15iOr+8jVrhe5T77nPNyffdop//MW4d53pc0o2lcB/oupGW9df3IVj9qY+rDkizCfZxwwklO/wDE2npxP1A5qvyeUfYa1HdF6x/iyK7M9888/YXOvdvfe3VMtZewTSRdk1Yb6eVrQ4P73cCOp13/pusaATiF4Drzc7nr2zTbDWx7wA3uec25ocFenvawY2/ZsqXjS5ISlut8WK6MseqeDQEEEEAAAQQQQAABBBBAAAEEEEAAAQQQ6LYAITtDvOyAlLGrxkvWILdeS9qKDvZoIFIzeiQN9ocDR2nPFQrQTHCd3pKWdJ06dVruEE1SGTUgas1ipfPWcctsVfmqDNP+cEWhZc40C8uSJS/kGihOq1v9TQHKpIFk71JF20+aiUSz8uh82t2KhmKqOKewzFUOfof7DZ8X7TPCz+q52my8vKHaQNGloC27POEnlUFLVo8ZM65l4DqrjVp/V7+mmfl0befdFE5RoMTaX/yaFfjJCrfE+4h/92GCuB6TQna+zrrdj6fNlhWfkxU60OeTZvuMP5/0uwIxWrZc+w/fk7edKWCUNHtpuL8k+6L9SdgG1SbvvvueYUu+hsfN+1zXSt5l3sMyZD2P22De8mS9TzNSacbCrM3qQ6xrLms/8d97cV9WO1VILssm6e/6jqX7Y3wPsa4tf75V9aN57v/+mO32n34/VTyqj1E7Swp7JVnneV1BMQV8s5ae7cX9IG4jSf1XHuN2rkF9Z1QIMY9n2nsUdtR32TzfAfWebn7vlWHR/+7K496d9ww5Be3cwCduqH9PR390DDeo2ev6unNqBY6ybds2QnZv1zMEVyY4V+Qzqns2BBBAAAEEEEAAAQQQQAABBBBAAAEEEECg2wKE7AzxdgakjN01lkCNB5+qDNnpmFr+9eFHFpQOY2lGFA3+dmNLWtJVs79UsWk/sbdCGO0ECDXopzDH4d/6zrB9x8eyftcAo+onafnerPPeunWruYSmdaz4NYWULp1yWa4ARxVtX1ZW8OZrX/+Ge/31N7JONfPvRUMxVZxTWKgqB7/D/YbPrWBMWp8RftY/t2YjKroUtGWXN/ykciiEdP/9D5Tul3S9/e1vf881MO/P2z+mzcITXiNJgR+FW3TdFA0vh+GjuB6zghK96McVINHsmqGJ9TwpCFS2zAq4KKCmNtJOO9Pn02aU8+eSZF+0P/Htyz+qv1MISPdQf6wij3KYO++WRjDW77PKx7gNFimb9V4FSBVMSloiNS67VbdJ11z82azfe3Ff1uyPZ551duG6DmdLi+8hSdeWP38FCtVG1FasOsl6TeUtOkNxu/2nL3tVjzLQvUTLxGadb9bf1adr+W8t25x36/b9IG4jSf1XnvK3ew3qWtc1X7b9lf3vi25975XhyA3Z5WkBB/979uzZQ8juEA3Zqe7ZEEAAAQQQQAABBBBAAAEEEEAAAQQQQACBbgsQsjPE2x2QindpDXKnBWbaGezZsWNHIxiSdzBMyxA+suDRjg3wxxb6fefOncOWBvzu947MnGXN2pf1mmbe0P7CgdYqlqLVsTTYeMv8W3MP9CqQMHv2DY0QiVXWIq8pzPL880tyhzk0kHzGGWe5tWvX5g4pVdX2k2Z+Oe30M9zHH39c5LSHvbdoKKaqc/IFqXLw2+8zfizaZ8Sf1+8ffbS7ZQYaBU1fXrHCemvia5ZdkZCd37H6JS09qushvC6TnitIoQBW3iCPP078qONOmjQ5NSiXFvjRNbd06bIWx6QyW+GjuB7zBiW63Y8rwKJgbNrSillBIAVWZJ117/H90pYt7zSrq912pnp67rlFqSHoJPui/Umz0NETGepeqntqUhsJX5eTvIoEfaJD5vo1boNhGfI+/853j2jMjKnZpbJm/YoLZdVt2jUXfz7P792+L6uun3rq6Vx1rb5M4TB9xm/xPSTr2vKf0zWje3re4K/CTfrOoOujzNZu/1nmmFmfUfvTP6Q45ZRTczv4dq6ZBG++eZ7bvn171mHMv3fzfhC3kaT+yyxo9GJV16Da37hxEzL7eO+tvlDXSdj2o6Jl/irzTn/vVSHa+e+uzJPgDR0XUOB68+bNBO0OsaCd6lx1z4YAAggggAACCCCAAAIIIIAAAggggAACCHRb4KAI2XUbbSQcr6+vrzFz27xb5rtRo85sLLWl5ba0ZNiUy6a6hQufaMxswv+cLlebmj1p3br17o4773ITJ05q+spYv+t1/V3vq3pTnWlWGtWhBgZ/ecKJzeOrrjXjiIIVCrqxIVAngbBfOn/0mGa79f2Sgl4KyZYNhVjnqutFM+Lomgz7Qh3/oYcfyRX69PtQ+cLrXdeewoNlwkdWWePXQq+w7N6r6n5cAdgnn3yq5RxPPvlUN2fOXKeARZ77hfahEIxcwr5Jbg888GDpgEtsY/2uAI7q4vJpVzTudeqPVYYZM2e5t95aXWm7so6v19R21YYfffSxxr1WdaVy6EdtTvdkzaqqumWrVqDb92XV9fr1Gxp9S9if6ZpRuH7lylUd+Q6ge7vu8TqGjuXbl++PdP0pZF3F5vu+dvrPKsph7UPXkGZgVr8cfxeSifocXW8vvvSS27VrV67+yzpO/Jo36fb9IC5Hr35X+1u+fHnDNrwvqf2pHqq+L+k8Zc733l7V+Mg4rr57FFlmlPeO/OVl2/1HWyOjZVNKBBBAAAEEEEAAAQQQQAABBBBAAAEEEKijACG7OtYKZUIAAQQQQAABBBBAAAEEEEAAgUwBzZROeG7kh+fy1KHqmg0BBBBAAAEEEEAAAQQQQAABBBBAAAEEEOiVACG7XslzXAQQQAABBBBAAAEEEEAAAQQQaFuAoN3BH7IjYNf2ZcIOEEAAAQQQQAABBBBAAAEEEEAAAQQQQKBNAUJ2bQLycQQQQAABBBBAAAEEEEAAAQQQ6K2AlhHdvHkzs9q9fXAF7lSnLBHb22uLoyOAAAIIIIAAAggggAACCCCAAAIIIIDAPwQI2dESEEAAAQQQQAABBBBAAAEEEEBgxAsMDQ25PXv2uG3btrktW7YQuBuhgTvVnepQdak6ZUMAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQABrhSyaAAAgAElEQVQBBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrVAGRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBGopQMiultVCoRBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEEEAAAQQQQAABBOogQMiuDrXQozL09fU5/bAhgAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAgjYAoTsbJeD+tWdO3e6M8862/33//FP7p/+5+fdmDHj3IcffnRQn/NIOLlly/7WqBPVi/+54sqrRkLRKSMCCCCAAAIIIIAAAggggAACCCCAAAIIIIAAAggggAACCCCAAAIIIFCJwEcf7Xbz5t/utv7Xe5Xsj50gUIVAbUN2+/btc+ee+/tm2MiHjpIev/LVw9zJJ5/q/nT/n92HH35Yhc1Bu4/rb7hxmOvNN88bEeeruj3mJz9rKf+//tvhbv36Danltz6n/dSprRCyS63CEfvHzZs3u1NOOcUde+yxbu7cuSP2PMoUvL+/3w0NDZX5aEc+U7fydOQk2SkCCCBQUIBZjQuCZbz9UL7vZ9DwZwQQQAABBBBAAAEEEEAAAQQQQAABBBBAAAEEcgls377DTZg42f36P0e5vz63ONdnqnzTwwseaxxbx1/+8soqd82+RrjAQROyC8N3n/v8F5yCZHv37hvh1ZOv+EXCWUnhxYkTJzkFUOq+WWE5Qnbla81qD3k8yx/x0PvkoTjYPjAw4O666y533HHHuQsvvLDnYda6lefQuwo4YwQQqKPAZ5995q655ppGCFyP+p2tfYFD8b7fvhp7QAABBBBAAAEEEEAAAQQQQAABBBBAAAEEhgsMDg66l1escldcPcP99oxzGqGn35x6hjvvgvFu/u13ufc/2D78Q22+omOuXrPOXTl9prtp7vzce+tFWVW4Va+86k457ayGzZ/+/GDu8uqNN865pRkkO+vc0W7LO+8W+nx8fAXSFE5rd1POZ9qV1zTKdv1Nc93+/ftz73Ljps1O56KynD9G49TlVnQkZJeb/JB740EZsvOBu5N+9Rv3QQc61rq1kiIhO5Vds9Z5I/94511/rNtpmeUhZGeylH6RkF1putwfPBQH29WuJk+e3AhuKGj32muv5fbqxBvrVp5OnGPefWpmwY0bN7rbb7/dnXfeee74449v1JNmWjz11FPdpZde6p588km3a9euvLvkfQggMEIFdu7c6X73u981+gBd/++8884IPZN6FftQvO/XqwYoDQIIIIAAAggggAACCCCAAAIIIIAAAggcDAJaKtQHrRSYsn7+8/TfuSeeeqaSlbV27Njp7vzjPW7U785rHkshtDxbt8vqy6SJRq674eZmeSdf9odCE1GFITv5Fg3pxcfXPtoN2WliqLnzb2+ck+q/yMRaBw4ccNOvva7pQcjOtxQeqxQ4qEN2CpCdP3qM27t3b5VmtdtX0ZCdPKb94Qr3xS99ufFz401zCqV/ewlAyK5afUJ21XpaezsUB9sV5FJQSwGuadOmuU8//dSiqeS1hQsXNkNir7zyirnPbpbHLEANXpTB6tWr3ejRo5teCtYl/ajubrjhhp7PQtgLut27d/9/7L35s13Fee/9X7y/v1W5lVTlVuVWJbm5yfs6dhLHGRznJvF1bFO2wRgBEgghIUASQoDEKEYxmkFCGDOJeRTGGDMJIQkQYjBmtEFgCTGIwQZjgtdbn8X7bPfp02vttc/Z0jna/nTVrj2t1f30p7+r19bpr56uDYiwQb9m9/rdKPw+zme/6/2e86qrhvnH72WXXVZ9/etfry655JLKbWOHM8a76zrpcv8bTo+sRQJTQ+CKK66ojjzyyOr8888fuXsx/wajfytWrKi2bh37v4MxPB9zzDF135988smpgW+rEpCABCQgAQlIQAISkIAEJCABCUhgigmkmcwwbi1ZemK9Zeebb71VZ1tbddn3Kwx2fMfzxkcenVDEH330m2rjpkfr+smQR33po4vJbnfFWuogmfzmzl/Yi5mMdlueeKp0aPGz3GS35LgTBlrX3br11ergQ+f32ofdZE12D2/YVGfmO/DgudULL75UjLvpw3UPPdzL6kcsmuyaSPn5ZAjscSa7u+/+Ub3oj9kqHmTiuPfe+6qv/OfXxmVo+4P/9kfV7bffMRlG0/7cQU12075DLQFqsmuBM4GvNNlNANqAp+yuxfYBwxqZwzUZ9B9KTGIYaMgqiHFs8eLF1aZNm6r33ntvzP/swXDz+uuvV7fddls1a9as+tiZM2dWL7zwQv9GRuiIrgalEepy5644n3VGNaUHquEpxV/truvE+9/UjvOubp17N+YyTGaYsfqVu+++uz72pJNOqt59991+h+8R34+yye7pp5+uFixYUI/ZTTfdNGY8NNmNweEbCUhAAhKQgAQkIAEJSEACEpCABH5PCZCdLsxuV6+5viK7WV7Wb9jYM9oNmsEt6kq3BKU9stid992Le9uNdjHZ7a5YI+b0+a6776k5Ya6L7XRXrb58zPpfenz+OjfZUQ/bz3Ytad9jvCZjsnvv/fdrwyN1rb78ys79IF4MmEcuOqanG+rQZNd1JD1uEAJ7nMkOQ1lTIUMbmetiC9R4njNnboWZaFSLJrvPVs8/324CKZnz/u3fvzytsjRNxThqstv1s8LuWmzf9T2Zni1oMmgfF67x0047rWeYY1GXrHb9Chmtbr755job4f77719vMdvvnFH5XoNS80g6nzWzmU7fqOGpHY3ddZ14/5vacd7VrWuyq2pz4ahmstu5c2d1xhln1P/xIc9Wp8luV19d1i8BCUhAAhKQgAQkIAEJSEACEpDAdCdAZjhMc5ikME3tfOedYsgkjzjz7PPr42bNnlf97OcvF49r+xBD2LdnzKpOOe2s6vEtT9Zmvrff3lmbs2i/n8lud8aa94OtUU8+9cy6/zxjSquNZUcsqt566+388OL7MNmRjS62yWX7Wdj2K2nfZ889otp/1py6/cmY7B5Yt74io+BBcw6rMxb2iyG+Z+0z+r9w8bG9bYY12QUhn4dJYKRMdoB56qmnqz/9s78YY7T7/N//Q/XKK7/bhgVD1v/z/352zDGrVq2ujQcPrltXfX2vb1RkwGM71cce2zyO9yeffFJt3vx4tWzZCdXfff4LvXo4/lt7f7u6/vob6gxB405s+IBsQpzDudSBOZD2v/Slf6vOOuvsijSbeSmZxsJUmD/nJsNr1lzbizmO5bO2MpEYm+r78MMPqx/d8+PqwANnVX/+P/+yU3+jrlK/GcthmexKRjc+4yax5trrqv/48lfqsYHbZ/76c9Xy5acVxyfiTZ+jDjIu/uEf/XHd73/8p3+pLlm5qq6/1PbJpyxPqxjzmpsF/UYjaAXNEBd108all15W7dixY8w58aakgdBC/kxcTWUyY9lU56h9vrsW20eNW9f+aDJoJsUP4EsvvbQ22C1cuLAi6+sghTlm48aN1Te+8Y2K87kP/D4UDUrNo+x81sxmOn2jhqd2NHbXdeL9b2rHeVe3rslutE12bfrRZNdGx+8kIAEJSEACEpCABCQgAQlIQAIS+H0gsH3769WceUfWhq1+JrfIRDfoNqnBkexnrOGnZRCT3e6MNY2R12ylypaqGOvIKPfsc8/XRjdMapjVupQw2S07cXl17gUX1XXBnn71K2xLC3fav+LqNT1j4kRNdqlpEPNkF6NfxPjc8y/ULOj7ffc/WJsja8Ph4YsqxnMiJbRFPZseeWwiVXjOiBIYOZNdyYT1x//9T2pTXIxhyWR30smn1CaqMCqF0Sg3GD373HPFbWnj+HjGPMbWtm0ZgzDr3XTzLT2jWZybP2OauujiSyomliilfubnxfvJmOwmE2PEGs+w2LBhY/XZz/3dOJNfxMozY3DOOedVGLjyUur3rjbZYXT7whf+qTFmxgcDHqyayosvvlT973/7j8Y6qB+jZ8qB100mO25ssw6aPe74/Hxiu+KKq8bdhCZrshvGWDaxGvTzt956q/re975XPfVU8/7yGA6uvvrqavbs2b0tM/fbb786g8RLL73UeJ3GAva+++5bb//WFNtFF11UG5kOPfTQirbSki+2kyGMLb3mzp3bi+Wggw6q1qxZ0ynjJpnJiOuwww6rs4yx/efee+9dHX/88dWWLVsa+xIxMXZbt26ttyCDAeezjSjx3HjjjY0xpKYN+svi77XXXluR5Yw6Vq1aFU3Uz21M0rroC0zWrVtXG7m+9rWv1fVRL2OW86Tyxx9/vD6GdkuP0ni1xTMm8Kqqtm3bVm+vmvJBO03xxPlpv2gP1uiLTCWMEbHyzPtf/OIXcVrjM/VNRLdRIQa5vfbaq5o3b97ABruogz5ceeWVdeyMVakE2xNPPLHWT95nTHr0ue1aS+st6WEQjVMXcXM9cF0Ee7TFdUM/8uy26Jn4S3qKz+hnWqiH70Jv3J+Yi7ie+Zzr6ogjjqi1TZ8irmeffbZatmxZbV7kOPjwns+Ju63wDwr0n/ary/Wb1jnoHJLqOljkz03aoN38eqK/ixYtqg2cTf1N24R7v/km7V/6Op1/4RZ9T+dfru2SJtJ6QuPM8WQfeuSRR+qxhT3XV7414zDGifZ/+ctf1vNyGi/zEltI5nPIRDScnoP+ed9UBomlqY6JaCEdwzadpfcFXqcl1RN1lOaYtntOWle8hn9pbmeeS2PO5404n2d4P/jgg/X1wHXBdcU8han5nnvuqeNMj+d12s/8OuR9zEf5ebyPeTGdf+K3UK6n0vldPqONZ555ps6gms69bX3K6y2NT9d7AOObctiV8zJjxG83ro1dUdCH28VeUW+nCoe2+WlX8J/KOjXZTSV925aABCQgAQlIQAISkIAEJCABCUhgOhB4fceOavX3rqguWrm62vjIo60hhRGKLGzPv/DimGP5Wz3ZzchUt/SEUzqbrQYx2Q0r1jGBd3yz5robaoMbWehI2pRmlutqUguT3ZLjTqgeePChnmkO015b4W/BbEuLAQ1T3lNPP1PNnb+wfj9Rk11qGmQb3K7lgw8+rE5afkbd9mlnnF17aqJfw8xkxxrTzbfeXs07YlGdbQ9DH6/vuPOuMT6eprjx+tx73wMVmfbQJOzY4hdtPvLo5lavScqmjS9mQOotGQNzXePFwRxJ1kCOv/DisWv99INxxsB46hkrqpmzPzV00u9D5y+ovvf9qzpfU01M+Jw47rn3/mrh0cf1tn+GD5zuvOvuzmwZh3xsGC/G7eENm+o+YkqFZVPB78NYMCbfOeDg+hyeiY2xC7/WyJnsWOiYsf+B48xHqVmuZLLDqBVZ5FKjUnoeBru/+du/H1d3enz6GrMYGepKhUn9e5d/v5d9LD2v6fUZZ57VM0uVzGZN503UZDfZGNN+cwHecsutRcZNcR+3dNk4I0Sp37vaZNcUX/o5Y43Rjn7m5fXXd1Rf/dpenXWT1lsy2U2kvhUrzulph/gmY7Ib1ljmnAZ5TwwYxdgGM0xZ+aJ61IfRhkXn0mI0n2GSwMiE3vOSL9bm38f71IDBYn5a0sV2jDFLlixpjGXOnDkVC2tNhe84pqkvfH7uueeOu26iPvrIgnAwK9Uzc+bMeoE8zonn1KSAseDkk08eE0duJGhjktZ10kknVSeccMKYutK4MD785Cc/iTDq54mYDNriicq78GGhH0Ng6VpP+8WC8C233NLIGkMFRp2mMhndUidZ5zA1YLLDbFcqzz//fLV06dI6xjBqYQANQ1ic88Ybb1SHHHJIbSrKzUQcE2xnzZpVrVy5smceTceR17Rx0003Fa+1aAuNY4TLz03fo738OovzeebHEtdBek7+Or/WWLyfjMnuhhtuaJ1nyChIXKtXr27lw5xT0hb9wgSDaS/vS/qe65c5p6lMZA5JdZ22lb4m7rxwPbVdA5y/fPnyokElbbPLfJO3He/T+fe73/1ubYhL405fY5ZrMhqFxrkOvv/9748Zw9xcPYxxIv4nnniimjFjRuN4M4/DN+5dE9Fwek6byW7QWIJ/PE9GC+kYlnQWbaT3hfz3QKqnidxzog2euT5/9KMf9UyyqYZ4zTzHb5Nvfetb9dihnVLBiMb1mp+fvmcOzzOQpv1Mj43XTSY7GOT37TiHZ/TUNv+U+pB/xhzHvQ8Gad3pa+awpuuM+iZ7D6APtAeHXT0vR1uwY8z5Xdo0f+esurzn+hyWye6KKz41q/HMHwkee+yx6tRTT60WLFhQP3jNZ23/YYg/dNBndMR5bOPK71ru66XfBvSRbVA5juuu6ZiIrWSkS7/jfK49fjNSJ9fHOeecU/Fbpo07feK6Ofvss6ujjjqqPnfx4sX1f6Zgfmk7l+845pJLLqm3daVd6uC6bmoXDR9zzDH14+WXX67bPuWUU+p2+fdGlDiOOvttF0s9xBDxH3fccfX8X/oPaVF/PG/fvr3+zxL0mba69j3O91kCEpCABCQgAQlIQAISkIAEJCABCUxnAvz95oILV9ZGGMw1+RapqamoZDpq6lt6Xr9Mek115J/3izU/vt97PDEY4+jX8tNXVB999GmyhzDedd1uNTWjYdSLbXp5zjP8pTFtf31Hz1TH9rJk0Yusem0msLSO/DXGOvoz6Na/P/jhj2rTG+1jCKOk/WI8J1LCwElMN9x0a711Ma9LjxNPOb2V10s/+3k1f8Hi4rlRH3Xs3DnWZxBxD9tkh2mO9qJtnnOtf/zxx9XlV1xds02PS1/DHFPaRMsTTz1dzT708DFxpPXzGrPdjh1vNDbBdxyTnxfv+e6Ciz6dJ9pMdmS1PO74kxvroT62r+Y6GTmT3bZt26t//uKXxhiachNWyWSXGpvS12GyQ9Df/NY+Y+rlODLWLV68pH7E1qfp+V/6138vptNkW9qSqS89N3+Nkev22z9dyGbiXLny0grj3fzDjxgX15e//J/1d3x/7bXXjzFNlAxWfJaXycaY1vfkk09Vf/G//mpcnHkf0/clk+J0NdkRN9nofv7y2L3eWVjGLJj2a5DXuckOd+yioxaPqw8tHTr3sGrpsuOLRlDYs6AbZdOmTbU+2O42z9JH5sejjz6mpx+y8KVlWGOZ1tn1NT9A6AcLROmiLQu6mADywqJUZFrDrHDbbbdVLDaxaE0GkjAwcP6dd96Zn14vJsZiLYtsTSUMGLnZguNTgwB10RbGEoxPL7zwQnX//feP6Q+LhqVtOdF+GGwwemH0ePXVVys+37Bhwxhj0mWXXdYzXkTMsGNxNBa/MTKRQQcW1EN9kXUGZrBLS2pS+PrXv17Xw/EstmIgwpyVljYmaV1dmLRlYotFburJjRVd4+E4+LD4GXwYy3vvvbfmg2bI8hd8mgxyab+CEfXABqMgY87YRxtNYz1Z3dIfNEE7JeMMfU1NIvQnrhM4kmUMXUXh+Msvv7w27OWGR46JseZcHtHn5557rl605/swdraZ/jBeHHzwwXUdHM95XCNwJVMli9bRBrrD0JEX5lz0z3H0H96cSx3UddZZZ/X4cz2l/Yy60nEs8YvjUu3RHvMJpid0iFkhvaaIJa7f4ANLjJYpnyaDTHr9w4bMkVy3xBrXb2TCatJVWsdE5hD6nc5nxN1USvMNmiSGfBwwDoRRLOpLxyCupbb5Js7Ln9N4GaPQFeODPrk2GY/QFeaNkq7oa2iKeKgHzphKyfQYmaxSxhMdJ/pANrS4Jun3ddddV48z8zXzUsSMrkr3rpRfm4a7mOwmG8tktZCOIddcU0nNZ/m9IOUR49h2H26752zevLlnsAs90R6/QfiNEWMTmipdJ+kcz/hyf+E+Q5xcHxdccEFvnjrzzDPH/IZP+5/OQXmf0+PQdBjs0AzzIO2g1/T3Q9v8nNZXes01HNuT03fma2KKaz6d55rm3mHcA7IrwcAAACAASURBVFImxLEr52XmD3jGWPNM35hf8jmtxKzfZ7vCZMe9g3sTZqv8gXGOPnHN5gUDIXNJfk68x/T105/+ND9taCY7THpcs9Fe+twWN9rnN0F6fPqac9FMabz47Oabb+4ZCtPzeM25fJ+fG+Y5fkvBmntFnItpMEocx3dtJjvMh2Gui3riGSZk9C4VxpHrO8x1cU48Exf/FiqNd6k+P5OABCQgAQlIQAISkIAEJCABCUhAAtORAL6QOYd9uq0sWdXyv3Wwrk5mM8wxGHleeWVrp27sCpNdv1g7BZYctPnxLb2sc/c/sK73TWrG6peNjpNyMxrnwGvGzNnVT555tldv/iIMcWwXSyxpuxMx2TF2557/6Xa1C446tnr3vffyJovvySQ4/8hPzWtXr7m+p4G8X8WT+3yYmuxgQna18757cfXwxk3V5i1PVNfdcHM165BPs8CR3Q2zX6lgyortj6OOnz77XJ0FDnZLlp7YM3Y1mfW68u2ayW7fGbNq8xyZ9GiTrJF3rL1rTPi33La2Z7A76phl1UPrN1QY0V5+ZWt14SWX9rLxYejERDho4ZzIokcc11x7Q/XaL7bVXOCDeROusI8MhXkbGEFTsyCZC+nHU0//pOK6OOW0s3pxUk+Tye6dd96tFh97fN0WbZIZkbFhLiCW0848pxfLEQuPHi2THRff1desGWdA+o8vf2XMH6D7mewwy7G152f++nNVmOzuvfe+cVnnMDW9//77vbFsyjB2xx1re8fwAgPN/gfMHBMnhjIMVeFO5Zizzz53XJsHHjir+tWvfjWmPmLMjVu5OSs9oYvJbpgxssBBNr08xn333a/62c9+Vk92/E98Mt3lRsW99vpmjwl9YLHu3/79y2Pqyk2UaV/jdek86uHztJRYEvdRi4+uM2+gMbI83bH2znGxchzZCdOCISw3F+ZjzZhjmGRr15xRPo6l+siSl2YFQR/zDjt8XF3nnnd+Glr9ujQ2bTxLxxPzRMZyXDAtH8TWYfniNYYUjFFNC0wYE1j03GeffWpDRd4EhgUW02NhNM+yEYu1TcaXqC8MGMTHInlaUoMAJhiMbfmPPBbo0sVpDFB5Wb9+fc/k8dBDD+Vf18aQyAiHOQPjTVpYUIcDfW0yKGFGoq8cwyJ/unCYmxTICoUemkobk7QumNDfnAljzmIwsfDAyJIfQ9sxRhzTZjJoi4d6nn766Z5xAj5hmkn7l5pNMIPt2LEj/boe+1SjF1544bjtzWCKqYh4MTSUTGuT1S3syKrD4j8LrHnB2AV3zB0PPPBAjysaYfxLfcNYQn3ElpdgS59KmRQZNwyGbSYwYsZMQh0cx/H5eOfXCVmK8mMYkzDqnXfeeWM0TNwcf/vtt/d0VbrWUn22GZRS7WEwyK992gvW9ItHSVvERF1h1uB1XjBWcT7HlK7/tF9N4z7ZOYSY0vmMcW8qGNja5pt0LLkO8u2+0zGg3/3mm6Y40njRNhki88K1nhqQfvzjH+eHjDGScs/AcFIqwxgn5lX0RL+Zy5l38gKfOIbsemSbTEvKr03D/Ux2w4hlslpIx7B0bUS/mf9hxiO/F6Q8JnPPSXlQTykbaaonYildJxhv+K7pt0l6n+AY5uZSSeegvM9xPHMDcyXtMTdwDp+lhd9Chx9+eH0MJrH8t1B6bNNr7jUxh/F7hj6khTb5TwVc78RC9rO0DOsekDLZ1fMy8cOKNsnkSr/igbmPz0u/JdJ+t73eFSY7DFYYttauXVv/e5RxwuzF/ZfvyEyH4TMtaRxkZEOPZIfjXH7DhPmObHhsp52WYWWyIzaMm2QShmkeN30qmfwwDUaf77vvvvo3GVrktwIm6fiu9B91MKBhpONx7bXX9v4DDO3zPr7jd31aUvMc9WMQpG1+RzGfRUmPazPZUQe/G/ldT79p/4c//GHPeEc/uH7ywpwAlzx+/o2P2Y/Pm7jldfleAhKQgAQkIAEJSEACEpCABCQgAQlMRwL8reSSVZfVppgm4wxxk41r5zvv9DK9denLsE12XWPtEhvH8DeudKvW7dtf752KsfDkU8+sufTLRsdJuRmNusIQVjIuck6pja4msF6g2Qv+7lXKzJcdNuZtypUMYxjAouT9is8HeU5NdpjBtjzx1LjTyZyH/jBwpRkF48DU6Mm2o+seenjc3+jRKCY36uCRmgWjnq58u5rsaAdTY9NafzoemADfSzxRERN9wWRJXU1aiWNLz5de9v363P1nzal+8sz4/8QNl8hUyTFkS8zLffc/2DO/lQyKXCvEGVu/luYKjmFbafqBwe7Gm28dt+sLx7D1bJj+RiKTHZ3igmdLzJJR6bTTzxiz2NNkssOYlE5C6SBdddXV40xLP7pn/EIshrrcKEX7aXnk0UcrsoWlx5GdjIssLUwMeRa0z372b8ctuJaMYbk5K623i8lumDFu3vz4uP5iDMOUmJc8NgxpGByjlMxybaawtvO6muxmH3LoOGMj9ZJVkPjScWSrYiadKKtWrR7zPceWxrq+eFdfNu7YfBzJLpi2x2vayEuJOfpmoSwtTJy5AbKNZ6neiY5lGkfTa1iSGSqMX7FIHBlSuEbaSph/Sua3OC8MTbSRLn7xfSzWlr6L83luayc1CKxYsWLMXJTWEVty0seSKaJLLGGioY50wR19kYmMz9sW7NPjMG6kJtTUpNBlEb6NSVoXC7pN211hnpw/f34dd1ObwSXvc8q23xihI0yF1NFvrDE4hZEgNwmk/WqKl1hYlA6jwQ9+8IM81FY9xcFtusV0e+CBBxbNciyukr2EPuRmotBq6XphMXi//far2LozX8yNsYYdxulSgXGYJkumqtQEynFN1zZzQmS0K5mLog+MJdooldSIR+x5ScexdC3G8an2Hn300fh4zDPaRuPEU+p3HNwvJsYUQw+L9Ok9Js7nOe07Jp68RLxtGm+aQ6KutI0SO47rej2lcx4GAuafKOkYtF1LcXzTcxovRr20jfSc9DgMqk0abxtD6hvGOGE4jPkhn2PSmNPjcv2l/No03M9kl7YxkViGoYV0bJquabhwz+M645He//gu5TGZe046d3NPbdIT8yDXGbGUrhOMk1zPGHtyrcUYp/3BvFkqcU2X+hzHp9dZmxbCJMe9gXlmkEIfuG6IozQvR13pcfk4DOsekDLJr4uIY1jzctTHM1qgD3AgwyEseGDGRAPbtm1LD+/0OjW3pRnQmk4OQ1lpa9bYdhVTVX59UB+aPProo2vTWf49mReXLFlSZ7kt/ccA+s25mLZys9qwTHZNcfM7MTLc8dshvZ4YZ8z2mNT4zZRfr9xL2UKW7/P/yIHxlOuF70qGfuric75nzNP/dJea59oM4ulxbSa7Uh20z3iHUQ4zc1r4rXf66afX8V1zzTXjflMxN0eGP+6/Kbe0Hl9LQAISkIAEJCABCUhAAhKQgAQkIIHpTGD9ho0940zJlDSZ2Idtsht2rPlWrfmaWmSjazImpWxyMxp1kUEMw9Hc+Qsr2soLZifq5hi2p6V0NYHldcX7iTDf8sSTtQYwPmG2Skver/S7rq9Tk11TVkC26cVcBwsy6mHoTEvK6sKLm9c/MbFFRrsS9658u5rsMCXmsaZxdxkP/sYaxsjjTzq1+uCDD9Mq+r7GoLj+4Y3Vo5sfH+eTipPT/pA9MS2p2bNte2T+nhpZEksmu/R6ausHpr8V51xQj/UeZ7LLDUb93v/N3/599cILL6a8q5LJ7j+/+vVxWYnGnNTxTRfDGxnF8rhLhj2aLJmqaCMtXdpMj8+NbMTCZ2kZZowlo1neXrRNmtbP//0/jOGTZmCbCpNdbnSLWMlAR6a9dCyJPVLNsmCxYOFRY77HlJePX9Q36DjGeaXnksYx0+Vu5EFNdsMcy1Lc6Wdsu8bi5GQWKiNbDIaFhx8e7wxP2yu9jsXaNlMK57GASpwlc1JqECgttke7TPCR4QyDVJqdkGMiQxLtYDzk+K6FxT8W4ji3bZGd+ljomzNnTr2YmmbDS00K/eqgnjYmg9QVY/itb32rmI0wxoi+5QvDKZ+2eFKDE5nY8h+jaT1krcH0Q3tkv0qNq137lWqC+PMSfZ6objEWEF/JEEfmNr4jw08+H7A4jsEiNz8QX/St9F2w7XedpAaVPCNemAabxjllFH0g1nxBPwyG9JFYmwxpaX356+grdbRpfRjai7bTNnNdxTH9nlNdleaaycwh0Xa/NjiO+zRGmyYNRl1cZ1xvHIeBI83Sm/JoG4Ooq+m5S7ycy/2a64VYSpkcu2q8KY70834xxfXf73qC0dKlS+v5OjfMduXXz2Q32ViGoYWUV2m+DLapKS2/F3TlQV3R59JcxO8SNMLcXDIbRSxpzKVrMY5re07709TvLnNQ3A+Iu8msRxzpfTCfn9vi5Lt03s0Ns/m5GIP4jcH8jBEoyrDuAV2Y0GZc06XfbRFTqptB5mWuK7KbHXbYYbVeYM/9CjNYft+NtkrPu8Jkh+ms9B8b+J2IWQzTGGOUFjLEsfUp8zSGu7wwf5INGHNmbiYclsmOLVPT31tpDGRIJG40lWb1TPt0111jtzmI87lWiRuTWvrbb9OmTcU64zyew3yI8R/DXJTUPJfPRXEMz+lxbSa7/Luog+uH7IH0nbkpLfw24nc/v/Vee+219Kve6zgm59Y7wBcSkIAEJCABCUhAAhKQgAQkIAEJSGAaE3j+hRd720yWsldNNvQuBqOubeyKWB9Yt77OqIW5jNd5YTvP2IaTbGFtpWRGY5vMyFCWbkUb9UQGstTY1NUEFnXkz4Oezzahy05cXhueSluJlvqVt9nvfWqyw+zVVNrauuqa6+oY+22/S91hjmRcMZ6lpSuf1JSWx5zqus1MRrts18u2vWEe/MUE/iN5Gv9EX6f9YTzSkmZdLGURTI+NMSqZ7NA4/eRR0ntaT1wbI22y+5P/8ae1SS3tOK+7GpDy87q872eUKhmv2jKHcTyLlOmDz9LSr830WF73M9kNM8ZSXX/6Z39RPfXU03lY9Xv6mW8Hi1Et+lz6vo1fNFI6r2smuyaTHYsxxxy7dIyJjgyFZHujYMb5xjf3HvP9P3/xSxV7rpfKoONYqiM+66rxQUx2wx7LiLXpORZAWZzkdWrAaDon/5wFMLbbow4eLHiyEIV5LDSVn5O+j8XafmaHiLW0WDvIYnu0V1rcR8Nh7qIvbE22Zs2aOvtI08Jj9CVdACfWiZR0sbmL6aWNySB1pQaB0mJlMINJ6fvoa1s8LK7CnDryhco4P55TY1A+3l37lWqC+PMyWd2GWSE3SqATxo5+ltoNU0dpfMOomfeZ2INtv+sEDYf5KtVhypTvOa6tpOOV94O6yM5CH3lg1GVxnr6xIN3FnNp1HIehvehn1zaZtzAMY/ggs2D0M39O+UYbk5lDoo5Uu6U2OC4dn37XU2gnH/euPCKupucu8ca5xArHko4jztJ3cX76PNFx4rww+5WutbSNttdd+aVzQn7dDyOWYWghHcP8ek8ZxPzFGOb3gq48qK/tnhM6yPWaxsHrNOam64Tj+A3Gto8YYdi+O7+O431Tv7vMQXE/QLtNmUaJJWXUlvUx7yvvUwN1U6yl8+KzYd4DujCh3RjLtussZZJfHxF72zNbqmIA++Y3v1mPbVtbpXq4Prl/YaIaVia7JrNa2lZuskuzumHS433XsjtMdmF2wwiYbhmLrsg4CT+uMYyAjEmXcvXVV9fncS3kmebjfOrndwUPXkdpM8/FMTy3Hdf2XdTB7xlMwfQvz0Z3/fXX1583mSrT9hcvXty4JXW05bMEJCABCUhAAhKQgAQkIAEJSEACEphOBHbseKM6YuHRtSFm9qGHVz/7+fj/GDrZeFMzEuaciZZdEWuaOa2U8YxY02P6ZSwL89HBh86vtm59te4qBja2msV0xNaz6d/IyH5GnXxHxrv429hPnnm2wkjG57kZqgu/riayqOuW29bWRkNMU2REy0v0a97hiyrGcyJlsiY72Jx59vk1E8Yq3c62FE8bw658UlPaZEx2xBeMGdNvz5hVnbT89Dpj4JtvvtX5b62lfuafsVZy+9of1JqbMfOQmhdt5o9cVykTzIxtJfRQMtmFEfLAgw+tMMW2lTD2jazJ7iv/+bXqiSefLDLoakAqnvz/Z3u47HuXV9/+9n7VZ/76c2NMVGlWs3idmrRKpqY241VTDOnng5qz+pnshhljqa7g0vU5zcCGSSA34U2VyY4xYCvgvB+MB6UUa8nYF2M56DiyqHPjTTdXBx44q/q7z39hXBx5XCnHaLM0Pk08S8fmbfR7X4ohYsmfMTykmexYIGbRi62hBinbt2/vbS8ZC9Y8s50XWYC2bNnSaLyJxdp+xoq2xdqui+30qW1xn+9Z8GVrKzKipH3hPQa8devWFc2DaQwTWQCPtlkgpt0ui81tTAZZuE6NE2xlmZcYI+LKjRXpsW3x9GsjrYfXUVeecbBrv7qMx2R0G/HlW9GG2bJk4qRfwZLz8xLb65VMAtFev+sk5ZNmDEyNPnlGszwO3qf8WGDOCz9a165dWzStYLplHiGWppLG2ab14DUZ7UUMXdrEIEMGqPTab3pdGkPaop2JzCERZ8q+qY30emqKL/88104XHhFT23OXeOP8GM/S9dFV49Q1mXFKr4U27UXMTc9d+bW11/ZdU7v558PQQjqGjFFTSdvidVq68uCctJ70njOI6TCNuXSdYI4hexa6z6+F0vumfodmOSfvc/Q/tFuqt+mzQbWXMmuKI+IpPadam+w9oAsTYggupXtaxDiIbuIcnsmgShz8Z4hgPF0y2U3EZEefGFe2bMXQRYY0jN5sl8p8F39ESxnE691hstu5c2f9u5TY8qxv6XayfH/sscdWq1evrh577LHGrIJc65jWOL6LuTH6Gs9dDHIc23Zc23fRDs9k6CPOdFwZD/rI510fObe0DV9LQAISkIAEJCABCUhAAhKQgAQkIIHpRCA1rZFFrZ8hZqKxD8Nkt6tiTbPUXXDhysY1brbWxKREVrSNjzzaiKLJfMQ2sJyfbzmbZtFL603NXbkZqrHx5IvUMNXvfHYVxGBJfKsvv7LIIPo1lSY7tk8lYxxxsq1qv923UgZ5BsL0uzY+6ThM1mTHWsa6hx6uZh1yWN0H+hEPzHDo79XXfpGM4mAvqR8NYXyLetue836nfc2/yyMJPZRMdvHdnHlHVpjo2krMDSNlsvvz//mX1RFHLKi342z7g/9ETXZAW7Lk2IotP/uZidLv+5ns2oxXbYMY3w1qzpqIyW6iMZayuaVsurxOjVkl41qTKSz48Fw6r9SnYbBsM9kdPHtOhfu7VLq2jdmFLXT/8I/+eCAdphyj/ZJxronnsMcyYmh7Jj4WKmfMmDFmoZKtmVjwa7vO03qZpF966aV60emggw7q1RWLn5jtSpk5YrE2N4CkdfO6bbG232J7WhcL+hFT00I1fcGARRa7uXPnjjPcka0vz1aTxkCfJlIGXWxuYzJIXXAIJqWt7mKMOKaJWb8xStvA6NivRN/IJMZCaJSu/eo6HhPRLWYFFr9LPCLbUGk7TPoQLFetWhVd6j1H30qGhODR7zqJOogt3co2NViwbVlpK7teIJnJrhRrHMuPVbIIsaieGnZpn6xRZOuBcV7SONvMJsGrxDqtM/iU2MVx/dpku7eZM2fW48p8SL/ILpiWVFe02VQmModEXV3aSK8n2HR55NrpxyPi6ffcJd6oI8aztBVojGEeZ5wbz5Mdp/RaaNNetNf03JVfW3tt3zW1m38+DC2kY8gYNZW0LV6npSsPzknrSe85wzTZkVEr5iTu2dx34J2WNI6mfodm2+ag0G6X6zCOGVR7aaw5+7RPTa9TrU32HtCFCXEEl8nMy2l/+D361FNP1Vuu8p84giXjvHLlyjHbmKbntb2Gy3TIZBcxYtS/+OKLq4ULF44xb2GMZBt3rpG87A6THf8+Oemkk+qYSmYxflPccsst9Xa3qemMfpD5ln8jpmVQ7um5vO5qkGs7ru27tD1+x+QmuzT+tL9tr0vc0nZ8LQEJSEACEpCABCQgAQlIQAISkIAEpgMB1tfZGhYTzncOOLhav2HjLgsrjDS0hQFn0LIrY8VM1GZEKn2XZpzL+xIGo9x8lJr5MNxR+DtoZGbLM+QNYnjKY+B9VxPZxx9/XK0454KaweELjq7eeKO880b0a7qY7JaecErjf/wNHimDCy8eu1abftdmKEvHYbImu4iLv7E+tH5DndUwzzRHhrvLr7xmTLbDOK/f85YnnqyvZTQ7f8Hi6uENmyqMiWlJ+5P3my11MZFyfv5dWgevQw+5ztPvumQbjLlhjzPZ3X33j+o/hvMH8fRR+sN+Di/eT8RkhwFn7332bTQ1kUnsf//bfxQzivUz2ZnJ7g8auWLCS81hJbNckyksxptnxu9L//rvY9oZhsmOsc2Ngm0mu//zf75a7dxZzqDUxWSH6ezIBYvGtRkxkFkRHf7DP35xnBk05RhsBjHZlY6Ndrs+l2KIWNqeub7J0sZiaCxc8ozhYSLZ7aiPxVDMelFfaVE5Fmv7GSvaFmtTgwDHtZVor5RJqek8ftC8+OKL1VlnndUz3M2fP39Mxr/IYEZf+8XQ1M4gJgXqaGMySF39svsFM/rWtrjfFk+6pSH1tRV4k4WN9vLF+a79SjXRr700li66Tc0KOY8wcc6bN6/ezjqtm9fBqBRT9K10ncR5/a4T5u9+28XmTPMYeT/IeMX5GMu4D9x44429DHeYqUqmyugrY1zqb9Q5DO1FXf3aJGMf8cAYw3CppLpiTLqWLnNI1NWljTBzEi8GAPrW74FJgjii9OMRx/V77hJv1DGM7WInO05c46O0XewwtJCOYWluivFrM3oNoqe2e07MdZPZLjYdY+biksGfPqX9aep3lzkoNEnm1RdeeKHvtQgrDLwlA3Kwzp/TcW6KNT8nfd92X02Pi9dt94AuTKgnxrLtntNFN2RK43coczNzXjzIYkcs/HaeaEnNUl0yqoXhCsMZc2paOD83Y6Xfp21RT1tBw4wBxrVly5b1DHdsrZr3d3eY7N54440Kcyb9azOLsVXstm3bqgceeKA688wz64x8nMNWsswzUejfnpLJjvtWPq5s3cFY8HkX3US/fZaABCQgAQlIQAISkIAEJCABCUhAAtOZAMaqi1au7hns7rn3/oH+hjlo38JIg3lnUJPdrow13ca1ZKZr+qwtQ1eT+Yi/22LOo84w1JWMd8G2zQwVx7Q9dzWRPfX0T3rGrKb+Nn0+qOEuNTTmhrW0L8Ewrx+GYUrMv0vPj9fTbbvYiCt/ZsvgtT/44ZgMd/1Mbnkd6ZbG849cXL2+Y0d+SP2+TVepZq6/8Zbi+fFhjFHJZPe77WLn1mbPOKf0vMduFxsGplKnun42EZPd9y7//jhj07777le9+OJLY/Yc7meU4g/3CxYeNaauLiaxtr71azM/t18mu2HGWDJm/emf/UVFDA8+uK7T44knnugtvpeyqVHfU089nXdzzPvSmE/WZMfEeMyxS8eM5R//9z+pNm/+NIMKWZRm7H/gmO8x+jUtqHYZx3vvvW+ceQ5T3aOPPtZjRMdL/S0Z3Erj06TH0rGTGcsxA9TxDYu+zzzzTG2OS7dM5TU6SQs6ZoGUB4uHpcIYspDGomjJ2BaLtSye5tnh0vraFmtTg0Cb8YW+sShGLPk2pMSJ9ulLvoAZcXD+7bff3lvgTbe5Y8Gc7b2ou800RF3BbbKmlzYmXRauo19hEGgagxgj+pabyqIOntvi2bFjR0V2N+pItzFNz4/XcGFr3hLLrv1KNUH8aQn+E9Vtm8kuWJU0kOov32aW+NA/Y4BGOTYtwZbv04Xq9Bhep0YMFobTct1119VMS9dhehyvyZgDf657tlyMQlxoHXZsp53HGcdhUiPWpvHuOo7Bk3omqr2Iqa3NdEzbsjylusrnmsnOIRFnWxtxTGrqZVwnUtp4DFJfl3ipj+suzG0lA1UXjQ9jnIglnfParif0jc5hld/juvJLYy7NC5ONZRhaSMcwnzdSLaSmtPx67Moj55/f98OI2W+eSmPOr8U0ltJ8Gn1K+5PfJ+KYLnMQ2fiYo/rFHHVO5DkdZ35TNc291I3mYJDP0cO4B1B/FyYcF9f0ZEx2mNHS36JwXrx4cX0/YM6dbEnNUmz/2a/O2Dp0V5vs0n5hXOM/wSxatKj+nfnII4+kX9emN8xepZjiwDYDYNt3cf7LL79cZ6kjhp/+9Kfxcd/nV199tZcB7/LLLx/DF+MkcXONMg6DlK5Z6NqOa/suYuE6Y44mTq477mNRIv7zzjuvb3bgOMdnCUhAAhKQgAQkIAEJSEACEpCABCQwXQlgWrtk1WV1xiqyVt186+2tf4McRj8marLb1bGmJqxzz7+oWv/wxtYH5qHI9IUpqlTazEds5cn5PNgmNraQZateDHdpaTNDpcc1ve7KPG2nyUzX9HkXo1sa32RNdtQVBq4ZM2dXjF9bYYyIHd7pVryc09VQlvLhdVpSxmxjm2eNS4/95a9+VXE8hjp0XSoY4zDIEXOX7XDTOtJY0HLTukLan9zI9+Zbb1Vkn6N9zIxtf0Nv0/n9D6yr66AeXreVzY9vqfbd/6Bqj8tkNxUmu5JZ6m/+9u+rn7/88jjGXYxSbPWZZ/760T0/HlcXH2DiO+PMs8Y8+CwtXdpMj+9nsuPYYcZ42ulnjOvvXXeVJ/I0ztJrFhBykyIsb7nl1tLhvc/4Pmde2rp1EJZkpNtrr2+Oqffzf/8PFfuAU7iQSya8Rxq2o+zX9iD17QqTHX0a5lj2BmcCL5hot27dOmZbrnxRPUxBLHq2GT3astZE5i/qKGW8InQ0edppp9WL2KXF2nSxfcWKFY0TfGr0ys0OaQawNhNY2ud0UR5eLCDSj35GqJtuuqk+Ljf6pcaAPL7SELYtYHetKzW0YRLMt8ek3WEsqKcGzfv2BwAAIABJREFUm/33379i4bWpPPTQQ71FdVilpWu/Uk2k40Rd6RhOVLfBPt3qkLrDbFFimbLOryXODWNbXiffRXtt2ko1WNqOMzXgodWmH1PcjyMDJWYoMthE4ZwwqjZticuxpDXGrMb1UNJy13EchvYi9rY2UyNUm8kOcwFGGvrFmKRlsnNI1JVqN28jjknjxZCKtpoKY1b6cd7Go6mu0udd4uU8rnmufdilWxlHnV00nvZ7ouNEe2RZ5Rohlnx+iHh4JivZPvvsUx+XX5dd+aUxl66FycaS1j9RLaT3xjZTWsxRcMvnsK480nmwNE92nafSeTy/TtJY2vrz4IMP1mPbpoMuc1B6DbTNrWgKwxSPQUv6OyjPpJvWxe/YCy64oO5Xzrcr27Z7AG11YcJxcU2XfrdFzOlYla6PaIvtYc8+++wKs2HTvSvqHPT5+uuvr01Up556am1MbDqfMaBPGK7YYpZrLy39zGocH1vTppns0APbk19zzTW1ma7Uv1/96lcVv29pm3jTEpns2La96bdVW2xt30U7xEfbzLvpbwKyPBM3GffQTalEJjh+x6e/MTdt2lSsM62D7cFPP/30+sHrKF0Mchzbdlzbd9EORlV0Qd9zAzLzB58fffTRjdlvox6fJSABCUhAAhKQgAQkIAEJSEACEpDAdCbA36Mw1YXRC7NdaU1h2H1IDUCYc7qUXR0r9a9afXltBtp/1pzq2eee7xvWW2+9Xc07YlF9zsmnnln8D6Vt5iMMVmSxw3x00vLTq0VHH1e/Xn76iopMZGlpM0OlxzW95m94GLVoq1R/nEe7jE+/x1nnnF/Xdej8BdXPfv5yffw777w70N/Ah2Gy2/LEU7Upi34xfqW/sdK3995/v1qy9MQ6Zoxj218fm9ktMqhRT5spLYx6HDcZkx2Z4aijzRxIX4iF4wY1MKbXWFt/yFpJ/Txyk12aDa9k/AzNpHGWMtlt3fpqdfCh8+s2mq4T6mLuia2KNdn9359uVVrK8hXgS1uUlrKgcfyD69aNMV1h7Eq3i+UYTFZkPEtNX4uOWjxuYmPAL1m5asxxf/lXn6mefe65CK1+7mfOGnNwVdVZ5NK2eY3xLi3DjJH4/uC//dGYfnz1a3tVr2eTQ9r+E08+WT322O8yFKXflUyCbMPK4lap0A7t5X1etWr1uMNLLGcfcmjFAlJeMEbm/SJzXbqQU4r1uKXLxhmtGOvVqy8bF2OqnVImuaasc2gEraR9Lml8kDrp/7DHMmc6kfds1fW9732vNiak56fZ29iS7fXXX0+/rl+z4BuZ7EoGoXRLMrJBcHxaGDcWWSOTSWmxNl3g5jiO57y0sDi6atWq3oI6ZoG0pCYw4nz++fE/nKgzMtnlGb6oKzVknHzyycWMeGT4CqNJ3t9+i81pvLxuW8BO6/rGN75Rbdy4cRwTWF966aU9JrmhLdoj6xomBB5NRsh+8fD9008/XREL9cAnvY6jLeYYtMQxJRNX2q/SgnzUk2oCPaRlGLqNjEC5SS9MDBhz0EMUtHPDDTf0OOaGHRZyFy5cWG/1mi5gx/kx1nBBx+g1L2S3Cb5szZZnZOQctm+jjjZNoIO43og5v5bCSEg9LKzn3xNXmsmulHUJo02Mc5tZKgwWtJWbetL+B5/S/BDHtWknvf5hk2cKog5MxxEz8dBmWtI6JjqHUB8L//vtt189Tm0GoQ0bNvTG6cILLxxn+KAuxuaHP/xhrSuuv3Ss2nik/eIc9JkbSuKY9Fpjbkt1H8egRa55uKEtYs9LjGHpPhHHpownOk7URTxcI8RDzKXtgdOYS3NRVw2nJrjSnDWMWCarBX5/LVmypOZR6ivM0ntX6XpM9dQ2v/S756S8msaYe0foqXQtpnN8aXzRNObGuBdTR36fCM11uf+lxjZixnyTXmtRF3FjFCN2/t2TF/qeZ59Lj0nHGY757yWOTe8D+fw9rHvA7pqX6c8999xTrVmzpvh7IWUzmdeYp4866qjaMMV8WRo76uceFMelJrlou59ZjfEtmew4P4xop5xySjEbd2r2ytuOLHOYKkv3Ln7DL1++vO5fmzmQvpXus+n5eTY65nsyC5LhrvT7EJb8TsKMlrdN1nHmRL7jt3XOnfeMB9/nBsguBjm4th2Xfse9lrk4LbQPa7iWjHRp/KXzqYsxv/baa+tsg3n/0rZ8LQEJSEACEpCABCQgAQlIQAISkIAEppLA+g0be1uDsl3sRAx2nINZLDeFtfUrNQB1NdkNI9a2mFLD27HLTqrYOrZf4e8+/Yx5bSY76o/sdWF0iqx2eduTNdkRaxi2Fhx1bPXue+/lTQz0Pvo1qPkrbWQYJjt2yjjtjLNrA9d3Dji4WvfQw+P+3ohG4QxbOF+95vpxx/A3/DAhzjnsyGrbtu1pqPXr5194scJsFmM1GZNdag48/8JLxvmYaDDNZNcvM14eLOPLOBMrMRN7WtDD5i1PjOlPbrLjeDIsBrcTTzl93HVBPTCHPW2VTHYcs/ryK+vvqevGm28dZ8bkGAx/UY8muw4mOzKWYeJKDUuY5O688wc9gQN2y5YtFVt3psfxOjVKMdgsRux/wMwxx2HWOvvsc3tZCsi0c/U1a6o/+R9/Oua4b3xz73FZYdieNDftYQLEaEUGAibZNDNFyfiVm+yGGWOpLrh89nN/V2FUi4UDYty2bVu1YsU51R/+0R9XZAuMrVfTi4oMgl/4wj+N4RL1rbn2utq8xwIh5ro77lhb/fMXvzTu2CZzWslkR91HLT66l6GChUPipg6+Sx9sK5wWYqUf6TH5WMNn5cpL6z6nx/E61Q6LIfMOO3xMXRyDOS9dzHz55VcqtjLO6yqZ7FjULGUGJB4WtqmXdqMMeyyj3l31nC7ozpgxo14o3L59e71VGYvYLOyFYQeDDzzSQt9ZZGORm+M4HkMYZiUyZ5BRK87nmJKJJjV5pPWQJY8tbqmHRUC+43HCCSf0rok0ltREsPfee9dbRJEVBPMAC4mYQMimQh0YohirtDBHsfgc8R522GH1YjsLcTC58cYbK+rlfBb3WRhNS2pSKJkx0mN5HaaUEpO0Ltojbo6nH3zH2KQmhcMPP7y4sEs7YRyjHjjClTEi+1Fa2uLhOLR+2WWX9caBuDFsBR8WmTHY0E6TuSLtVxujVBMl88RkdRsZGPOMXGmWJnTGuKMTjGtkzsLAQv9SDTI/s0DL56WFZtgFW47hwTiQBYZ5GI2ynRnM+K6JHfWguTCW9NME+oh7RzrOfBbaiWsWPTE29JdxZC6IWDB35SU3S7EIz5hQTzpH7E4zBwaByG7GdYqJBZ0z1mS3jGs/xoAxyctk5xDqSw1CXA933nlnzYZtvNPC9ZQalrieMKQwBugCfcS8xzjl2upyLaXXLLGQtSgv6bUGm3TujDiYL4Nbk65C420mO9oexjhRTz5WaJBriZgxMzF/EzPsGIO8dNVweo9rmrMmG8tktUDf0msNLWEuYe7numRsYn6JcczNOKmeOKbf/NJ2z0kN2VEPcdAmxt5Zs2b19ERbpWsx7Q/zEUYt6uD3ANtqxn06+lO6T8Cl6/2P+xh9or6YF4kXPeXzInNwbkZN52b6w5jmJR9nfh9FG2gXA3bMU2Q1pO28pO0E26bfBU3Xaso210HaXlzTpd8ocVyqm6brI47dVc9wJRsbZi4MVStXrqznAq5xvuO3DobFMNg1GaomY7LjPxgsW7asjoHfypi6+Tcbvytpn5iIr2T24p58zjnn1N/DEM0SN58zPhj3OJdHbnSDacTN99wzMLbxxyTqYM4nnmg71y2MIjb0yNwZ93Dap67gVrrGuGfBnHvErbfe2jNT0j7v+ZzvMa6mJTXIkcmvqbQdl35H/zDA8hn95nfb2rVre7Hz25XP80JcxBdsI9MiY8cYUiffkcUPrVskIAEJSEACEpCABCQgAQlIQAISkMB0I/DIo5trQwzGmKOPPb7a+uprfbOXYY5LzXSpwWn2oYf3dqPr19dBTXbDiLVfTKmZqGQ2ajo/treEI0auvIQZrWQ+4li2hU2NW2S2w/CXl8ma7KjvrrvvqY1Os2bPq7PP5W0M8j76NdUmO2J+6Wc/7zH89oxZ1Xnfvbj66bPP1XpmfE44+bS634xRySgW/U5Nf/TrjrV3VU88+VS9ZTD9DQMY9fCYjMkO4x/G1qjrqGOWVQ+t31CxReuOHW/UY0UMfI8x7Qc/HJtAKGJue077M+uQw6orrlpT9+Xue+6tmYR5LmIo6Z4tb09afkYvzuBCpscH162vTjntrArmUUeTzulXZG2kXepkbJgLGKuzz7uwZ+Y7YuHRbhcbRqSSASkGnT9cH3/8ieNMS5z7d5//Qm2s+8xff674PceccOLJPTNe1EnGu9xAF7E0PWPOuv32sVmPqI/tSdmmtOm8POteF5Md9Q4zRrLSDdpf+oNBLc/cx6IOZro8i1xT//PPOY/zqScvTSa7vI7S+y/+y7+Oy6aHdkpbrJbOL32WmuyIFRNf6Tj0h8ETPZa+57PS9rjUWdoaOK0jN2AOcyxz/sN+zxiTFS5fgI+F63heunRpccGXeFKDQRyfPrPIFlmHSou1qcmDjHuRkSetI16zCJ6bw1ImGHnD6BXn5M+YL1iIKxX0yGJ+LHTn5/J+zpw59Zal+fmDLja3LWCndcEsFv9L8cycObOCYVPBJIL5MT83X1xviyfq7sIHk866deuK80far7YF+VQTpYXdyeqWhVS2+8UsgbkhLRhycgMH7DBEoRt4855sZWghjJdN2cioO9iyVSnXUql+6kR3tF+aeyNGYggDUT6m8R5zRduCMOaNtuuMeugXC+hNsWzevHncvJGP6e40c6DNNItfsIhn2GJmnD17dj1+MEoN0sF3snMI9ZQ0hAbyQvvMeU16IHbiZk6if2npci2lBjHqKl1L6bXGPIOmg1n+zFyOGalUQuP9THbDGidiwIQdhtA8Vt5zX2vLbNVFwynDXN8ph8nGMhktEEdqni2x4HqObUj5Pp//Uz1N9p7DnIF5pel3BXrH2BNmu6Zrgzm11Bc+oz9XX311736PQa1U4Nrl/se5mOnC2NrULnpjrPMCzzin9DsnjmecMEq1XfPMzU3XGfVM9h6wO+fl6Peufmacr7zyyp5hCmNU6YHBDjN9qYRZrWRk43ja4DvqzbPR8T0mc4xqpXb5DLMaJtHSPRVNhZktP586w4RXii3i5hi2Zs3P5z1zd9P9fOfOnb2tbEvn8hkmNbSbF+bzm2++uZE77ZJNMr9/oeFgNVmTHdfL6tWr6z6W4ocJ2fxKBTMdY0mcpXP5jCx8/Ac3iwQkIAEJSEACEpCABCQgAQlIQAISmI4EwiQV5piuz6mxKDXLcX76XVuf0/OIo18ZRqxtbfA3KEw+9KHJJNR0fpoxrJQhLmJvqjfdkpP2r7rmumJTwzDZvfDiSz1j5f0PrCu20/XD6Nd0MNkRM0a7+QsW98xeJT1jsCP5V1MhsRbHlM7lsxkzD+nphPe53lNdd8k8R3ux7W5TmxjYMMdNJMskScfOveDT7WZL9dOfy6+4ujrw4EPrPl94cXmtBINcZPkr1TP/yMXVUUuW9r1+qOe4409u5EvdGPHYXtZMdh0y2SFkjF55RrLUiNT2umTgYzK86KKLBzKKnXHmWeP+kE9suLDZbrYphoma7IYZI4sud931w4GNdmRuK23VOpHY4IPBjkx5nF8qEzXZYSDElFgqTdvVNo1X+nlusptMXbkOItZ+prncZDfssYw4duUzC1AsWGNAicVfFrHZCpLF4yY9REyYdljkjm0SMYZgBGIxl4W5MGCUFp9TkwdZp8iiwWIgmVwiloMOOqg2mpQW+SKGeCaDBu3SPnGw8M1iP9thsfDPQmlbYfzIYMFiZtofFuEwJDadn5oU2swY0XYbk7wusnLAhBiiTxjEGDOO7Vc4hv6E6eGAAw6os6Wk57XFkx5X4sM4zZ07t7r++utb48n71cQy1UTJGBTxTFS36DkMJ/k2u/Tv4Ycf7pmxuCYY97gGyCSEUY5xoN/otLSdb8TIc7ANA9Kzzz5bZ0bhGgt9klUPwyrt9ytwI6ZUD9RFthVMYl3qoD9c21zjEQf9ob/oqmlROmKjDfodpjW0lRsAdreZg5hgS0ah0Dp9Iy6MlXDDXAfzpm016d9k5xDYYrSLrIPEcNVVVwW6Mc/EnM83xMc1yla9TYv7Xa4l6iYOtIpOMRHlJb3W0ClzLFk7uZ5j/mWMYy7Pz4/3ucbj89LzsMaJuhmrPF7uF5gXS1s3p/EQRz8Noxnmc8ak37w+mViIa6JaiD5x78Qwko5dqqPUCMbrtOR6muw9h7q55pjXYn7hmTmKaxRWYfRFO6US45POc1xTjC2/OdItf6mr9FuYervc/6J9rl0y5h177LG9OYTrJ/09E8emz5jiIk5MR8TeVPiOzJawCDbMV7RJ23GvaTqfzydzD9jd83JbP4b5HVyZz9AH9+gwTcEVjWGCw1TVVMKslt/H4niY8x31lkx2HIcm+U1BttvIkEb7GABL82/UzTO/Lag/zHZxHvMY7dFuKbaIm2f+4EK2SO7rHI8mMd89//zzrZpk7iCLHYa0aJ9nssD24xbcuV9hUqVdnnnPf2IoXQvDNNlh1oMdfSTeiJ//3AMLmPQrjA1jBPPgRgZBsjUz7hYJSEACEpCABCQgAQlIQAISkIAEJDBdCYRJqmSaafssNRbx90i2gcQItPSEU+qsVF36m5qRiKNfGUasbW2k2eROPvXM4tadbedjjIPZvvsfVGfnSo+N2JtMdhwbWfT2nzWnIkNYqQzDZIfnhf4R65lnn9/p78mlWPgs+jVdTHbExN/z1v7gh9XCxcf2sqthJKPPZENs+xtv9BNGd9x5VzXviEW9zGoHz5lfXXDhyurV135RG+vi+kivBc5Pdd3FZMc5xPTMT5+rTj1jRTVz9tyeAS3afGVr+e+kEW+/Z+pft37DGCZkTly5+vLqzTffqrMmYpKjTxjpWH8plZwL2ehgdPOtt9drg6GHNp1TL2bB9Q9vrI5ZemIvMyAZAnl//4MP9a49TXYdTXZAZXG/tE1pmKIwWrHN5n98+StjDG+8Ly3oI5qbbr6l+vP/+Zdjjo/64pmtUy+6uLzXcYiIhZfSVrXUkZurumayo+5hxkh9Tzz5ZPWV//xaa3+JmT6TYa1t8YDYfvzje+ttZ4NV2/Nf/tVnaqMf5zWVksnu0EPnFbdpjbYY91tuubW40BLtkG1wr72+2djv0M6X/vXfxxyTm+yor19dGAnPPGtFddDBh4ypq2mLXH5gXLJyVaPhMzfZRZ+GOZZRp8+/HwRyw4OLfMMf99jSkMx0r7322vAbSGocxICUnOZLCexyArnJbpc3aAPTkoD3nGk5LAYlAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEhhDIAx9GK0wF1okMFkC/Gfpc8//NGPe3PkL6y1vJ1unJrsBTHbAJi0iW41iFMMIhtGKrTqXLz+tTg2IYemYY5eOMTdherr33vsax4qMGtdff0P1rb2/3cv0Rt20cemll7VuH5lWSuaLCy+8uPrHf/qXXvvEtmzZWFfnICa7qH9YMVIfjDCzwSnd3hSjGQzg27ZlZsQUz2l9//CPXxxjFqP+I45YUD3wwIOthr2oq2Syw+iG+/Xuu39UffNb+xTHPc5ve6aOW2+9rbEOtMWWrmHe47lksqONiCfVDGbNhYsW11lUmCxWrVo9pi7qY7vZUsF4uHHjptqYxzhwbGjwoYfWl06pP0vZD2MsGxvyi5EioOFh1w8n1yZbwJKhiuxmTc7+YUSiyW4YFK1jVxDQZLcrqO55dXrP2fPGzIglIAEJSEACEpCABCQgAQlIQAISkIAEJCABCUjg94/Ae++/Xy1ZemKduYwshKXdJH7/qNjjNgLsYoV3pqnsfOedeptXsuF1zeDXVFd8Pm1NdhGgzxLYnQSaTHa7MwbbksCoE9DwsHtGOLb4w2jH9mZsb7griia7XUHVOodBQJPdMCju+XV4z9nzx/D3rQfnnXdevbUn23v6kMHu0gBbIVgkIAEJSEACEpCABCQgAQlIQAISkIAEJDDVBDY+8mi9VSfZ7F762c+nOhzbn8YESGJ14imnV2euOK96//3xW8mSaOq6G27ubXN70y23DaU3muyGgtFKRoWAJrtRGUn7MZ0JaHjYfaNDhtMlS5bUGe2+9rWvVRjitm7dWmcUTaPgf4JgyrvtttuqK68c7H+GaLJLSfp6OhHQZDedRmPqYvGeM3XsbXliBDTZaazbXca6tB1NdhO7Xj1LAhKQgAQkIAEJSEACEpCABCQgAQlIYLgE+DvVRStX18YoDFQYqSwSKBF49LHHa0MmWepmHXJYbahjm+E333qr2vTIY9VJy8+o9tlvZq2lhYuPrd55591SNQN/psluYGSeMMoENNmN8ujat+lCQMPD7h2J3/zmN9XatWurfffdtzbbkdmOxwEHHFDNmTOnmjVrVvXVr3619x0Lru+//37nIDXZdUblgbuZgCa73Qx8mjbnPWeaDoxhSUACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQKBCJDGeYpDHf+B9ECJD+qCTy6+fHaYIdWmh5Ljjuhen3HjqER02Q3NJRWNAoENNmNwijah+lOQMPD1IzQr3/962rTpk3VueeeO8ZYh8EOox2f8z3HDVI02Q1Cy2N3JwFNdruT9vRty3vO9B0bI5OABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJlAjs2PFGRfYxMpH9+L4HSof4mQRqAh9++GF1z733VwuPPq6X2e47BxxcHbP0xOr+Bx+qPvroo6GS0mQ3VJxWtqcT0GS3p4+g8UtAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQksCcT2LnznerCSy6tXnll657cDWMfMQKa7EZsQO3O5AhospscP8+WgAQkIAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpDAqBHQZDdqI2p/JkVAk92k8HmyBCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQALDIqDJblgkrUcCEpCABCQgAQlIQAISkIAEJCABCUhAAhKQgAQkIAEJSEACEpCABCQgAQlIQAISkIAERo6AJruRG1I7JAEJSEACEpCABCQgAQlIQ
-
-
'Unbelievably Exciting' Results in Rare Type of Breast Cancer
Metaplastic breast cancer (MpBC) is a rare form of triple-negative breast cancer (TNBC), accounting for fewer than 1% of all breast cancers, but it is very aggressive and responds poorly to chemotherapy. So new results with a combination of immunotherapies that resulted in significant tumor shrinkage and survival topping 2 years have led to some excitement, even though the results were seen in only 3 of 17 women who were treated...
There was one complete response and two partial responses with "very little tumor burden left. That gives us the hope that maybe there is a chance for cure in these three patients..."
-
It looks like Chasing Cancer with WaPo is an ongoing series? I missed the one June 17, best friend's 60th, but see the one on June 24 is a different topic. So I'm wondering, was the previous one postponed, didn't happen or I just missed it?
Joyner, thanks for that OBR share. Interesting research for another potential benefit of my dr. putting me on a statin.
-
Cancer drug: New treatment halts tumour growth [not bc-specific]
More than half of the 40 patients given berzosertib [an ATR kinase inhibitor aka VX-970, M6620] had the growth of their tumours halted [in a phase 1 trial].
Berzosertib was even more effective when given alongside chemotherapy, the trial run by the Institute of Cancer Research (ICR) and the Royal Marsden NHS Trust suggested.
...One of the study's authors, Prof Chris Lord, a professor of cancer genomics at the ICR, said these early signs were "very promising", adding that it was unusual in phase one trials to see a clinical response.
https://www.bbc.com/news/health-53137328
Looks like there's at least one clinical trial testing this drug with bc: https://clinicaltrials.gov/ct2/show/NCT04052555
-
debbew, I read about the trial and if I read correctly an exclusion is MBC. ??
-
I don't see where it says that breast cancer is excluded. Here's the only reference I see to BC:
I hope that my cutting and pasting works!
Whereas the traditional approach to cancer treatment has been to categorise it by tumour site - breast cancer, lung cancer and so on - the precision-medicine approach targets the genetic abnormality in the tumour, regardless of where it is.
-
LoMa, maybe you saw that information on a different site rather than on this one? Perhaps you saw something more in-depth? I hope not!
-
joynerL
“the precision-medicine approach targets the genetic abnormality in the tumour, regardless of where it is.“
I wish more doctors would sign into this philosophy but they still go by standard of care in my experience even at MDACC.
I know we can ask for expanded access or compassionate right to try which I may have to do with my Neuroendocrine features. Right now so many centers will not include me in Neuroendocrine drug trials or even Neuroendocrine standard of care because it is breast cancer. Sarah Cannon cancer institute in Nashville said I don’t qualify for their breast trials because of the Neuroendocrine! Arggggggg
i asked about the MATCH trial and my MO said that is in their phase 1 department. I met with a phase 1 doc along time ago and they have not sent me a single trial to even look at.
I talked to the RACHEL trial coordinator ( Bintrafusp Alfa + radiation NCT03524170)BTW- She said early results are not good but a new one should follow this one that looks more promising. I ran a bunch of trials by her that listed MDACC as a trial site. She told me they were all in the phase 1 department not breast! 🙄🤪
So I continue to check here and compile my Trial list. thankfully my current line is working but it's only a matter of time as we all know.
Sorry for the rant.
Dee
-
Dee, wow....you're way down the road past me in terms of knowledge of trials and how they work! Thanks for the explanation, though we all wish it were more encouraging!
Here's the latest post from PracticeUpdate. I thought that there would be more excitement about progress in immunotherapies than seems apparent to me:
https://www.practiceupdate.com/C/102335/56?elsca1=emc_enews_topic-alert
-
Sorry for my delay in answering. Under NCT04052555 in the Exclution section the 5th dot says metastatic disease. So maybe it’s just for BC and not MBC
-
AlabamaDee - disappointing to read that MDACC (The University of Texas MD Anderson Cancer Center ?) doesn't practice what they seem to preach. After reading Lorenzo Cohen and Alison Jeffires "Anti Cancer Living" , I had more hope for integrated and new approaches. I think they are or were based out of MDACC. Not medical DRs but part of an integrative approach used at MDACC focusing on lifestyle. I looked into trials a year o so ago, I wish I had known more at the time . When I called once place after my MO sent records, they said they had nothing for me, and probably wouldn't prescribe anything different than my MO had. It seems like my MO mad the comment that my history with cancer is unusual/rare, that the cancer itself is not - that it is one of the most common kinds of BC
-
Here are two new articles on MBC from Practice Update:
-
-
Joyner
I’m so excited you posted that article about ablative radiation. I am sending it to both my MOs. Neither thought my SBRT to the single lung lesion would have much effect on OSR since there was no study. Now there is!!!
My RO was quick to say SBRT was feasible.She is fantastic and warned me that while she saw real benefit, there wasn’t a lot of long term data. I bet she already has a copy of this article to show to the MO community.
Thanks for posting.
Dee
-
-
Joyner, very interesting article on SABR. Thanks for posting!
-
-
Quoted by Dee above: "the precision-medicine approach targets the genetic abnormality in the tumour, regardless of where it is."
It is starting to happen. I am in a Phase 2 basket trial that is testing neratinib for tumors with ERBB2 mutations. The trial has arms for various types of cancer (including cervical, salivary gland, lung, bladder, breast), the common requirement being that they have an ERBB2 mutation or related EGFR exon 18 mutation.
P.S. It's working!
-
ShetlandPony that is amazing!
-
So happy to hear Shetland Pony!
-
ShetlandPony: Yeah! That is great news. I knew you were in a clinical trial but couldn't recall which one.
For others interested in this topic, I am also in a clinical trial. It is the Aviator trial. Long story short, it seeks to harness the immune system to attach cancer. Won't get my first set of scans for a month or so. You can read more about the trial here:
-
Thanks Lumpie! That's interesting and hopefully successful. Would be great if we could figure out away to use the bodies natural defense system to kill cancer.
-
-
yay Shetland Pony- great news
Lumpie- hoping for good results!
I’ve been contacted to submit to a Neuroendocrine trial at UCSF -Keytruda with taxol or keytruda with Camptosar. I’m excited to be considered, but it would be too far from home for the number/ frequency of Infusions required. Still looking for something to put in my pocket should my current line fail.
Dee
-
Great news, Shetland! Keep us posted!!
-
Functional Status May Predict Outcomes in Hospitalized Patients With Advanced Cancer
A new study is suggesting many hospitalized adults with advanced cancer have problems with functional impairment and this is affecting their outcomes. The study findings, which were published in JNCCN — Journal of the National Comprehensive Cancer Network, revealed that 40.2% of hospitalized patients with advanced, incurable cancer were functionally impaired at the time of hospital admission. The study also showed that functional impairment was associated with higher rates of pain, depression, anxiety, longer hospital stays, and worse survival.
Lage DE, El-Jawahri A, Fuh CX, et al. Functional impairment, symptom burden, and clinical outcomes among hospitalized patients with advanced cancer. J Natl Compr Canc Netw 2020;18(6):747–754.
-
High Prevalence of Urinary Incontinence With Breast Cancer Suggests Potential Overlap of Risk Factors
Urinary incontinence was highly prevalent at diagnosis in women with early-stage breast cancer, a prospective, observational study has found. These findings were reported in the Journal of the National Comprehensive Cancer Network.
...approximately 80% of patients had prevalent urinary incontinence at baseline.
"The incidence [of urinary incontinence] we observed seems higher than one would expect of women in this age group without breast cancer," noted the study authors. "This frequency raises the question of whether risk factors for developing breast cancer overlap with those for developing [urinary incontinence], an extremely common problem in breast cancer survivors."
They ... identified a need for management approaches for patients with cancer experiencing urinary incontinence, given that survivorship guidelines from the National Comprehensive Cancer Network (NCCN) do not currently address this issue.
1. Chung CP, Behrendt C, Wong L, Flores S, Mortimer JE. Serial assessment of urinary incontinence in breast cancer survivors undergoing (neo)adjuvant therapy. J Natl Compr Canc Netw. 2020;18(6):712-716.
2. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Survivorship V1.2020 — March 17, 2020. Accessed June 26, 2020. https://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf
-
A quick peek at "risk factors for incontinence" finds: BMI, smoking, and diabetes are among risk factors for incontinence-- these are also cancer higher-risk groups...
-
Lumpie, fingers crossed for great progress on your trial!
-
Lumpie - thanks for posting the incontinence associations with BC. It is so interesting the various associations with cancer with other medical problems. Does one suggest the other? Years ago, ong beore any BC, I complained about more frequent/urgent peeing issues. Assumptions were, well I'm getting older, perimenopausal etc, maybe the fibroids. Just wish there were better very early detection tests, long before any lump shows up
-
post treatment incontinence issues may be due to neuropathy. Early on I mistakenly assumed only feet and hands were affected but urethra and eye neuropathy are also possible.
Also any hormone blockers can exacerbate it as drop in estrogen is a factor in incontinence.
-
Moth, yes, the article implies that there may be a connection to estrogen (which is not surprising).
BlueGrilRedState: Yes, I am so hopeful that better detection and very early treatment methods will evolve. I think that if we can really make progress on the CTC and cfDNA testing, maybe we will be able to detect cancer super early and rev up the immune system with immunotherapies to knock out a whole lot of cancer before it ever becomes clinically detectable.

-
Phesgo Approval Allows for Faster Administration of Pertuzumab and Trastuzumab
The Food and Drug Administration (FDA) has approved Phesgo™ (pertuzumab, trastuzumab, hyaluronidase-zzxf; Genentech), in combination with chemotherapy, for the treatment of early and metastatic HER2-positive breast cancer.
Phesgo is a fixed-dose combination of pertuzumab (Perjeta®) and trastuzumab (Herceptin®), HER2/neu receptor antagonists, and hyaluronidase, an endoglycosidase used to increase the dispersion and absorption of coadministered drugs via subcutaneous drug delivery.
Phesgo is administered subcutaneously (SC) into the thigh by a healthcare professional at either a treatment center or in a patient's home. It is administered over approximately 8 minutes for the initial loading dose and approximately 5 minutes for each subsequent maintenance dose.
"...it makes the treatment process more efficient for patients, to be able to receive a drug subcutaneously instead of intravenously. A home administration protocol for this subcutaneous formulation is an area of current research and can be advantageous for patients and infusion centers, especially during the current pandemic."
85% of patients (n=136 out of 160) preferred Phesgo SC ...
https://clinicaltrials.gov/ct2/show/NCT03674112?term=PHranceSCa&draw=2&rank=1
ClinicalTrials.gov Identifier: NCT03674112
-
Efficacy and Safety of T-DM1 + Capecitabine vs T-DM1 Alone in Previously Treated ERBB2+ Metastatic Breast Cancer
- JAMA Oncology
-
FDA OKs Bavencio as first-line bladder cancer therapy
Bavencio, or avelumab, Pfizer and Merck's immunotherapy, was approved by the FDA as a maintenance treatment for patients who have locally advanced or metastatic bladder cancer whose disease didn't progress after undergoing first-line platinum-containing chemotherapy.
Avelumab is already approved in bladder cancer patients whose disease has progressed following chemotherapy. Bavencio has been approved for maintenance treatment of patients with locally advanced or metastatic urothelial carcinoma that has not progressed with first-line platinum containing chemotherapy. Avelumab is indicated for the treatment of metastatic Merkel cell carcinoma (MCC).
BAVENCIO® (avelumab) is the FIRST and ONLY FDA-approved human anti-PD-L1 immunotherapy with DUAL ENGAGEMENT of both the adaptive and innate immune systems. BAVENCIO has been shown to release the suppression of the T cell-mediated antitumor immune response by blocking the interaction of PD-L1 with PD-1 receptors in preclinical models. BAVENCIO has also been shown to induce NK cell-mediated direct tumor cell lysis via antibody-dependent cell-mediated cytotoxicity (ADCC) in vitro.
https://pharmaphorum.com/news/fda-approves-pfizer-merck-kgaas-bavencio-in-first-line-bladder-cancer/
{Avelumab is currently being studied as a therapy for HER2+ MBC in the Aviator clinical trial.}
-
Efficacy and Safety of T-DM1 + Capecitabine vs T-DM1 Alone in Previously Treated ERBB2+ Metastatic Breast Cancer
- The authors of this phase I/II randomized clinical trial of 161 patients with previously treated ERBB2-positive metastatic breast cancer compared trastuzumab emtansine (T-DM1) with T-DM1 plus capecitabine. The overall response rate was numerically higher with combination therapy (44% vs 36%; P = .34). The median progression-free survival was similar between groups. Toxicity was higher with the addition of capecitabine, and more patients discontinued treatment due to adverse events in the combination arm compared with the T-DM1 monotherapy arm.
- Chemotherapy adds only modest potential benefit to T-DM1 while increasing toxicity.
- Adding capecitabine to T-DM1 did not statistically increase ORR associated with T-DM1 in patients with previously treated ERBB2-positive mBC. The combination group reported more AEs, but with no unexpected toxic effects.
doi:10.1001/jamaoncol.2020.1796{For the sake of clarity, it seems that HER2+ breast cancer is now being called ERBB2-positive breast cancer. I think it is a more specific reference to the mutation that causes the problem (uncontrolled growth) but I haven't seem a concise explanation for the change in practice.} -
EMA speeds review of AZ, Daiichi Sankyo HER2 drug Enhertu
The European Medicines Agency will fast-track its review of AstraZeneca and Daiichi Sankyo's HER2-positive breast cancer candidate Enhertu, or trastuzumab deruxtecan. The FDA approved the antibody drug conjugate as a treatment for metastatic HER2-positive disease in December.
http://www.pmlive.com/pharma_news/ema_fast-tracks_review_of_azdaiichi_sankyos_her2_drug_1344455
-
Wow Lumpie, that is very good news... I think a drug with such profile, if approved in EU, would be compensated in my country pretty soon (I mean in a year/few years). Hopefully... Saulius
-
just got this in my email
so I wasn’t aware of an immunohistochemical prognostic model score. Now there is a modified mICH4 that can possibly help doctors know if they should give hormone therapy or chemotherapy first.
Can anyone shed some light on this?
Dee
-
Acquired ESR1 Mutations Predict Poor Benefit from Further AI Therapy in Metastatic Breast Cancer
Patients with hormone receptor (HR) positive metastatic breast cancer who acquired ESR1 mutations during prior aromatase inhibitor therapy had worse survival when treated with the aromatase inhibitor exemestane compared with fulvestrant, a combined analysis of the phase 3 SoFEA and EFECT trials found. The results were recently reported in Clinical Cancer Research.
https://clinicaltrials.gov/ct2/show/NCT00065325
https://www.clinicaltrials.gov/ct2/show/NCT00253422
Turner NC, Swift C, Kilburn LS, et al. ESR1 mutations and overall survival on fulvestrant versus exemestane in advanced hormone receptor positive breast cancer: A combined analysis of the phase III SoFEA and EFECT trial [published online June 16, 2020]. Clin Cancer Res. doi: 10.1158/1078-0432.CCR-20-0224
-
Thanks, Lumpie. This is such good information. I'm glad we have so many eyes scouring the news.
-
BMI-Related Differential Benefit of Adjuvant Docetaxel in Early Breast Cancer
Journal of Clinical Oncology
TAKE-HOME MESSAGE
This retrospective analysis evaluated the impact of body mass index
(BMI) in patients with breast cancer treated with docetaxel-based versus
non–docetaxel based chemotherapy in a large adjuvant therapy trial.
A higher BMI was associated with worse disease-free survival and
overall survival among docetaxel-treated patients. No difference was
seen in the non–docetaxel treated patients. These findings of a
differential response to docetaxel according to BMI require validation
in an independent cohort.
– Paul J. Hampel, MDhttps://www.practiceupdate.com/content/bmi-related...
-
ASCO develops guideline for management of men with breast cancer
Research has led to major improvements in breast cancer diagnosis, treatment and survival. However, men with breast cancer represent only 1% of the U.S. breast cancer population and have not been emphasized in this research.
"Nearly all clinical trial participants have been women," Michael J. Hassett, MD, MPH, medical oncologist at Dana-Farber Cancer Institute and lead author of ASCO's guideline on management of male breast cancer, said in an interview with Healio. "When so few men have been included in the trials, it's hard to draw conclusions about how to treat men vs. women. Considering that more than 95% of breast cancers in men are hormone receptor positive, some have suggested that men and women with breast cancer should be treated differently."
-
Many negative trials presented with 'not-negative conclusions' at oncology meetings
Increased attention should be paid to the conclusions of formally negative trials discussed during oral presentations at oncology meetings, as many convey a not-negative message, according to a research letter published in JAMA Oncology.
"During [the 2019] ASCO Annual Meeting, several trials presented were considered formally negative according to their primary analysis, but they were presented with ambiguous and not-negative conclusions," Massimo Di Maio, MD, researcher in the department of oncology at University of Turin in Torino, Italy, told Healio. "My colleagues and I later decided to perform a systemic review to better understand the real magnitude of this phenomenon. We started with ASCO 2019, but later found that the proportion of those clinical trials was not negligible. We then extended the analysis to the [European Society for Medical Oncology] meeting, covering 3 years in total."
"Our aim was to be provocative," Di Maio said. "We do not want to be considered fundamentalists of clinical research methodology, because we ... know that even in a formally negative trial there could be many potentially important findings and many ideas for further research.
"...It would be interesting to compare the conclusions included in the oral presentation of these trials with the conclusions of their final publication in a peer-reviewed journal. It was too early to perform this analysis when we wrote this letter, but this could be an interesting follow-up."
-
A novel HER2-targeted antibody-drug conjugate offers the possibility of clinical dosing at trastuzumab-equivalent exposure levels
Molecular Cancer Therapeutics
Trastuzumab and the related antibody-drug conjugate (ADC), ado-trastuzumab emtansine (T-DM1), both target HER2-overexpressing cells. Together, these drugs have treatment indications in both early-stage and metastatic settings for HER2+ breast cancer. T-DM1 retains the antibody functionalities of trastuzumab and adds the potency of a cytotoxic maytansine payload. Interestingly, in the clinic, T-DM1 cannot always replace the use of trastuzumab plus chemotherapy administered together as single agents. We hypothesize that this failure may be due in part to the limited systemic exposure achieved by T-DM1 relative to trastuzumab because of toxicity-related dosing constraints on the ADC. We have developed a trastuzumab-based ADC site-specifically conjugated to maytansine through a noncleavable linker. This construct, termed CAT-01-106, has a drug-to-antibody ratio (DAR) of 1.8, approximately half the average DAR of T-DM1, which comprises a mixture of antibodies variously conjugated with DARs ranging from 0-8. The high DAR species present in T-DM1 contribute to its toxicity and limit its clinical dose. CAT-01-106 showed superior in vivo efficacy compared to T-DM1 at equal payload dosing and was equally or better tolerated compared to T-DM1 at equal payload dosing up to 120 mg/kg in Sprague-Dawley rats and 60 mg/kg in cynomolgus monkeys. CAT-01-106 also showed improved pharmacokinetics in rats relative to T-DM1, with 40% higher ADC exposure levels. Together, the data suggest that CAT-01-106 may be sufficiently tolerable to enable clinical dosing at trastuzumab-equivalent exposure levels, combining the functions of both the antibody and the payload in one drug and potentially improving patient outcomes.
https://www.meta.org/papers/a-novel-her2targeted-a...
DOI: 10.1158/1535-7163.mct-20-0190
-
[Tests in mice show] New therapy extends breast cancer survival rate, prevents reoccurrence
A new immunotherapy developed by researchers at Northwestern University dramatically extends the survival time of mice with triple negative breast cancer, one of the most aggressive and difficult-to-treat forms of breast cancer.
In a new study, mice treated with the therapy, which comprises two immunity-boosting drugs housed inside a nanoparticle, experienced complete tumor remission for at least 100 days. All untreated mice died by day 30. None of the treated mice experienced adverse side effects or autoimmune responses...
The research will be published online this week in the Proceedings of the National Academy of Sciences...
"It's definitely prolonging survival," Callmann noted. "Even if not all mice were completely cured."
Mirkin and his team also found that the SNA-based immunotherapy protected the mice from relapsing. After the mice entered remission, the team attempted to reimplant the mice with cancer, but tumors did not grow...
The researchers believe that, in theory, SNA-based immunotherapies should be an effective treatment for many types of cancer. Mirkin's team plans to explore that next. Mirkin notes that he feels encouraged that four SNA drugs are already in human clinical trials, including a variant of the SNA used in this study in a type of immunotherapy for Merkel Cell carcinoma. That structure also was invented at Northwestern and is in a Phase 2 clinical trial conducted by Exicure, a clinical stage biotechnology startup.
-
Antibody-drug conjugates in breast cancer: the chemotherapy of the future?
Current Opinion in Oncology
Abstract
Antibody-drug conjugates (ADCs) represent an interesting new class of anticancer agents, capable of exploiting the specificity of monoclonal antibodies toward cellular-antigens for a targeted release of potent cytotoxic drugs, with a potential increased activity and reduced toxicity compared with traditional chemotherapies. The aim of this article is to review the efficacy and safety of ADCs in breast cancer. Following the approval of T-DM1 both in early and advanced human epidermal growth factor receptor 2 (HER2)-positive breast cancer, novel anti-HER2 ADCs have been investigated. Some of these compounds, such as the recently FDA-approved trastuzumab deruxtecan, have shown relevant activity in T-DM1-pretreated patients, possibly thanks to the so-called bystander effect, namely the ability to exert cytotoxic activity also against antigen-negative cells. Such feature allows to overcome the HER2 intratumoral heterogeneity in breast cancer and could explain in the preliminary activity demonstrated also in HER2-low breast cancers. However, several ADCs targeting other cancer-associated antigens than HER2 are under development, representing a promising strategy for the treatment of triple-negative tumors, exemplified by the encouraging results of sacituzumab govitecan. ADCs are innovative and effective therapeutic drugs in breast cancer. Research efforts are ongoing to identify novel targets and combination with other treatment modalities, particularly with immunotherapy, to further improve patients' outcomes.
https://www.meta.org/papers/antibodydrug-conjugate...
DOI: 10.1097/cco.0000000000000656
-
As always, Lumpie, we appreciate you!!!!!
-
T-DM1 in Patients With HER2-Positive Metastatic Breast Cancer and Brain Metastases
- Annals of Oncology This exploratory final analysis of a phase IIIb trial was designed to evaluate the benefit of trastuzumab emtansine (T-DM1) for patients with HER2-positive breast cancer and brain metastases. Reduction in the sum of major diameters of brain metastases >30% occurred in 42.9% of patients. Significant intracranial responses were observed among 49.3% of those who had not received brain metastasis–directed radiotherapy.T-DM1 has good activity in this population, and further study is warranted.
https://www.practiceupdate.com/C/103466/56?elsca1=emc_enews_topic-alerthttps://www.annalsofoncology.org/article/S0923-7534(20)39930-0/fulltext# DOI:https://doi.org/10.1016/j.annonc.2020.06.020CONCLUSION: This exploratory analysis of patients with HER2-positive MBC and BM enrolled in a prospective clinical trial shows that T-DM1 is active and well-tolerated in this population. T-DM1 should be explored further in this setting.
-
I found this article about specific mutations
MRE11-RAD50-NBS1 complex alterations and DNA damage response: implications for cancer treatment
https://molecular-cancer.biomedcentral.com/articles/10.1186/s12943-019-1100-5
I’m sharing it with my MO because I have MRE11a somatic mutation.
Dee
-
'Liquid biopsy' tech contributes to successful clinical trial for detecting breast cancer recurrence
"These circulating markers were more predictive of relapse than any other commonly used clinical marker on the planet," Radovich said. "It's more predictive than tumor size, grade, stage or lymph node status."
"This is the largest clinical study ever published on the use of circulating markers and minimal residual disease," Radovich said. "This really puts it on the map."
-
fascinating
-
I’m glad liquid biopsies are getting traction!
I have had 2 liquid biopsies with zero results, since metastatic. Very odd but I guess it happens. Had to move onto a tissue biopsy.
Dee
-
Neratinib Plus Capecitabine in HER2+ MBC Previously Treated With ≥2 HER2-Directed Regimens
- Journal of Clinical Oncology This international, randomized, phase III trial was designed to evaluate capecitabine with either neratinib (an irreversible pan-HER TKI) or lapatinib (a reversible dual EGFR and HER2 TKI) in 621 patients with HER2-positive, metastatic breast cancer, including approximately 16% with brain metastases. Patients must have been previously treated with two or more HER2-directed regimens for metastatic breast cancer, although only 35% had received prior trastuzumab, pertuzumab, and T-DM1. Neratinib plus capecitabine led to a significantly improved progression-free survival (a co-primary endpoint) compared with lapatinib plus capecitabine (HR, 0.76; mean PFS difference of 2.2 months). There was no significant difference in overall survival (a co-primary endpoint) between groups (mean, 24.0 vs 22.0 months). Time to CNS disease intervention and duration of response also favored the neratinib treatment group. Diarrhea and nausea toxicities were numerically higher in the neratinib group, but discontinuation rates and quality-of-life assessments were similar.This trial is the first to demonstrate superior clinical outcomes of a particular HER2-directed TKI compared with another in the metastatic setting, and establishes neratinib plus capecitabine as an appropriate treatment option for this patient population.
DOI: 10.1200/JCO.20.00147 Journal of Clinical Oncology -
Fascinating about the liquid biopsies. Thanks, Debbie for sharing.
Thanks too, Lumpie, for the Neratinib trial. Always on the lookout for tx possibilities.
-
Lumpie I ran across this today and thought it might be of interest to someone.
Here's another https://www.goodnewsnetwork.org/cancer-vaccine-eliminates-97-tumors-amazing-success-human-trials-next/
-
Gussy: Thanks for sharing that - it does sound interesting.
For others who want highlights:
Larotrectinib is an oral drug that received accelerated breakthrough status after it displayed remarkable success in treating adult and pediatric cancers that currently have no satisfactory alternative treatments or have progressed following treatment. This is the second ever FDA-approved drug that treats cancers based on a certain genetic trait, regardless of the patient's age or cancer type, and it is the first drug to ever treat cancers that contain the specific NTRK gene that is present in several common forms of adult cancer and many forms of rare pediatric cancers. NTRK fusions are rare, but can occur in salivary gland, lung, breast, and thyroid cancers, as well as soft tissue sarcoma – and prior to this week's FDA approval, there had been no treatment for many of the cancers that frequently expressed this mutation.
Here is the FDA announcement: https://www.fda.gov/news-events/press-announcements/fda-approves-oncology-drug-targets-key-genetic-driver-cancer-rather-specific-type-tumor
-
Lumpie, do you know if any of the common genetic tests (foundation etc) look for the mutation that Larotrectinib targets?
-
Yes. Looks like Foundation One screens for it.
Here is their list:
I also found all 3 NTRK alterations on the Strata Oncology test list - so it appears that Strata tests for these alterations as well.
Addendum: These tests generally recommend drugs that treat cancer with the genomic finding. So it would be interesting to hear whether this drug is now being recommended. I looked at my results from Strata but, since I did not have any of these alterations, I didn't get any associated recommendations. Strata (in theory) tells you drugs in clinical trial for the alteration, but... that part did not appear to be a perfect process. I know of one drug off the top of my head that was in stage 3 trials at the time my test was run but was left off the list of clinical trial drugs (DS-8201a AKA Enhertu). In fact, they did not recommend any clinical trial drugs. In fairness, Strata was still in clinical trial phase at that point so maybe they had not fully implemented that function yet.
-
Thank you! You're a gem keeping us utd on all this!
-
Lumpie, thanks so much for this.
Two things: I went back and checked the list of genes for which Foundation One tested in Jan of 2019 on my own results, and it appears that the number is the current number tested is the same on the link you provided. I was hoping that they might have added a lot of new genes, but it doesn't appear to be the case. Here's the list from my Jan 2019 test. Maybe I didn't look carefully enough:

Second, on my own test results, I found that I have NTRK1 amplification. I got excited and thought that this might be an option for me. However, per the article below I found, this drug works most specifically to fusions rather than other modifications:
-
Interesting article from Science News today about the effectiveness of an immunotherapy plus a vaccine currently being trialed (phase 2) at Duke -- currently for Her2+ use.
https://scienmag.com/investigational-breast-cancer...
-
JoynerL - That list is huge. I need to go back and look at results from genetic test my DR ordered Sept 2019. No known markers were found, but I thought she said 20-30 known markers were looked at. Your list looks much larger. I think she said the test was specific to BC. Insurance so far has denied to claim, saying it is not relevant to diagnosis or treatment. I think the lab is going to pick up most of the cost.
-
BlueGirlRedState,
Foundation One testing is genomic testing -- testing of the tumor and changes within the tumor (tumor cells can change during cancer evolution) -- not genetic (what you are born with) testing. I had trouble in 2016 getting my insurance to pick up genetic testing. Genomic testing, on the other hand, is FDA approved and I know that Medicare covers it -- that means that most insurance companies, that take their cues from Medicare, will cover as well.
-
This article is relevant for both early and advanced cancers, with some interesting info relevant specifically to tamoxifen users. This is only an abstract but if you follow the link to the publisher ("Nature") there's somewhat more info as well as an option to purchase the article itself for $8.99, which seems pretty reasonable to me, particularly compared to some fees for such articles.
"Fasting-Mimicking Diet and Hormone Therapy Induce Breast Cancer Regression"
-
you can see the text for free here https://www.researchgate.net/publication/342967885_Fasting-mimicking_diet_and_hormone_therapy_induce_breast_cancer_regression
-
BevJen - Thanks for that link. I find the vaccine studies fascinating and promising. Nothing better than out immune system to fight bad cells. We just have to teach the body to recognize Cancer cells as bad and attack them. 😃
-
Indigenous American Ancestry Tied to HER2+ Breast Cancer
Higher proportion of Indigenous American ancestry associated with a greater incidence of HER2+ breast cancer
- HealthDay TUESDAY, July 28, 2020 (HealthDay News) -- Indigenous American (IA) origin could partly contribute to the higher incidence of human epidermal growth factor receptor 2-positive (HER2+) breast cancer in Latinas, according to a study recently published in Cancer Research.Katie M. Marker, M.P.H., from the University of California in San Francisco, and colleagues evaluated genomewide genotype data for 1,312 patients participating in the Peruvian Genetics and Genomics of Breast Cancer Study to estimate genetic ancestry. The association between HER2 status and genetic ancestry was evaluated with findings replicated in 616 samples from Mexico and Colombia.The researchers found that the odds of having a HER2+ tumor increased by a factor of 1.20 with every 10 percent increase in IA ancestry proportion. In samples from Mexico and Colombia, this association between HER2 status and IA ancestry was independently replicated."The positive association between Indigenous American genetic ancestry and HER2+ breast cancer suggests that the high incidence of HER2+ subtypes in Latinas might be due to population and subtype-specific genetic risk variants," the authors write.https://www.practiceupdate.com/C/104315/56?elsca1=emc_enews_topic-alerthttps://cancerres.aacrjournals.org/content/80/9/1893DOI: 10.1158/0008-5472.CAN-19-3659 Published May 2020
-
Thank you, moth, for the Research Gate link to the article
-
Burden of Pre-, Postmenopausal Breast Cancer Up Worldwide
Countries with very high HDI have highest pre- and postmenopausal breast cancer incidence
- HealthDay TUESDAY, July 28, 2020 (HealthDay News) -- There is evidence of an increasing burden of premenopausal and postmenopausal breast cancer worldwide, according to a study published in the August issue of The Lancet Global Health.Emily Heer, from Alberta Health Services in Calgary, Canada, and colleagues conducted a population-based analysis of global breast cancer incidence and mortality among premenopausal and postmenopausal women.The researchers found that in 2018, about 645,000 premenopausal and 1.4 million postmenopausal breast cancer cases were diagnosed worldwide; in each menopausal group, there were more than 130,000 and 490,000 deaths, respectively. Compared with higher-income countries, countries with a low United Nations Development Programme human development index (HDI) faced a greater burden of premenopausal breast cancer for both new cases and deaths. The highest premenopausal and postmenopausal breast cancer incidence was seen for countries with a very high HDI (30.6 and 253.6 cases per 100,000, respectively), while the highest premenopausal and postmenopausal mortality was seen for countries with low and medium HDI (8.5 and 53.3 deaths per 100,000, respectively). Significantly increasing age-standardized incidence rates were seen for premenopausal and postmenopausal breast cancer in 20 and 24 of 44 populations, respectively. Growth exclusively at premenopausal ages mainly occurred in high-income countries, while in countries under transition, the increasing premenopausal breast cancer burden was most notable."Our study provides evidence of a rising burden of both premenopausal and postmenopausal breast cancer worldwide and wide inequities in breast cancer care," the authors write.https://www.practiceupdate.com/C/104327/56?elsca1=emc_enews_topic-alerthttps://www.thelancet.com/journals/langlo/article/PIIS2214-109X(20)30215-1/fulltextDOI:https://doi.org/10.1016/S2214-109X(20)30215-1Related editorial: https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(20)30307-7/fulltextDOI:https://doi.org/10.1016/S2214-109X(20)30307-7
-
Metastatic Breast Cancer and Pseudocirrhosis
- ESMO open In this retrospective study of 48 women with metastatic breast cancer to the liver, the authors analyzed patient characteristics and assessed the prevalence of complications associated with decompensated cirrhosis. There was a trend toward more patients with luminal cancer in this sample compared with the hospital cancer registry. Of these patients, 47 had widespread liver invasion and 28 had ascites, including 18 with ascites classified as transudate. Esophageal varices were observed in 11 patients, with 3 experiencing rupture. Cisplatin and 5-fluorouracil were most frequently used at the time of liver contour abnormality appearance. Approximately half of the patients achieved a partial response.These findings suggest that pseudocirrhosis develops at the expense of a substantial burden of liver disease and commonly with 5-fluorouracil, with or without cisplatin, and may follow treatment response.
Commentary by Lillie D Shockney RN, BS, MAS, ONN-CGA subset of metastatic breast cancer patients may manifest pseudocirrhosis; however, we would need to know if all radiologists report this finding. Radiologists commonly measure the increase in the size of known lesions in the liver or report new lesions; however, they might not be noting this additional anatomic finding. -
JoynerL: Thanks for sharing that about checking your Foundation One test info from 2019. That is also really interesting that "this drug works most specifically to fusions rather than other modifications." I would not have realized that from what I read in the prior article.
-
Independent Prognostic Factors and Treatment Modality Associated With Survival and Recurrence in Breast Cancer
JAMA Network Open
- The authors of this study of 956 women with invasive breast cancer evaluated the independent prognostic performance of various clinical and molecular variables (age, tumor size, nodal status, high tumor grade, p53 status, estrogen receptor status, ERBB status) by specific treatment.
- The performance of these factors was weighted by the specific treatment and outcome category.
Published: July 9, 2020. doi:10.1001/jamanetworkopen.2020.7213{Kind of technical. If you like parsing this minutia, this may be of interest. Open access to article.} -
BevJen - thank you for explanation.
-
Bev-Jen, thanks for that article. I guess that would be a one-shot treatment, wow, if effective, that is a game changer for HER-2. No more being tied to every-three-weeks-at-the-cancer-center.
-
Olma.
Yes, it sounds very interesting. Hopefully they will get good results from the trial.
-
Moth, thanks for the heads up on the Research Gate link. Your grateful neighbor to the south salutes you.
-
Survival Outcomes by TP53 Mutation Status in Metastatic Breast Cancer
Purpose
To determine the significant genomic alterations in patients with metastatic breast cancer (MBC) and survival outcomes in common genotypes.
Patients and MethodsHigh-depth next-generation sequencing was performed for 202 genes in tumor and normal DNA from 257 patients with MBC, including 165 with estrogen receptor/progesterone receptor–positive and human epidermal growth factor receptor 2 (HER2 [hormone receptor positive (HR+)])–positive, 32 with HER2-positive, and 60 with triple-negative (estrogen receptor/progesterone receptor–negative and HER2-negative) disease. Kaplan-Meier survival analysis was performed in the discovery set, in patients with breast cancer analyzed in The Cancer Genome Atlas, and in a separate cohort of 98 patients with MBC who underwent clinical genomic testing.
ResultsSignificantly mutated genes (SMGs) varied by histology and tumor subtype, but TP53 was an SMG in all three subtypes. The most SMGs in patients with HR+ cancer were PIK3CA (32%), TP53 (29%), GATA3 (15%), CDH1 (8%), MAP3K1 (8%), PTEN (5%), TGFBR2 (4%), AKT1 (4%), and MAP2K4 (4%). TP53 mutations were associated with shorter recurrence-free survival (P = .004), progression-free survival (P < .001), and overall survival (P = .003). Furthermore, TP53 status was prognostic among patients with HR+ cancer with PIK3CA mutations. TP53 mutations were associated with poorer overall survival in the 442 patients with HR+ breast cancer analyzed in The Cancer Genome Atlas (P = .042) and in an independent set of 96 patients with HR+ MBC who underwent clinical sequencing (P < .001).
ConclusionSignificantly mutated genes (SMGs) differ by tumor subtype, but TP53 is significantly mutated in all three breast cancer subtypes. TP53 mutations are associated with poor prognosis in HR+ breast cancer and should be considered in the design and interpretation of precision oncology trials.
Other points of interest:
GATA3 alterations were mutually exclusive with TP53 alterations.
The authors concluded that HR+ tumors with TP53 mutations are mostly aromatase inhibitor resistant and would be more appropriately treated with other modalities. However, we do not know whether other regimens would be more effective for these tumors or whether TP53 mutations would equally confer resistance to other agents.
https://ascopubs.org/doi/10.1200/PO.17.00245
DOI: 10.1200/PO.17.00245 JCO Precision Oncology - published online April 25, 2018
-
Four-stranded DNA structures found to play role in breast cancer
...These structures form in regions of DNA that are rich in one of its building blocks, guanine (G), when a single strand of the double-stranded DNA loops out and doubles back on itself, forming a four-stranded 'handle' in the genome. As a result, these structures are called G-quadruplexes...
During the process of DNA replication and cell division that occurs in cancer, large regions of the genome can be erroneously duplicated several times leading to so-called copy number aberrations (CNAs). The researchers found that G-quadruplexes are prevalent within these CNAs, particularly within genes and genetic regions that play an active role in transcription and hence in driving the tumour's growth.
..."The abundance and location of G-quadruplexes in these biopsies gives us a clue to their importance in cancer biology and to the heterogeneity of these breast cancers," added Dr Robert Hänsel-Hertsch who is now at the Center for Molecular Medicine Cologne, University of Cologne, and is first author on the publication.
"Importantly, it highlights another potential weak spot that we might use against the breast tumour to develop better treatments for our patients."
...By targeting the G-quadruplexes with synthetic molecules, it may be possible to prevent cells from replicating their DNA and so block cell division, halting the runaway cell proliferation at the root of cancer. The team identified two such molecules - one known as pyridostatin and a second compound, CX-5461, which has previously been tested in a phase I trial against BRCA2-deficient breast cancer.
https://www.eurekalert.org/pub_releases/2020-08/uoc-fds073120.php
-
The 'Dynamic Space' of HER2 Breast Cancer Treatment Strategies
More evident than ever that one-size-fits-all approach is less likely to work
A review by Danielle File, MD, and colleagues in the ASCO Educational Book highlights the recent advances in treatment and discusses how the clinical landscape is shifting toward tailored therapies based on disease characteristics and biomarkers.
Early stage HER2 breast cancer treatment strategies have proven to be a dynamic space and it's more evident that a "one size fits all" approach is less likely to work and should be tailored to the patient by considering anatomic and biological risk.
Read the paper here and an interview about it here.
Primary Source: ASCO Educational Book
-
Stage IV Stampede!
Reminder to anyone interested who has not yet registered.... there is still time! The Stampeded is going virtual! **August** is Stampede month. The Stage IV Stampede is part of a grassroots advocacy effort designed to advocate for MBC priorities with members of Congress. Join us, bring friends and family - anyone who might advocate with us. Help educate members of Congress about priorities for the MBC community. No experience necessary! {cross posting}
Thanks for your indulgence of the PSA....
-
Aug 1, 2020
Stimulation of Oncogene-Specific Tumor-Infiltrating T Cells through Combined Vaccine and αPD-1 Enable Sustained Antitumor Responses against Established HER2 Breast Cancer
Abstract
Despite promising advances in breast cancer immunotherapy, augmenting T-cell infiltration has remained a significant challenge. Although neither individual vaccines nor immune checkpoint blockade (ICB) have had broad success as monotherapies, we hypothesized that targeted vaccination against an oncogenic driver in combination with ICB could direct and enable antitumor immunity in advanced cancers. Our models of HER2+ breast cancer exhibit molecular signatures that are reflective of advanced human HER2+ breast cancer, with a small numbers of neoepitopes and elevated immunosuppressive markers. Using these, we vaccinated against the oncogenic HER2Δ16 isoform, a nondriver tumor-associated gene (GFP), and specific neoepitopes. We further tested the effect of vaccination or anti-PD-1, alone and in combination. We found that only vaccination targeting HER2Δ16, a driver of oncogenicity and HER2-therapeutic resistance, could elicit significant antitumor responses, while vaccines targeting a nondriver tumor-specific antigen or tumor neoepitopes did not. Vaccine-induced HER2-specific CD8+ T cells were essential for responses, which were more effective early in tumor development. Long-term tumor control of advanced cancers occurred only when HER2Δ16 vaccination was combined with αPD-1. Single-cell RNA sequencing of tumor-infiltrating T cells revealed that while vaccination expanded CD8 T cells, only the combination of vaccine with αPD-1 induced functional gene expression signatures in those CD8 T cells. Furthermore, we show that expanded clones are HER2-reactive, conclusively demonstrating the efficacy of this vaccination strategy in targeting HER2. Combining oncogenic driver targeted vaccines with selective ICB offers a rational paradigm for precision immunotherapy, which we are clinically evaluating in a phase II trial (NCT03632941).
https://pubmed.ncbi.nlm.nih.gov/32732224/
{Exciting that this is in clinical trial phase.} -
Sequencing Endocrine Therapy for Metastatic Breast Cancer: What Do We Do After Disease Progression on a CDK4/6 Inhibitor?
I recently asked my MO to download this article for me so I didn't have to pay for it. Just got it today.
(maybe others can get your MO to download these articles that charge fees. )It has great info for what could be next if you fail a cdk4/6 and what could be driving resistance. It listed several trials by number and offered some hope for triplet therapy (3 drugs together)Dee -
Thanks, AlabamaDee. Another hint regarding accessing journals: if you have a kid in college who has access to an academic library, they may have access, too. Friend who has gone back to school? Same. At our community college, it is not easy, but members of the public could get limited access to the health sciences library. And ask at your public library, too. With all the COVID stuff, sometimes remote access to databases has been liberalize. Even your local hospital. It has a medial library. How open it is to the public varies. And right now it is probably restricted. College alumna? Call your alma mater and ask their librarian if there is any access for alumni... sometimes you gotta pull out all the stops.
-
Low-Dose Metronomic Chemotherapy as an Efficient Treatment Option in Metastatic Breast Cancer
- In this retrospective study of patients with metastatic breast cancer (MBC), the efficacy of low-dose metronomic chemotherapy (LDMC) was compared with that of conventional chemotherapy (CCT). Disease control rate longer than 24 weeks was the primary endpoint, and it was reached by 30.0% of patients receiving LDMC and 22.5% of those receiving CCT. Median progression-free survival was 12 weeks in both treatment arms. Disease control rates were 40.0% (LDMC) versus 25.0% (CCT) in younger patients, 33.3% (LDMC) versus 25.0% (CCT) in non–heavily pretreated patients, and 36.0% (LDMC) versus 18.0% (CCT) in patients without multiple metastases. Similar efficacy was also observed among patients with HR-positive and triple-negative disease.
- These results demonstrate comparable efficacy of LDMC and CCT in patients with MBC, suggesting that LDMC may be a valuable treatment option in a select patient population.
Note: LDMC is defned as a continuous administration of cytotoxic drugs at low doses, distinctly lower than the maximum tolerable dose (MTD) of conventional chemotherapy (CCT)Breast Cancer Research and Treatment (2020) 182:389–399 https://doi.org/10.1007/s10549-020-05711-5 -
Shallow Whole-Genome Sequencing From Plasma Identifies FGFR1-Amplified Breast Cancers and Predicts OS
- In this study of formalin-fixed paraffin-embedded tissue samples from 100 patients with metastatic breast cancer, the authors sought to investigate the utility of cell-free DNA for the evaluation of FGFR1 copy number. FGFR1 amplifications were identified via tissue-based analyses in 20 tumors. Of these, 12 tumors with a ctDNA allele fraction above 3% demonstrated concordance for FGFR1 status between cell-free DNA and tissue. High ctDNA levels were associated with poor prognosis.
- These findings suggest that ctDNA may be used to identify patients who will respond to FGFR inhibition, and ctDNA analysis may indicate prognosis in clinical trials.
- Background: Focal amplification of fibroblast growth factor receptor 1 (FGFR1) defines a subgroup of breast cancers with poor prognosis and high risk of recurrence. We sought to demonstrate the potential of circulating cell-free DNA (cfDNA) analysis to evaluate FGFR1 copy numbers from a cohort of 100 metastatic breast cancer (mBC) patients.
- Conclusions: Screening for FGFR1 amplification in ctDNA might represent a viable strategy to identify patients eligible for treatment by FGFR inhibition, and mBC ctDNA levels might be used for the evaluation of prognosis in clinical drug trials.
Cancers 2020, 12(6), 1481; https://doi.org/10.3390/cancers12061481 -
Quantifying the Impact of Axillary Surgery and Nodal Irradiation on Breast Cancer–Related Lymphedema and Local Tumor Control
- Journal of Clinical Oncology The authors of this prospective study of 1815 patients with invasive breast cancer evaluated the impact of axillary surgical extent and lymph node radiation on breast cancer–related lymphedema rates. Breast cancer–related lymphedema rates were lower at 5 years among patients with sentinel lymph node biopsy with or without regional lymph node radiation compared with those with axillary lymph node dissection with or without regional lymph node radiation. Tumor control rates were similar in the two groups.The type of axillary surgery appears to be the major determinant of breast cancer–related lymphedema.
Although RLNR adds to the risk of lymphedema, the main risk factor is the type of axillary surgery used.DOI: 10.1200/JCO.20.00459 Journal of Clinical OncologyPublished online July 30, 2020.PMID: 32730184 -
Cancer-Related Fatigue in {Early Stage} Breast Cancer Survivors
- The authors reviewed cancer-related fatigue (CRF) among breast cancer survivors. CRF was highest among young women, obese women, and women with diabetes. Women with CRF were more likely than women without to report pain, depression, insomnia, and cognitive dysfunction. Coping strategies appeared to impact the risk of CRF. CRF was not associated with tumor characteristics, previous treatments, and physical activity. CRF predicted quality of life.
- More awareness and education are needed to allow clinicians to effectively address the frequent problem of CRF among breast cancer survivors.
Fatigue is the most distressing and frequent symptom in Breast Cancer (BC) survivors after treatment. Although fatigue can be found in other cancer survivors, women with a history of breast cancer may share some distinctive features. This study aims to recapitulate the knowledge about risk factors and correlates of cancer-related fatigue (CRF) in BC survivors after oncological therapy. An electronic literature search was conducted in PubMed using the terms "fatigue", "breast", "cancer", and "survivors". Records were included if they were original articles, available in English, used a quantitative scale, had more than 100 participants, and excluded women who had relapsed. BC survivors should have finished their treatments at least 2 months before, except for hormonal therapy. Physiopathology or interventions were considered beyond the scope of this review. Correlates were subsequently classified into seven main categories: 1) sociodemographic, 2) physical variables, 3) tumour- and treatment-related, 4) comorbidities, 5) other symptoms, 6) psychological and 7) lifestyle. Notably, fatigue was consistently higher in younger, obese and diabetic women. Women reporting fatigue often communicated symptoms such as pain, depression, insomnia and cognitive dysfunction. Coping strategies such as catastrophising could play an important role in the persistence of fatigue. However, tumour characteristics, previous treatments and physical activity were not consistently related. CRF was a strong predictor of quality of life in BC survivors after treatment. To conclude, CRF is a frequent and serious symptom that severely affects the quality of life of BC survivors after treatment. More awareness and information among health practitioners is needed. -
Aromatase Inhibitor Symptom Management Practices
- This retrospective study was designed to compare aromatase inhibitor (AI) symptom management practices among 179 women with hormone receptor–positive breast cancer. AI-related symptoms were documented in 82% of patients, but just over half of these received guideline-based management.
- Only around half of patients with AI-related symptoms received guideline-based treatment.
PURPOSE
Aromatase inhibitor (AI) associated symptoms are large contributors to early discontinuation. Though guidelines exist for management of these symptoms, little is known about the degree to which physicians address symptoms and adhere to the guidelines for treatment.
PATIENTS
In this retrospective chart review, 179 women with hormone receptor positive breast cancer who were prescribed an AI between October 15, 2012 and September 14, 2017 were randomly selected from the institution's National Association of Central Cancer Registry.
RESULTS
Among 179 women prescribed an AI, 82% had at least one symptom and 46% had multiple symptoms. Of the 147 women with any documented symptom, 97 (66%) received some form of symptom-palliating treatment. Seventy-seven patients (52%) received guideline-based treatments or guideline-based treatments in combination with non-guideline based treatments. There were no differences in receipt of treatment overall (i.e. guideline or non-guideline-based for either vasomotor musculoskeletal by age, race, or stage.
CONCLUSIONS
Although 82% of patients had symptoms documented in their medical records, just over half of those patients received guideline-based treatment.
https://www.practiceupdate.com/C/104124/56?elsca1=emc_enews_topic-alert
https://www.clinical-breast-cancer.com/article/S1526-8209(20)30174-9/pdf
-
Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial
PURPOSE The oligometastatic paradigm hypothesizes that patients with a limited number of metastases may achieve long-term disease control, or even cure, if all sites of disease can be ablated. However, long-term randomized data that test this paradigm are lacking.
METHODS We enrolled patients with a controlled primary malignancy and 1-5 metastatic lesions, with all metastases amenable to stereotactic ablative radiotherapy (SABR). We stratified by the number of metastases (1-3 v 4-5) and randomized in a 1:2 ratio between palliative standard-of-care (SOC) treatments (arm 1) and SOC plus SABR (arm 2). We used a randomized phase II screening design with a primary end point of overall survival (OS), using an a of .20 (wherein P , .20 indicates a positive trial). Secondary end points included progressionfree survival (PFS), toxicity, and quality of life (QOL). Herein, we present long-term outcomes from the trial.
RESULTS Between 2012 and 2016, 99 patients were randomly assigned at 10 centers internationally. The most common primary tumor types were breast (n 5 18), lung (n 5 18), colorectal (n 5 18), and prostate (n 5 16). Median follow-up was 51 months. The 5-year OS rate was 17.7% in arm 1 (95% CI, 6% to 34%) versus 42.3% in arm 2 (95% CI, 28% to 56%; stratified log-rank P 5 .006). The 5-year PFS rate was not reached in arm 1 (3.2%; 95% CI, 0% to 14% at 4 years with last patient censored) and 17.3% in arm 2 (95% CI, 8% to 30%; P 5 .001). There were no new grade 2-5 adverse events and no differences in QOL between arms.
CONCLUSION With extended follow-up, the impact of SABR on OS was larger in magnitude than in the initial analysis and durable over time. There were no new safety signals, and SABR had no detrimental impact on QOL.
CONTEXT
Key Objective: To determine the impact of stereotactic ablative radiotherapy (SABR) on overall survival (OS) in patients with a controlled primary tumor and 1-5 oligometastases.
Knowledge Generated: In this long-term report from an international randomized phase II trial, patients who received SABR demonstrated a 22- month improvement in median OS compared with patients who received a standard-of-care approach alone, corresponding to an absolute survival benefit of 25% at 5 years. There were no new safety signals detected.
Relevance: These data add to the growing evidence base that suggests that SABR can improve long-term outcomes in patients with a limited burden of metastatic disease. These results may influence treatment decisions while awaiting the results of phase III trials.
CLINICAL TRIAL INFORMATION NCT01446744
https://ascopubs.org/doi/pdf/10.1200/JCO.20.00818
DOI: 10.1200/JCO.20.00818 Journal of Clinical Oncology Published online June 02, 2020.
{Wow. These are HUGE improvements. It is a small study, so that has to be taken into account. If you are oligometastatic, be sure your doctor is up to date on this research. Free access to full article on ASCO website.}
-
Cumberlege review exposes stubborn and dangerous flaws in healthcare {re NHS}
Editorial
On 8 July the Conservative peer Julia Cumberlege published her much anticipated Independent Medicines and Medical Devices Safety Review, looking into the response of England's healthcare system to patients' reports of harm from drugs and medical devices.
The Cumberlege review was inspired by longstanding patient campaigns alleging harm from these three interventions, and the panel's explicitly declared approach was that patients' and families' voices, experiences, and views should be "at the heart of the review."
The Cumberlege review made nine recommendations {including} a dedicated patient safety commissioner to help patients navigate the bureaucratic tangle and to troubleshoot problems throughout the system, has generated interest both inside and outside England. It is clearly the panel's centrepiece, characterised as a "golden thread" tying the disjointed system together in the interest of patients. Other recommendations include a Redress Agency to provide remediation to victims of medical harm without forcing them to litigation; schemes and specialist centres to provide care, support, and treatment; reform of the approval and tracking process for drugs and devices; and a public list of doctors' conflicts of interests, to be run by the General Medical Council.
the report .... has the potential to extend its influence far beyond the UK.
https://www.bmj.com/content/370/bmj.m3099
BMJ 2020; 370 doi: https://doi.org/10.1136/bmj.m3099 (Published 06 August 2020)Cite this as: BMJ 2020;370:m3099
{Matters related to patient safety often do not get the attention they deserves. I would be interested to hear whether this report has gotten much attention on the "other side of the pond."}
-
Lumpie as always thanks for what you do!
Re the Cumberlege report, there was significant recent media coverage of the case surrounding the use of pelvic mesh and the fact that patients who suffer extensive harm from it’s use had basically been ignored as ‘ women’s problems’. NHS issued an unprecedented public apology and the report was cited as a catalyst for change in how patients are advocated for and listened to. -
Lumpie and Karen,
This is fascinating stuff. Thanks, Lumpie, for posting.
-
Lumpie - thank you for your posts on lymphedema and AIs. AIs definitely have SEs, and I don't think DRs know much about managing them. I have BC for the third time, twice left breast, and now R-axilla. Even though Ibrance is shrinking the tumor, oncologist suggested I look at surgery, which terrifies me. I think the risks and SEs will be much worse than bi-lateral was. Tendons, nerves, muscles - and I already have lymphedema from the tumor. Just had a CT Thursday, really hoping for more shrinking. Radiation might be out since I had that in 2009 on Left side, whole breast.
-
BlueGirl,
If you were not radiated on the R side, radiation might still be a possibility. And they are getting much better at targeting radiation. So don't give up on that thought!
-
consider proton rads - very targeted
-
Novel Therapies in the Management of HER2-Positive Breast Cancer
- Interview with Reshma L. Mahtani DO
- 9 minute video offers overview of treatment options for both early stage and MBC HER2+ disease. There is discussion of new therapies and Dr. Mahtani briefly mentions HR+, HER2+ disease. Transcript provided, too.
- https://www.practiceupdate.com/C/101965/56?elsca1=emc_enews_topic-alert
-
Karenfizedbo15: Thanks for sharing insight on NHS situation. I hope that all of our health systems will pay more attention to patient concerns!
-
On the use of DNA as a linker in antibody-drug conjugates: synthesis, stability and in vitro potency
Here we present the synthesis and evaluation of antibody-drug conjugates (ADCs), for which antibody and drug are non-covalently connected using complementary DNA linkers. These ADCs are composed of trastuzumab, an antibody targeting HER2 receptors overexpressed on breast cancer cells, and monomethyl auristatin E (MMAE) as a drug payload. In this new ADC format, trastuzumab conjugated to a 37-mer oligonucleotide (ON) was prepared and hybridized with its complementary ON modifed at 5-end with MMAE (cON-MMAE) in order to obtain trastuzumab-DNA-MMAE. As an advantage, the cON-MMAE was completely soluble in water, which decreases overall hydrophobicity of toxic payload, an important characteristic of ADCs. The stability in the human plasma of these non-engineered ONbased linkers was investigated and showed a satisfactory half-life of 5.8 days for the trastuzumabDNA format. Finally, we investigated the in vitro cytotoxicity profle of both the DNA-linked ADC and the ON-drug conjugates and compared them with classical covalently linked ADC. Interestingly, we found increased cytotoxicity for MMAE compared to cON-MMAE and an EC50 in the nanomolar range for trastuzumab-DNA-MMAE on HER2-positive cells. Although this proved to be less potent than classically linked ADC with picomolar range EC50, the diference in cytotoxicity between naked payload and conjugated payload was signifcant when an ON linker was used. We also observed an interesting increase in cytotoxicity of trastuzumab-DNA-MMAE on HER2-negative cells. This was attributed to enhanced non-specifc interaction triggered by the DNA strand as it could be confrmed using ligand tracer assay.
https://www.nature.com/articles/s41598-020-64518-y.pdf
https://doi.org/10.1038/s41598-020-64518-y
Nature Scientific Reports | (2020) 10:7691 {open access}
{This article is pretty technical. I think that there is press reporting on it, too, which may be more reader friendly. I will post that if I can find it. In short... many of us are familiar with antibody drug conjugates, like Kadcyla aka T-DM1. It combines two drugs: Traztuzamab and DM1. They are "linked." Making the link stable is challenging. This article discussed a different method of linking drugs which may be more stable and may allow the linkage of more than two drugs.}
-
New class of precision medicine strips cancer of its DNA defenses
A new precision medicine targeting cancer's ability to repair its DNA has shown promising results in the first clinical trial of the drug class. The new study, designed to test the drug's safety, found that half of patients given the new drug either alone or with platinum chemotherapy saw their cancer stop growing, and two patients saw their tumours shrink or disappear completely.
A new precision medicine targeting cancer's ability to repair its DNA has shown promising results in the first clinical trial of the drug class.
The new study, designed to test the drug's safety, found that half of patients given the new drug either alone or with platinum chemotherapy saw their cancer stop growing, and two patients saw their tumours shrink or disappear completely.
Damage to the DNA in cells is the root cause of cancer -- but it is also a fundamental weakness in tumours, and cancer cells can be killed by further damaging their DNA or attacking their ability to repair it. The new phase I trial tested the first in a new family of drugs blocking a key DNA repair protein called ATR. Phase I trials are designed to assess the safety of new treatments, and it's unusual to see a clinical response at this stage.
The drug's benefit in blocking DNA repair was even more marked in patients also given chemotherapy, which works by causing DNA damage. In these patients, 15 of 21, or 71 per cent saw their disease stabilise -- suggesting that chemotherapy boosted sensitivity to berzosertib.
Story Source: Materials provided by Institute of Cancer Research.
-
BlueGirlRedState: I am so sorry about your dilemma. I loathe ambiguity... part of the reason I research ad nauseam. Surgery is scary. It seems to me that lymphedema results more often from removal of nodes than lesions, so if they are only talking about removing a tumor, that may be an advantage. My impression is that they are moving toward more neoadjuvant therapy so that less, or less extensive, surgery will be necessary. I think that if they find a way to do less node removal, there will be less lymphedema. I hope all goes well for you.
-
Trial Assessing Atezolizumab in Triple-Negative Breast Cancer Misses Endpoint
Genentech announced that the phase 3 study of atezolizumab in combination with paclitaxel for the first-line treatment of patients with metastatic triple-negative breast cancer (TNBC) did not meet its primary end point in the PD-L1-positive population.
Findings showed that the study did not meet statistical significance for PFS and also demonstrated a negative trend in overall survival (secondary end point) for patients in the atezolizumab plus paclitaxel arm. The study, however, was not powered for overall survival and data was immature at the time of analysis. The safety profile of atezolizumab was consistent with that seen in previous studies and no new safety signals were reported.
Atezolizumab is marketed under the brand name Tecentriq and is currently approved in combination with Abraxane (paclitaxel [protein-bound]; Celgene) for the treatment of unresectable locally advanced or metastatic TNBC in patients whose tumors express PD-L1. In June 2020, Genentech announced results from the IMpassion031 study evaluating Tecentriq plus Abraxane in patients with previously untreated, early TNBC. Results showed the combination therapy demonstrated a statistically significant and clinically meaningful improvement in pathological complete response, regardless of PD-L1 expression (primary end point).
Reference
- Genentech provides update on phase III study of Tecentriq in combination with paclitaxel for people with metastatic triple-negative breast cancer. https://www.businesswire.com/news/home/20200806005915/en/Genentech-Update-Phase-III-Study-Tecentriq-Combination. Accessed August 7, 2020.
-
Lumpie,
Thanks for posting. My center has been doing a trial with tecentriq for those with hormone positive cancer (no longer enrolling). I wonder what the implications are for that cohort. Atezo/tecentriq was all over my Foundation One report as a possible drug for me.
-
The other night I heard an interview from this ND, Nalini Chilkov, and was impressed. Her website might not be as impressive as the interview. https://www.integrativecanceranswers.com/dr-nalini-chilkov/ She stressed how she works with the oncologosts, has them focus on the cancer while she focuses on the patients health from the cancer and effects on treatments on health, making sure what she does is not interfering with what the oncologist does. If she was not in southern California, I would probably consult with her to see if she would take me on as a patient. . Another interview with Dr. Ralf Kleefon the same program was also interesting where hyperthermia is used sometimes in combination of lower doses of chemo drugs than the standard calls for. The particular treatment is ony allowed in 3 countries in Europe at this time, Germany, Austria, Sweeden. Here is an article, not the interview https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6469443/ It is tempting to try something other than the "standard of care" when you start having doubts about the standard.
-
Check out Dr Keith Block , The Block Center, chicago. He is MO who is ALSO an integrative doc. I thought he was wonderful.
-
Serial Analysis of CTCs in Patients With Metastatic Breast Cancer Receiving First-Line Chemotherapy
- Journal of the National Cancer Institute These authors evaluated the prognostic significance of circulating tumor cells (CTCs) in 469 patients with metastatic breast cancer receiving first-line chemotherapy who had serial samples available. The authors improved on the current model of baseline CTC measurement by identifying four CTC trajectory patterns. Progression-free and overall survival were most favorable in patients with undetectable CTCs. In the remaining patients, the model was able to stratify patients into low–, intermediate–, and high–CTC trajectory risk groups. The CTC trajectory performed better as a prognostic model than baseline CTC status or combined CTC status at baseline and end of cycle one.The findings from this large dataset with subsequent validation offer promising and generalizable results. CTC trajectory patterns may serve as a powerful prognostic biomarker to guide treatment decisions in women with metastatic breast cancer.
-
The secret of lymph: How lymph nodes help cancer cells spread
For decades, physicians have known that many kinds of cancer cells often spread first to lymph nodes before traveling to distant organs through the bloodstream. New research from Children's Medical Center Research Institute at UT Southwestern (CRI) provides insight into why this occurs, opening up new targets for treatments that could inhibit the spread of cancer.
The study, published today in Nature, found melanoma cells that pass through the lymph nodes pick up a protective coating, allowing them to survive high levels of oxidative stress in the blood [ferroptosis] and go on to form distant tumors...
They discovered cancer cells from the lymph had higher levels of a monounsaturated fatty acid known as oleic acid, which is the main component of olive oil. They also found this monounsaturated fatty acid was incorporated into the membranes of cancer cells in the lymph. This diluted polyunsaturated fatty acids in the membranes of these cells, inhibiting the chemical reactions that lead to ferroptosis and protecting the cells.
This protective coating of oleic acid from the lymph thus allowed the cancer cells to safely enter the blood, travel to other locations, and form metastatic tumors.
https://medicalxpress.com/news/2020-08-secret-lymph-nodes-cancer-cells.html
-
Published today in The Times newspaper, targeted radiotherapy at the same time as surgery can be just as effective as weeks of radiotherapy sessions.
https://www.thetimes.co.uk/article/new-treatment-heralds-breakthrough-for-breast-cancer-patients-c2js2kjjr?shareToken=ba9fca3c89bd9235fc8a5186708869d9 -
Dear Debbew, thanks for the article. The logical question that follows is whether it has something to do with intake of products that contain oleic acid (like olive oil, etc.)? Saulius
-
Saulius, that would be interesting to know. It's complicated by the fact that the body can make oleic acid and does so but preferentially shuttled it to the brain. We need it in other body systems as welll though...
https://www.sciencedirect.com/science/article/pii/...
"Therefore, the endogenous synthesis in many organs does not compensate for the absence of oleic acid from the food (Bourre et al., 1997b). This fatty acid is therefore partially essential.
There may be several explanations for why the oleic acid concentration in cerebral structures is not altered according to the oleic acid content of the diet. The nervous system may selectively bind oleic acid, perhaps by specific, active transport mechanisms across the blood brain barrier."
-
Thanks for this moth, wish there was a like button!
-
BSandra,
Adding on to moth's good info, I'll point to the article on olive oil from the food for breast cancer site, which recommends *only* extra virgin olive oil:
"Oleic acid might not account for olive oil's anti-cancer effects. In pure form, oleic acid has been shown to induce migration and proliferation of both hormone receptor positive (ER+/PR+) and triple negative breast cancer cells. These findings imply that the protective effect of olive oil may be due to other components of the oil and not the direct effect of oleic acid. The findings also argue against using highly refined olive oil."
The rest of the article talks about all the potential benefits of EVOO. BTW, I love that site and how they provide handy references to a bunch of relevant research on different foods and, to a lesser degree, supplements.
https://foodforbreastcancer.com/foods/olives-and-olive-oil
BTW, moth, I noticed this link in with their relevant olive oil research references:
Oleic Acid Reduces Brain Injury by Oxidative Stress Induced by Some Anticancer Drugs in Rat Brain
-
This August 2020 paper about the various mutations cancer can develop to resist Ibrance + anti-estrogen looks like it could help us to choose the next line of treatment/trial after Ibrance fail and genomic testing.
https://www.biorxiv.org/content/10.1101/857839v1.full
The genomic landscape of intrinsic and acquired resistance to cyclin-dependent kinase 4/6 inhibitors in patients with hormone receptor positive metastatic breast cancer
-
Long-term TARGIT-A data support single-dose intraoperative breast cancer radiotherapy
The 5-year results of the TARGIT-A trial have demonstrated the noninferiority of risk-adapted, single-dose targeted intraoperative radiotherapy (TARGIT-IORT) delivered during lumpectomy to conventional radiotherapy for the adjuvant treatment of early-stage breast cancer...
In fact, the risk for mortality from causes other than breast cancer was a significant 41% lower for women who received TARGIT-IORT than those given EBRT, a finding consistent with other reports, including a meta-analysis of randomized trials, say the study authors.
-
Dear Debbew, Moth, thanks for these insights. For sure it should be only "extra virgin" olive oil, as olive oil producing countries only use that one. But everything with moderation. "The middle way" - that is my philosophy... Saulius
-
I start to hate mice:) https://scienmag.com/new-therapy-targets-breast-cancer-metastases-in-brain/ Could not get to the article in Science Translational Medicine
Would write to investigators to check when do they plan a clinical trial? Saulius -
Dual HER2 Blockade Plus an AI in Postmenopausal Women With HER2+/HR+ Metastatic Breast Cancer
- Journal of Clinical Oncology August 26, 2020 The authors report updated results from a trial of dual HER2 blockade with trastuzumab plus lapatinib in combination with an aromatase inhibitor (AI) versus trastuzumab and AI in postmenopausal women with HER2+/HR+ metastatic breast cancer. The original publication of this trial was redacted due to statistical errors leading to small changes in the secondary analyses, but these do not impact the overall conclusions of this study, which showed a superior progression-free survival associated with dual HER2 blockade plus AI compared with trastuzumab plus AI.The combination of trastuzumab plus lapatinib plus AI offers an effective treatment alternative to chemotherapy for this population.
Commentary by Lee S. Schwartzberg MD, FACP:Dual HER2 blockade with chemotherapy has been shown to be of benefit in HER2-positive MBC, as noted in the CLEOPATRA trial for taxane, trastuzumab, and pertuzumab, and the recent HER2CLIMB trial for tucatinib, trastuzumab, and capecitabine. The ALTERNATIVE study evaluated a chemotherapy-free strategy in patients with HR-positive, HER2-positive MBC by utilizing a lapatinib, trastuzumab, and AI combination. They demonstrated improved PFS and a trend toward OS with very good tolerance. Of note, the large majority of these patients had received prior trastuzumab and chemotherapy. For patients with this biomarker profile, an endocrine/HER2–blockade approach makes sense and has the potential for improved quality of life over chemotherapy. It will be interesting to evaluate such a strategy with newer, more effective TKIs (such as neratinib or tucatinib) with trastuzumab and endocrine therapy in this setting.DOI: 10.1200/JCO.20.01894 Journal of Clinical Oncology{Abstract is free; fee for full article.} -
BET inhibition increases βIII-tubulin expression and sensitizes metastatic breast cancer in the brain to vinorelbine
Science Translational Medicine. August 26, 2020
BETting against brain metastases
Brain metastases are a dreaded complication of many cancer types. Even for malignancies that are relatively treatable, such as breast cancer, brain metastases are difficult to reach and often are not susceptible to the same therapies as peripheral tumors. By comparing primary and metastatic breast cancers, Kanojia et al. identified differences in the expression of cytoskeletal protein βIII-tubulin, which was increased in tumors that metastasized to the brain and sensitized them to vinorelbine, a chemotherapy drug. Another drug type, called a BET inhibitor, promoted βIII-tubulin expression and further sensitized breast cancer metastases to vinorelbine in mouse models, demonstrating a promising therapeutic combination.
Abstract
Metastases from primary breast cancer result in poor survival. βIII-tubulin (TUBB3) has been established as a therapeutic target for breast cancer metastases specifically to the brain. In this study, we conducted a systematic analysis to determine the regulation of TUBB3 expression in breast cancer metastases to the brain and strategically target these metastases using vinorelbine (VRB), a drug approved by the U.S. Food and Drug Administration (FDA). We found that human epidermal growth factor receptor 2 (HER2) signaling regulates TUBB3 expression in both trastuzumab-sensitive and trastuzumab-resistant neoplastic cells. We further discovered that bromodomain and extra-terminal domain (BET) inhibition increases TUBB3 expression, rendering neoplastic cells more susceptible to apoptosis by VRB. Orthotopic xenograft assays using two different breast cancer cell models revealed a reduction in tumor volume with BET inhibition and VRB treatment. In addition, in vivo studies using a model of multiple brain metastasis (BM) showed improved survival with the combination of radiation + BET inhibitor (iBET-762) + VRB (75% long-term survivors, P < 0.05). Using in silico analysis and BET inhibition, we found that the transcription factor myeloid zinc finger-1 (MZF-1) protein binds to the TUBB3 promoter. BET inhibition decreases MZF-1 expression and subsequently increases TUBB3 expression. Overexpression of MZF-1 decreases TUBB3 expression and reduces BM in vivo, whereas its knockdown increases TUBB3 expression in breast cancer cells. In summary, this study demonstrates a regulatory mechanism of TUBB3 and provides support for an application of BET inhibition to sensitize breast cancer metastases to VRB-mediated therapy.
https://scienmag.com/new-therapy-targets-breast-cancer-metastases-in-brain/
https://stm.sciencemag.org/content/12/558/eaax2879
DOI: 10.1126/scitranslmed.aax2879
{Abstract is free; fee or membership required to access full article.}
BSandra: this is the article you referenced. Thx for the tip!
-
Changes in Peripheral and Local Tumor Immunity After Neoadjuvant Chemotherapy Reshape Clinical Outcomes in Patients With Breast Cancer
- Clinical Cancer Research August 27, 2020 The authors completed a genetic evaluation of the tumor microenvironment in patients with residual disease following neoadjuvant chemotherapy to assess the effect of chemotherapy on the tumor microenvironment in correlation with disease outcomes. In ER+/PR+ breast cancer, there was no significant genetic change associated with relapse-free or overall survival. However, there was an increase in gene set expression in triple-negative breast cancer (TNBC), which was associated with improved outcomes. Additionally, increased cytotoxic T-cell signatures in the peripheral blood of TNBC patients suggested that neoadjuvant chemotherapy has potentially immunogenic effects in these patients.While additional studies are needed to clarify this relationship, these data are suggestive that cytotoxic gene signatures in peripheral blood may be an appropriate biomarker for persistent disease activity.
- {Abstract is free; log-in or purchase required to access full article.}
DOI: 10.1158/1078-0432.CCR-19-3685 -
FDA approves Foundation Medicine pan-tumor liquid biopsy test
The FDA approved FoundationOne Liquid CDx, a comprehensive pan-tumor liquid biopsy test.
FoundationOne Liquid CDx (Foundation Medicine) is a qualitative next-generation sequencing-based in vitro diagnostic test that analyzes 324 genes and genomic signatures to help guide treatment decisions for patients with solid tumors.
The FDA based the approval on results of clinical and analytical validation studies that included more than 7,500 samples and 30,000 unique variants representing more than 30 cancer types. Results showed high sensitivity and specificity, including at low allele frequencies, according to Foundation Medicine.
"Liquid biopsies are becoming an increasingly important option to inform personalized treatment decisions for physicians treating certain [patients with advanced cancer] who require minimally invasive solutions to genomic testing,"... "This approval helps expand access to important genomic information needed for physicians to make more informed decisions about targeted treatment approaches for their patients, and is another important step toward making comprehensive genomic testing a part of routine clinical cancer care."
Older and longer, more detailed article on similar topic here:
-
Study Finds Dairy (Not Soy) Skyrockets Breast Cancer Risk
Int J Epidemiol 2020 Feb 25
A new study claims that women who drink cows' milk could increase their risk of developing breast cancer by up to 80 percent compared to women who drink soy milk. Unbiased by either soy or dairy industry funding, this research was commissioned by the National Cancer Institute at the National Institutes of Health and the World Cancer Research Fund.
the researchers found a dramatic increase in risk with as little as a ¼-⅓ cup margin. Women who reported drinking just eight ounces a day increased their risk of breast cancer by 50 percent, and those who consumed two to three glasses of cows' milk escalated their risk by up to 80 percent (in comparison to the women who did not drink any cows' milk). To clarify, drinking one cup of cows' milk per day does not guarantee a woman is 50 percent more likely to get breast cancer. It does, however, suggest that her individual risk increases by 50 percent. So, if a person has an inherent 12 percent risk (the average), she can increase that risk by half simply by sipping one cows' milk latte or dairy-based smoothie a day. In contrast, participants who completely avoided cows' milk but consumed soy milk did not show an increased risk of cancer.
While this study does not prove cows' milk causes cancer, it opens up the field of study and provides a strong indicator of the harmful effects of dairy in comparison to benign foods. Researchers also suggested that the greatest benefits of soy milk in relation to breast cancer may not be in soy itself, but in the exclusion of dairy.
Conclusions: Higher intakes of dairy milk were associated with greater risk of breast cancer, when adjusted for soy intake. Current guidelines for dairy milk consumption could be viewed with some caution.
https://pubmed.ncbi.nlm.nih.gov/32095830/
doi: 10.1093/ije/dyaa007
{As the daughter of several generation of dairy farmers (with no history of breast cancer), it pains me to post this.... but there it is...}
-
Lumpie,
Thanks for posting the information on liquid biopsies. I really appreciate all the information you have been providing the group. It is so helpful. I’ll have to pester MO about this
-
My pleasure NorCalS. My MO has not wanted to use liquid biopsy either. I really hope she may change her mind if they become more standard practice. I have a resistant tumor. Biopsy showed it to be same old type as before, but I wonder if part of it has morphed. A liquid biopsy could be really helpful in such a sitaution.
-
Dear Lumpie, thanks... it is so strange that the very "historic" product like milk does this. Hundreds of generations grew up on milk, if not milk we probably would not be here, but on another hand when we are grown up, we rarely drink milk, only when we are little. Saulius
-
Saulius: You are right... there are lots of trade-offs and lots of questions remain unanswered. I believe that the studied population was adult only, so we don't know about childhood vs adult consumption and weather that makes a difference. As an adult, I really don't drink milk, but I put half-n-half in my coffee and I do enjoy cheese occasionally. I also like yogurt... but it can be digested differently because of the live and active cultures. Does this matter? More research to be done....
Edit: Big one: it does not indicate whether milk consumption impacts recurrence or prognosis for those with MBC.
-
I remember hearing of a dairy/breast cancer connection back in the 90s, but then science seemed to have reversed itself.
This does make me sad because I love cheese and I eat yogurt every morning. I did switch to oat milk or coconut creamer for coffee. Could switch to coconut milk yogurt a few times a week.
I currently buy sheep milk yogurt and cheese when I can, it is just easier to digest for me and very tasty 😋 Maybe it is a little better than cow milk? I joked that sheep are smaller than cows so maybe the fat makes us less fat than cow products 😆 ,
I will still avoid soy milk, I don’t like the taste anyway.Thank you Lumpie for continuing to gather all this great info for us x
-
Re liquid biopsies - as someone who just had one:
I recently had my blood pulled for the F1 liquid biopsy and my MO just sent me the report. This is about 14 months after my tissue biopsy. I haven't met with my MO about it yet (that's on Sept. 8) but I will say that just reading it over and trying to piece it all together, I am ambivalent on whether or not it is that helpful in comparison to a tissue biopsy. For me, the tissue biopsy had a bit more info. The blood biopsy did, however, identify another mutation that hadn't shown up in the tissue biopsy -- TP53. At first I freaked out when I saw that, but then did a little bit of research, and for NON-TNBC folks, it can indicate a sensitivity to immunotherapy (Yay!) which is good for me bc I also have a high tumor mutational burden.
Of interest to me was the fact that on my tissue biopsy, I had 2-3 ERBB2 mutations. On the blood one, it said "not detected." Very interesting. Waiting to find out if my doc thinks that's because of current I/F treatment.
-
Regarding milk - the integrative oncologist I worked with told me to cut out dairy or drastically reduce it. I still have milk here or there but way way less. If you have milk, the healthiest milk is organic grass-fed full fat but it still should be limited. He basically advocates a close to vegan diet with deep sea fish. Animal products mostly increase inflammation. Plus they displace vegetables and fruits, which have anti cancer phytonutrients.
-
BevJen: Thanks for sharing your experience with the liquid biopsy. It is my understanding that TP53 is a very common mutation. Please keep us posted on how it informs your treatment.
And thanks to others on dairy insights.
-
Lumpie, thank you for all your posts. I hope the liquid biopsy becomes more mainstream soon.
As for milk consumption and breast cancer risk, I hope this topic gets more investigation. As BSandra pointed out, milk has been a staple food source for many cultures for hundreds of years. However, modern milk production is not done in the same way it was done historically, and that could be a factor too.
I am not a huge consumer of dairy, but I do have a little bit almost every day. I use a small amount of milk in my coffee, and I find that plain yogurt is sometimes helpful for my stomach during chemo and Ibrance.
-
buttonsmachine: I had wondered about hormones, antibiotics... anything that might be added to the situation. Another forum I read raised the issue of BLV (Bovine leukemia virus) DNA. This was something I knew nothing about. If you want to read more on the topic, I will paste a citation below.
Bovine leukemia virus DNA associated with breast cancer in women from South Brazil
Nature - Published: 27 February 2019
Schwingel, D., Andreolla, A.P., Erpen, L.M.S. et al. Bovine leukemia virus DNA associated with breast cancer in women from South Brazil. Sci Rep 9, 2949 (2019). https://doi.org/10.1038/s41598-019-39834-7
-
Lumpie, thank you for your posts on dairy. Very disturbing. I consume dairy daily, milk, unflavored yogurt, cheese, and a wee bit of ice-cream. Maybe organic is not enough. Nutrition is so hard to pin down, advice changes all the time, lots of disagreement. Was it something else in their lifestyle ? At one time eggs were considered evil incarnate because of cholesteral, but now it seems like they have been redeemed as far as cholesterol is concerned.
-
Wow, the bovine leukemia connection just goes to show how far-reaching cause and effect can be - like the butterfly effect I suppose. That is definitely concerning.
I had another thought: is it possible that populations who traditionally consume more milk products are also at statistically higher risk for breast cancer anyway?
In statistics, we must always remember that "correlation is not causation" as they say.
I don't know the answers, but this is an interesting topic.
-
This specific study was talking about north American women.
& Actually, I believe we have not been consuming tons of cow milk for generations. Before refrigeration, milk spoiled quickly and thus our predecessors consumed dairy as fermented buttermilk, kefir or cheese. Even being able to consume milk & other dairy after weaning from human milk is geographically limited & linked to European genetic populations - most people become lactose intolerant around age 6 yr.
Also, all mammals produce milk to feed their babies so excess production didn't become common until humans started preferentially breeding animals for it.
The study mentioned here was done on north American women. I didn't see a race breakdown at first glance - will go have another look later.
Bias disclosure - ethical vegan; human lactation consultant -
Re the milk study, I take some comfort in this: "No important associations were noted with cheese and yogurt."
Consistent with moth's point about how we have evolved to consume dairy, and great news for Olma61.
-
Bovine leukemia virus DNA associated with breast cancer in women from South Brazil
Nature, Scientific Reports, Published: 27 February 2019
Abstract
Breast cancer is a neoplastic condition with a high morbidity and mortality amongst women worldwide. Recent data linking bovine leukemia virus (BLV) with breast cancer has been contested already. Our study investigated the presence of BLV genome in healthy (n = 72) and cancerous (n = 72) paraffin-embedded samples of breast tissues from women in south Brazil. BLV DNA was found most frequently (30.5%) in breast cancer tissue than in healthy breast (13.9%) (Odds ratio = 2.73; confidence interval = 1.18–6.29; p = 0.027). In contrast, antibodies to BLV were found in a very small percentage of healthy blood donors. There was no association between BLV DNA and other tumor prognostic biological markers such as hormonal receptors, HER2 oncoprotein, proliferation index, metastasis in sentinels lymph nodes, and tumor grade and size. Our findings suggest that BLV should be considered a potential predisposing factor to breast cancer in women.
Schwingel, D., Andreolla, A.P., Erpen, L.M.S. et al. Bovine leukemia virus DNA associated with breast cancer in women from South Brazil. Sci Rep 9, 2949 (2019). https://doi.org/10.1038/s41598-019-39834-7
{Posting this abstract for those disinclined or unable to click through. Full article is open access. I didn't find the reference to yogurt or cheese, but if those are not implicated, I am relieved!}
-
A Roadmap for Developing Study Endpoints in Real-World Settings
August 28, 2020
EXECUTIVE SUMMARY
With growing interest in using real-world data (RWD) and real-world evidence (RWE) to support regulatory decision-making, stakeholders are considering how to develop robust real-world study endpoints to evaluate medical product effectiveness when fit-for-use data and valid methods are available. Despite extensive literature and guidance for developing clinical trial endpoints, few resources support real-world endpoint development. Some principles can be carried over from the clinical trial setting, but differences in patient populations, care settings, and data collection in the real-world setting result in unique considerations for endpoint development. Additionally, studies conducted in the realworld setting have the potential to capture outcomes that are more relevant to patients than outcomes captured in clinical trials. This paper explores how key differences in study settings influence a researcher's considerations for developing study endpoints in the real world. First, because stakeholders involved in the realworld endpoint development process have multidisciplinary backgrounds, this paper details the current landscape of endpoint development, provides standardized definitions of key concepts, and introduces existing frameworks. Second, this paper presents a roadmap for endpoint development, beginning with selection of a concept of interest and study outcome that reflect the research question. Within this roadmap, the paper details how real-world settings impact selection of a concept of interest, outcome, and endpoint components, raising challenges for researchers to consider when developing real-world endpoints. Third, this paper addresses key considerations for the validation of real-world endpoints. Finally, this paper examines opportunities to enhance the use of real-world endpoints through stakeholder collaboration.
The paper contains disclosures about drug company funding of and participation in the preparation of the paper.
The full paper is available here without charge (but you may have to register): https://healthpolicy.duke.edu/sites/default/files/2020-08/Real-World%20Endpoints.pdf
-
Came across this article - it summarises MBC and some of the current clinical trials and may have already been posted here.
https://www.oncozine.com/new-therapies-may-offer-hope-for-patients-with-metastatic-breast-cancer/
-
Very early study with a long ways to go but, it's very interesting/cool none the less.
https://www.abc.net.au/news/2020-09-01/new-aus-research-finds-honey-bee-venom-kills-breast-cancer-cells/12618064
-
Morrison,
Thanks for the article. Very interesting indeed. Hopefully, they get it to the human clinical trials stage soon
-
Here's a wild one -- talking about the venom of the honey bee wiping out breast cancer cells. The ingredient that does is can be synthetically created, so perhaps some drug company will jump on this.
http://dx.doi.org/10.1038/s41698-020-00129-0
-
Dear Bev, just read the article - honeybees saving humans - I like this idea:)> Just like Pacific yew tree (taxanes), another organic chemotherapy! Saulius
-
Saulius,
Yes, to me, this honey bee stuff sounds very promising -- and also makes me wonder why the heck we haven't found a "cure" for cancer. My pessimistic self says it is because lots of things could "cure" cancer, or at least some types of cancer. But they are not commercially viable, meaning that some company can't make a lot of money in developing it. The good thing about the honey bee story is that the thing that they take from the honey bee can be synthetically created -- so -- maybe commercially viable?
I did have to laugh when I read the article, though. I am seriously allergic to certain bee venoms, and in fact, years ago, had to go through treatments to desensitize me to bee stings because it could be life threatening for me. However, honeybees were not among my list of bees and wasps to which I would react, so bring on the honeybees!
-
Aug 30, 2020
Clinical implications of HER2 mRNA expression and intrinsic subtype in refractory HER2-positive metastatic breast cancer treated with pan-HER inhibitor, poziotinib
Breast Cancer Research And Treatment
Abstract
We explored clinical implication of intrinsic molecular subtype in human epidermal growth factor receptor 2 (HER2) + metastatic breast cancer (BC) with pan-HER inhibitor from a phase II clinical trial of poziotinib in refractory HER2+BC patients. For this translational research correlated with phase II clinical trial, we performed an nCounter expression assay, using gene panel including 50 genes for PAM50 prediction and targeted deep sequencing. From 106 participants, we obtained 97 tumor tissues and analyzed gene expression in 91 of these samples. Of 91 HER2+BCs, 40 (44.0%) were HER2-enriched (E) intrinsic molecular subtype, 17 (18.7%) of Luminal A, 16 (17.6%) of Basal-like, 14 (15.4%) of Luminal B and 4 (4.4%) of Normal-like. HER2-E subtype was associated with hormone receptor negativity (odds ratio [OR] 2.93; p = 0.019), 3 + of HER2 immunohistochemistry(IHC) (OR 5.64; p = 0.001), high mRNA expression of HER2 (OR 14.43; p = 0.001) and copy number(CN) amplification of HER2 (OR 12.80; p = 0.005). In genetic alterations, alteration was more frequently observed in HER2-E subtype (OR 3.84; p = 0.022) but there was no association between PIK3CA alteration and HER2-E subtype (p = 0.655). In terms of drug efficacy, high mRNA expression of HER2 was the most powerful predictor of poziotinib response (median progression-free survival [PFS): 4.63 months [high] vs. 2.56 [low]; p < .001). In a combination prediction model, median PFS of intrinsic subtypes except Her2-E with high HER2 mRNA expression without PIK3CA genetic alteration was 6.83 months and that of the remaining group was 1.74 months (p < .001). HER2-E subtype was associated with hormone receptor status, HER2 IHC, CN and mRNA expression and TP53 mutation. In survival analysis, the information of level of HER2 mRNA expression, intrinsic molecular subtype and PI3K pathway alteration would be independent predictors to poziotinib treatment. ClinicalTrials.gov identifier: NCT02418689.
DOI: 10.1007/S10549-020-05891-0
-
Published in Oncology
September 01, 2020
Surgery at Primary and Metastatic Sites for Stage IV Breast Cancer
- The authors of this National Cancer Database study of 54,871 patients with stage IV breast cancer found longer overall survival to be associated with lumpectomy or mastectomy compared with no surgery. There was also a survival benefit associated with liver, lung, and brain metastasectomy.
- These findings add to previous retrospective studies suggesting improved survival with surgical management in the setting of metastatic breast cancer but are in contrast to various prospective studies which have failed to demonstrate a survival benefit with the addition of local management to systemic treatment, including the updated results from E2108 presented at ASCO 2020.
{Access to full article requires a fee or subscription.} -
Anyone hear of this drug that should perform better than fulvestrant?
Arvinas is developing ARV-471, an oral estrogen receptor (ER)-targeting PROTAC® protein degrader for the potential treatment of patients with locally advanced or metastatic ER positive / HER2 negative breast cancer.Trial NCT04072952
I am going to check it out when I go to Sarah Cannon next week
Dee -
Lumpie, in the article about surgery for stage iv, do they mean stage iv in the technical sense of de novo stage iv, or as many use the term to mean metastatic whether de novo or distant recurrence? (I have not subscribed so could not access the articles.)
-
Dee, I see that is a phase I study with ARV-471. On the Ibrance thread Cure-ious recently posted about the current status of oral SERD trials. Apparently there are only three that are beyond phase 1 right now.
-
ShetlandPony: Good question. The full article may go more explicitly into methodology. Reviewing the info available to us, it says they were only looking at women classified as stage 4 in the "National Cancer Database," by which I assume that they mean the SEER database in the US. (The authors are all associated with the Cleveland Clinic.) We all know that there are problems with classification in SEER. (Link below to the MBCN discussion of these issues.) Since the database only counts those diagnosed de novo's as stage 4, it would seem that they are only looking at the case histories of de novo diagnoses for this study. It would be interesting to parse more complex histories to try to identify patterns. Someday, someone will take on that project.
-
Thanks, Lumpie. That’s what I figured.
-
Harry Perkins Institute of Medical Research study finds honeybee venom rapidly kills aggressive breast cancer cells:
-
Dear Bev, I am not allergic to bees but I love nature, spend lot's of time by lakes and get stung once in a while, so... it hurts:) Cannot imagine being stung by 100 bees but if that'd be a cure for C, I'd take it:) Sure the are looking into commercializing this compound (melittin), and therefore it will take years to get it to the market if all stars align:/ Saulius
-
For HER2+/ERBB2- MBC adding Keytruda/pembrolizumab to eribulin doesn't improve PFS
"The results do not support the use of pembrolizumab in combination with eribulin for patients with hormone receptor–positive/ERBB2-negative metastatic breast cancer, independent of programmed cell death ligand 1 status."
https://jamanetwork.com/journals/jamaoncology/article-abstract/2769923?utm_source=twitter&utm_campaign=content-shareicons&utm_content=article_engagement&utm_medium=social&utm_term=090320#.X1E_Ap9GuxA.twitter
-
September 03, 2020
Blood test detects common cancer types 4 years before current screening methods
A novel blood-based assay demonstrated the ability to detect five cancer types up to 4 years earlier than current screening methods, according to study results published in Nature Communications.
The noninvasive PanSeer test (Singlera Genomics), which is based on DNA methylation, detected stomach, esophageal, colorectal, lung and liver cancer in 91% of asymptomatic individuals who were diagnosed with cancer 1 to 4 years later using standard detection methods.
"The ultimate goal would be performing blood tests like this routinely during annual health checkups,"..."But the immediate focus is to test people at higher risk, based on family history, age or other known risk factors."
...the current study, researchers analyzed plasma samples of 605 asymptomatic individuals, of whom 191 were diagnosed with stomach, esophageal, colorectal, lung or liver cancer up to 4 years after plasma collection.
With a specificity of 96% (95% CI, 93-98), the test detected cancer accurately in 88% (95% CI, 80-93) of post-diagnosis samples....it detected cancer in 95% (95% CI, 89-98) of asymptomatic individuals who were later diagnosed with cancer, although researchers noted that this result needs to be confirmed in larger studies.
we hope to proceed with a large prospective study of healthy individuals to determine if noninvasive cancer screening can reduce cancer deaths in a cost-effective manner."
{Not BC specific, but more encouraging news about blood-based assays.}
https://www.healio.com/news/hematology-oncology/20...
-
I Was Right — How one doctor learned the importance of advocacy
Podcast {audio} episode called Infectious and {section on patient advocacy} starts at 12:10 on the podcast. It's from Brita Lundberg, MD, patient advocate and founder of Lundberg Health Associates in Boston.
https://www.medpagetoday.com/podcasts/anamnesis/87...
{Really interesting commentary - by a physician - on the importance of patient advocacy (she was advocating for her mom). Not BC specific. Relevant segment is about 15 minutes long. No charge to access but you may need to subscribe/sign in.}
-
Oncologists Were Paid To Prescribe Generic Chemotherapy (Here's Why It Didn't Change A Thing)
Forbes.com Aug 27, 2020,07:00am EDT
Peter Ubel (@peterubel) writes in Forbes about the challenges of increasing use of generic drugs, which could save cancer patients' out-of-pocket costs, because of incentives in the payment system. Even when an insurer offered an additional payment to oncologists to offset the loss of revenue of prescribing a generic drug, compared to a name-brand drug, the program failed to increase generic prescribing.
For many medicines... oncologists receive a 6% markup, meaning when they infuse a patient with a $10,000 monthly course of chemotherapy, their practice yields an extra $600. By contrast, if the practice treated that patient with a generic chemotherapy, they'd be out most of that extra money.
"We shouldn't simultaneously burden patients with high out-of-pocket costs while incentivizing physicians to prescribe unnecessarily expensive medications."{Note on author perspective: In his book, Sick to Debt, Peter Ubel argues for a middle path between a market-based and a completely free system, Ubel envisions more transparent, smarter healthcare plans that tie the prices of treatments to the value they provide so that people can afford to receive the care they deserve.}
https://www.forbes.com/sites/peterubel/2020/08/27/...
{Obviously, this pertains to the U.S. only. I doubt other developed countries allow such perverse incentive schemes. But please let us know if yours does. In the meantime, I'd like more info on that "completely free" system.}
-
Our health care system is so screwed up 😡
-
morrigan_257: I concur! Sad.
-
ASCO 2020: Immune Profiling of Tumor Microenvironment Predicts Overall Survival in Breast Cancer Brain Metastases
The findings may help identify which patients could potentially benefit from immunotherapy
September 01, 2020
"Brain metastases represent one of the major unmet needs in metastatic breast cancer," lead author Gaia Griguolo, MD, of the University of Padova in Italy, told Elsevier's PracticeUpdate. "Brain involvement is frequent in breast cancer and usually carries a poor prognosis. Even if the central nervous system has been traditionally considered an immune-privileged sanctuary for cancers, recent data from patients with other solid tumors treated with immunotherapy have challenged this dogma by showing intracranial activity of immunotherapy agents."
Dr. Griguolo went on to explain that an "understanding of the biological processes, and more specifically immune interactions, sustaining breast cancer brain metastases is still limited, as only a small number of studies have tested the role of the immune system in brain metastasis, and the majority of them included patients with a variety of solid tumors, not just breast cancer. Our effort [was] to generate biological knowledge regarding the immune microenvironment of brain metastases, … in order to understand if these immunological interactions are or are not subtype-specific, and to identify potential biomarkers."
Of the 60 brain metastases samples included in the study, 18 (31.0%) were classified as triple-negative breast cancer, 19 (32.8%) were HR-positive/HER2-negative, and 21 (36.2%) were HER2-positive.
After a median follow-up of 42.6 months, 35 patients (58.3%) had died. Median OS was 33.4 months (95% confidence interval 22.2–not reached). Breast cancer subtype was the only clinical variable associated with OS. Median OS was 9.4 months for triple-negative breast cancer patients, 33.4 months for HR-positive/HER2-negative patients, and 53.0 months for HER2-positive patients (P = .01).
...we have identified two immune characteristics with relevant prognostic impact: CD4/CD8 and FOXP3/CD8 ratio in the stroma and density of granzyme B+CD8+ cells in the tumor area in triple-negative breast cancer. These observations support, from a biological point of view, the inclusion at least of triple-negative breast cancer patients with brain metastases in clinical trials evaluating immunotherapy agents," concluded Dr. Griguolo.
"Our next step will be to assess, using a specifically designed [multiplex immunofluorescence] panel, the expression of immune checkpoints in these same samples, in order to identify therapeutically actionable targets," she added.
https://www.practiceupdate.com/c/101957/67/13/?els...
{No charge to access but may require registration/sign in.}
-
HER2 Expression on Tumor-Derived Extracellular Vesicles and CTCs
Journal Scan / Research · August 25, 2020
- This study retrospectively reanalyzed stored peripheral blood samples from 114 patients with metastatic HER2-positive breast cancer for the presence of HER2 expression in circulating tumor cells (CTCs) and tumor-derived extracellular vesicles (tdEVs). The inclusion of anti-HER2 targets increased the detection of one CTC in a given sample from 89% to 95%. Interestingly, HER2 was detected in CTCs and tdEVs that express cytokeratin, which is often used to enhance CTC detection. Additionally, a preselected ROC target of 7% HER2+ CK+ tdEVs predicted HER2 expression with 74% sensitivity and specificity when compared with the HER2 amplification status of the primary tumor sample.
- CTC and tdEV heterogeneity in the blood of patients is inversely associated with overall survival.
- These results should be validated with prospective, large-scale analysis of patient samples. However, they present an encouraging prospect for screening for the presence of HER2 based on liquid biopsy.
{Open access} -
PBS NewsHour: The Best Health Care? America & the World
The presidential election will determine the course of the U.S. health care system — the most expensive system in the world, brimming with innovation but one that also leaves more than 30 million uninsured. This special series explores how the U.S. health care system stacks up with the rest of the world.
https://www.pbs.org/newshour/series/the-best-healt...
{Video. Free access. 5 segments, each of about 8 to 10 minutes duration.}
Try this 8 question, related quiz: WHAT DOES HEALTH CARE COST AROUND THE WORLD?
https://www.pbs.org/newshour/features/health-cost-...
{It's insightful.}
-
Veliparib With Carboplatin and Paclitaxel in BRCA-Mutated Advanced Breast Cancer
- The Lancet Oncology September 03, 2020 This large phase III trial demonstrated that the addition of veliparib (vs placebo) to carboplatin and paclitaxel in more than 500 patients with HER2-negative, germline BRCA mutation–associated breast cancer was well-tolerated and led to improved progression-free survival.Overall survival was similar in the interim analysis, but further follow-up will be needed.
- https://www.practiceupdate.com/C/105768/56?elsca1=...
- https://www.thelancet.com/journals/lanonc/article/...(20)30447-2/fulltext
- DOI:https://doi.org/10.1016/S1470-2045(20)30447-2
- {Press summary which includes MO commentary, free. Registration/log-in may be required; article abstract available free. Full access requires, purchase or subscription.}
-
Efficacy of Eribulin for Metastatic Breast Cancer Based on Localization of Specific Secondary Metastases
- Published in Metastatic Breast Cancer September 01, 2020In this post hoc analysis of 1864 pretreated patients with locally advanced/metastatic breast cancer who were treated with eribulin, the authors determined that eribulin was effective independent of metastatic location at baseline. Among patients with bone, lymph node, and chest wall/breast/skin metastases at baseline, there was a small but significant overall survival benefit for patients who received eribulin versus control treatment. Improved overall survival was also observed in patients with liver metastases who received eribulin.These findings suggest that eribulin has benefits for patients with locally advanced or metastatic breast cancer with metastases to bone, liver, lung, lymph node, and chest wall/breast/skin.
{Open access} -
Emerging Treatment Strategies for Breast Cancer Brain Metastasis
Published in Metastatic Breast Cancer - August 31, 2020
In this review, the authors discuss currently available clinical treatment options and emerging strategies for patients with breast cancer brain metastases.
Abstract
Systemic therapies for primary breast cancer have made great progress over the past two decades. However, oncologists confront an insidious and particularly difficult problem: in those patients with metastatic breast cancer, up to 50% of human epidermal growth factor 2 (HER2)-positive and 25–40% of triple-negative subtypes, brain metastases (BM) kill most of them. Fortunately, standard- of-care treatments for BM have improved rapidly, with a decline in whole brain radiation therapy and use of fractionated stereotactic radiosurgery as well as targeted therapies and immunotherapies. Meanwhile, advances in fundamental understanding of the basic biological processes of breast cancer BM (BCBM) have led to many novel experimental therapeutic strategies. In this review, we describe the most recent clinical treatment options and emerging experimental therapeutic strategies that have the potential to combat BCBM.
Commentary by Lillie D Shockney RN, BS, MAS, ONN-CG re merits of proactive screening.
https://www.practiceupdate.com/c/104222/67/13/?els...
https://journals.sagepub.com/doi/10.1177/175883592...
https://doi.org/10.1177/1758835920936151
{Open access}
-
Targeting HER2 in Breast Cancer Patients With Brain Metastases
- Video Interview with Lee S. Schwartzberg MD, FACP
- Run time 5:12
- Discusses systemic therapy, radiation therapy, and surgical options. Referrencs hippocampal sparing.
- https://www.practiceupdate.com/c/102115/67/13/?els...
-
Great news about Eribulin Lumpie. Thanks for posting that. It is in my bucket.
the hard part is reading the median OS numbers.difference in OS was also seen in patients with liver metastases randomized to eribulin versus control (median: 13.4 versus 11.3 months,
😢 2 extra months in overall survival is statistically good but only a median of 13.4 months prolonged OS I guess I should be happy that I am at 17 months and counting and still haven’t achieved PFS
Dee
-
While it might not apply to the ER+, HER-, it is comforting that it can beeeee synthetically produced and that stinging not necessary. There was a study about rattlesnake venom a while back, have not heard anything about it recently. Hopefully biting won't be required.
-
AlabamaDee : I hear ya! Sometimes it's two steps forward, one step back. Ya think... 2 months? That's all? But 2 months beats 0 months, as long as the QOL is pretty good. Hoping we get some better traction. I don't seem to be having much luck getting to progression free either. Hoping for improvement asap on that front! Hang in htere.
-
New Therapy Targets Breast Cancer Metastases In Brain
On Aug 26, 2020
Combination therapy reduces tumor size, dramatically improves survival in mice
CHICAGO — When breast cancer spreads to the brain, the prognosis is grim. Patients only have about six months to live.
Women with HER2-positive breast cancer tend to develop brain metastases in up to 55% of cases. Chemotherapy drugs targeting breast cancer cells in the brain aren't effective, because they can't cross the blood-brain-barrier.
But a new combination therapy targeting breast cancer tumors in the brain dramatically decreased tumor size and increased survival in a study with mice, reports a new Northwestern Medicine study. An estimated 75% of mice that had brain metastases from breast cancer were cured and cancer-free after the therapy.
"The new combination therapy we identified can cross the blood-brain barrier," said lead study author Dr. Maciej Lesniak, Northwestern Medicine chair of neurological surgery and professor of neurosurgery at Northwestern University Feinberg School of Medicine. "The therapy also targets brain metastases and significantly improves survival."
The paper will be published on August 26 in Science Translational Medicine.
The two drugs are tubulin inhibitor, vinorelbine, approved by the U.S. Food and Drug Administration (FDA) and available in clinics, and bromodomain inhibitor, I-BET-762, FDA approved for clinical trials. The bromodomain inhibitor increased βIII-tubulin, a protein found in cancer cells that metastasize to the brain. Overexpression of βIII-tubulin sensitized cancer cells to be killed by vinorelbine.
"The findings of our work set the stage for a clinical trial, whereby patients with breast cancer brain metastases can be treated with the combination of these two drugs," Lesniak said. "This will offer patients with breast cancer brain metastases, who have been systematically excluded from clinical trials, the chance to benefit from a new therapeutic regimen that has been proven to be strongly effective in experimental settings."
Breast cancer spreads to other organs like brain, lung and bone. The metastasis of breast cancer to the brain is a terminal disease and the deadliest complication.
There is a lack of targeted therapies for breast cancer brain metastases, said first study author Deepak Kanojia, research associate in neurological surgery at Feinberg.
"Patients with brain metastases are often excluded from clinical trials due to their poor outcomes and dismal survival," Kanojia said. "Regular systemic therapies, like Herceptin, do not cross the blood-brain-barrier efficiently, and offer no benefit in brain metastases," he said.
How the study worked
Scientists developed a mouse model that can grow multiple brain metastases to simulate what happens in human patients. They injected tumor cells in the intracarotid artery, resulting in the formation of multiple brain tumors. After the tumors grew, scientists treated the mice with the combination therapy. Final results revealed that 75% of the mice that were treated with the combination were cured and cancer-free.
https://scienmag.com/new-therapy-targets-breast-ca...
https://stm.sciencemag.org/content/12/558/eaax2879
DOI: 10.1126/scitranslmed.aax2879
{Open access}
-
BlueGirlRedState: I, too, am anti-bite! A few years ago, there were studies about injecting chemo directly into tumors using transcutaneous needle/catheter (much like a biopsy). I gather they were not successful, although I do not know the details. If the bee venom moves toward clinical trials, I will be interested in knowing how they propose to administer it.
-
Lumpie, thanks so much for all your work here. I see my MO Tuesday to discuss possibly moving to the Tucatinib, Xeloda, Herceptin combo or maybe a trial for brain mets I love having some knowledge about these things before the follow ups, you all never fail to spread the word and keep up up to date.
-
Thanks for your kind words, illimae - and good luck at your follow-up.
My MO + 2nd opinion both pushed Enhertu vs the Tucatinib, Xeloda, Herceptin combo. I think the sequencing is still subject to some debate. I couldn't find any good trials that met my needs this go-round, but I am encouraged that there seems to be some brain mets research going on.
-
I wish you the best luck with whatever you decide next and I’ll post any new details about the treatment changes or trial on the brain mets thread after my meeting. Enjoy your weekend 🙂
-
Dr. Pegram on the DESTINY-Breast01 Trial With Trastuzumab Deruxtecan in HER2+ Breast Cancer
OncLive - August 27, 2020@{Watch the video at link below. Runtime @ 2:25. Transcript:}
Mark D. Pegram, MD, co-director of Stanford's Molecular Therapeutics Program, and director of the Breast Cancer Oncology Program, at Stanford Women's Cancer Center, discusses the results of the phase 2 DESTINY-Breast01 study examining fam-trastuzumab deruxtecan-nxki (Enhertu; DS-8201) in patients with HER2-positive breast cancer.
Trastuzumab deruxtecan is a HER2 antibody-drug conjugate (ADC) that is based on a backbone sequence of trastuzumab (Herceptin), which is covalently linked to a topoisomerase 1 inhibitor payload exatecan derivative by a tetrapeptide-based cleavable linker, says Pegram. This agent is unique, with many attributions that distinguish it from ado-trastuzumab emtansine (T-DM1; Kadcyla). For example, T-DM1 has about 3.5 molecules per payload per antibody backbone, whereas trastuzumab deruxtecan has a drug-to-antibody ratio of 8, adds Pegram.
The DESTINY-Breast01 study was a 2-part, open-label, single-group, multicenter, phase 2 study. In the first part of the study, 3 doses of trastuzumab deruxtecan were evaluated in order to identify a recommended phase 2 dose, which was determined to be 5.4 mg/kg given intravenously every 3 weeks. In the second part of the study, the efficacy and safety of the recommended dose was documented, says Pegram. Overall, 184 patients were enrolled and they had undergone a median of 6 previous treatments prior to study enrollment.
The overall response rate (ORR) in this heavily pretreated population was 60.9%; this is the highest ORR reported for a single-agent HER2-targeted therapy in such heavily pretreated patients, according to Pegram. The disease control rate was 97.3% at the time of data presentation, adds Pegram. The durability of response with the ADC was also impressive, according to Pegram, with a median progression-free survival (PFS) of 16.4 months.
Moreover, a subset analysis of the trial looked at 24 patients with central nervous system metastasis and showed that the ORR in that subset was approximately 58% with a median PFS of 18.1 months, which is very similar to what had been observed in the intention-to-treat populations. Once the ADC received regulatory approval from the FDA, it became a new practice standard, concludes Pegram.
https://www.onclive.com/view/dr-pegram-on-the-dest...
-
Lumpie, picked up your post re brain mets and immediately thought Mae would be keen to see this.....scroll down and there she is! Just know that there’s a whole wee community here who really appreciate you!
-
"There was a study about rattlesnake venom a while back, have not heard anything about it recently. Hopefully biting won't be required"
I'm equally terrified and fascinated by Snakes so I've been following this and, no updates.
However, if it takes a bite, I'll sign up 😁
Reality though it won't take a bite, I don't know if it can be synthesized so I wonder (if it actually works) if there's going to be snake milking farms in the future 😃
I do love the fact that people are looking at animals (bees, snakes), our immune system, and recycling other drugs as Cancer treatment. There are so many drugs that have beneficial effects they're not designed for.
-
Hi.
I posted my question regarding the following Clinical trial on a vaccine for TNBC, in the TNBC forum, but was also hoping for any input on vaccine clinical trials for any type of BC.
https://clinicaltrials.gov/ct2/show/NCT03012100
I am interested to know about side effects, efficacy, etc. Any input would be appreciated -
Karenfizedbo15: Thank you! Made my day!
-
New Era for Targeting HER2 Beckons in Breast Cancer and Beyond
OncLive - September 3, 2020
Precision medicine advancements are opening a new chapter in the development of anticancer therapies that target the HER2 pathway, resulting in 3 approvals for breast cancer in less than a year and raising hopes for attacking other cancer types.
In the breast cancer arena, the FDA approved 2 new drugs, fam-trastuzumab deruxtecan-nxki (Enhertu) and tucatinib (Tukysa), and an expanded indication for neratinib (Nerlynx).1-3 Margetuximab, a novel monoclonal antibody (mAb), is hot on their heels, with developer MacroGenics seeking approval following promising phase 3 outcomes.4-6
Efforts to expand HER2-targeted therapy into other HER2-positive cancer types have met with less success over the years. Except for trastuzumab (Herceptin) in gastric cancer,7 there are no approvals outside of breast cancer, and multiple clinical trial failures have underscored that all HER2positive cancers are not created equal.8
Now, however, ongoing clinical trials of novel HER2-targeted therapies in gastric, colorectal (CRC), and non–small cell lung cancers (NSCLCs) are showing promise.9-12
Meanwhile, investigators are exploring the role of HER3, which preferentially partners with HER2 to drive oncogenic signaling in propelling resistance to HER2-targeted therapy.13-15 To date, HER3-targeted mAbs have demonstrated limited clinical efficacy, but the development of a HER2-HER3 bispecific antibody is generating early enthusiasm.16,17
Overall, a variety of approved and novel therapies are in the pipeline for targeting HER2 in a range of tumor types (see Table).
https://www.onclive.com/view/new-era-for-targeting...
{This lengthy article covers a number of interesting topics from new HER2 therapies to targeting HER3 and use of anti-HER2 therapies in the tx of other cancers. THanks for my friend Jackie for the link. Free access.}
-
In today's Washington Post (cross posted with are you on a clinical trial):
In a small bottom of the page article in today's Washington Post, it said that AbbVie has struck a deal on a cancer drug with a Chinese drug developer, I-Mab. Abbvie is getting the exclusive global license to develop and sell the Chinese company's cancer-fighting drug known as lemzoparlimab, also known as TJC4, which is an antibody used to treat multiple forms of cancer. According to the article, the drug therapy targets a "do not eat me" signal that allows cancer cells to avoid being targeted by a patient's immune system, blocking the signal to allow the immune system to "engulf and eradicate the malignant cells." Apparently, the Chinese company also has two other antibodies based upon the same drug, and AbbVie will develop those as well.
-
Oh interesting BevJen. I was just reading somewhere a brief mention about research on phagocytes being recruited. Sounds like someone has a working phagocyte stimulant with the lemzoparlimab. Phagocytes are some of my favourite cells from when I studied cell biology
I just want these drugs avail quickly on the market!
-
NorCalS : Many of us hold out hope for vaccines, both as prevention and to stimulate immune response in advanced cancers.
Well, I just wrote a long and detailed response that the page ate. Moral of this story: save your work. I will do what I can to recreate:
Official trial page: NCT03012100
Multi-epitope Folate Receptor Alpha Peptide Vaccine, GM-CSF, and Cyclophosphamide in Treating Patients With Triple Negative Breast Cancer
https://clinicaltrials.gov/ct2/show/NCT03012100
This trial is still recruiting, and I cannot find that it has reported any results yet.
Completion date: July 31, 2021
Required reporting date : July 31, 2022, midnight
Here are a couple of pages that give status reports on the trial. You should also be able to get this on the trial page but sometimes these have a friendlier format:
http://fdaaa.trialstracker.net/trial/NCT03012100/
If you are interested in breast cancer vaccines, I located this table of bc vaccine trials:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6340364/table/t3-bctt-11-053/
Published online 2019 Jan 17. doi: 10.2147/BCTT.S175360
If you are interested in reading about the rationale for breast cancer vaccines, this may be of interest:
Rationale for immunological approaches to breast cancer therapy
https://www.thebreastonline.com/article/S0960-9776(17)30477-0/pdf
DOI:https://doi.org/10.1016/j.breast.2017.06.009
This article references the trial and discusses the rationale for the research:
Folate receptor alpha expression associates with improved disease-free survival in triple negative breast cancer patients
https://www.nature.com/articles/s41523-020-0147-1#citeas
https://doi.org/10.1038/s41523-020-0147-1
Similar here:
Trial Watch: Immunostimulation with recombinant cytokines for cancer therapy
https://www.tandfonline.com/doi/full/10.1080/2162402X.2018.1433982
https://doi.org/10.1080/2162402X.2018.1433982
And here:
Design of an Epitope-Based Vaccine Ensemble for Animal Trypanosomiasis by Computational Methods
https://www.mdpi.com/2076-393X/8/1/130/review_report
https://doi.org/10.3390/vaccines8010130
Here is coverage of the trial in the popular press:
https://www.fox5atlanta.com/news/vaccine-could-prevent-breast-ovarian-lung-cancer
I believe that all references cited allow free access. This should be enough to keep any of us reading for a while! Bon chance!
-
Here is a link to the WaPo article BevJen referenced above:
AbbVie strikes deal on Chinese cancer treatment drug that may be worth $2.9 billion
https://www.washingtonpost.com/business/economy/ab...
The article calls the drug lemzoparlimab and TJC4 but neither of those comes up when I search the clinical trials.gov database.
Here is the Abbvie press release on the deal:
https://news.abbvie.com/news/press-releases/abbvie...
Also, the OncLive article posted above,
New Era for Targeting HER2 Beckons in Breast Cancer and Beyond
OncLive - September 3, 2020
discusses a drug "conditionally approved in China" but it seems to be a different drug, Pyrotinib. Here is the trial cited: "Results of a planned interim analysis of the phase 3 PHOEBE trial (NCT03080805) in patients with previously treated HER2positive MBC were presented at 2020 ASCO." Two other trials are referenced: Poziotinib (16 mg/day orally) produced an ORR of 42% in the first 12 evaluable patients in its trial (NCT03066206). For pyrotinib (400 mg daily), the ORR was 31.7% among 60 patients (NCT02834936). Both drugs had an acceptable safety profile."
Well, there are lots of companies excited to sell us thier drugs. I hope some of them work.
-
Lumpie,
Thanks again for the information. I will review and ask MO to help me get into a vaccine clinical trial
-
Thought I would share
https://clinicaltrials.gov/ct2/show/NCT04288089?term=04288089&draw=2&rank=1#contactlocationH3B-6545 represents a new class of ERα antagonists discovered by H3 Biomedicine scientists called "Selective Estrogen Receptor Covalent Antagonists" (SERCAs). SERCAs inactivate the estrogen receptor by targeting a cysteine that is not present in the majority of other nuclear hormone receptors. SERCAs have a unique biological activity profile compared to Selective Estrogen Receptor Modulators (SERMs) and Selective Estrogen Receptor Degraders (SERDs).https://www.h3biomedicine.com/2017/09/05/h3-biomedicine-announces-first-patient-dosed-with-h3b-6545-in-phase-1-study-in-breast-cancer/
This article says stable and partial response-https://ascopubs.org/doi/abs/10.1200/JCO.2019.37.15_suppl.1059
Dee -
found another one
OP-1250 is a small molecule Complete Estrogen Receptor ANtagonist (CERAN). OP-1250 potently competes with the endogenous activating estrogenic ligand 17-beta estradiol for binding in the ligand binding pocket. OP-1250 blocks estrogen-driven transcriptional activity, inhibits estrogen-driven breast cancer cell growth, and induces degradation of the estrogen
dee -
Dear All, Daiichi Sankyo is about to end another ADC's (Patritumab Deruxtecan, U3-1402) Ph2 clinical trial. It is an interesting ADC that targets HER3 and has to be as effective as DS-8201. Let's keep an eye on that one. Actually I found an interesting link where if you scroll down a bit, you can find a database of all developed ADCs and by using filter "Breast Cancer", you can get all of them related to BC. Just go through them, there are many links to clinical trials in everyone of them: https://www.adcreview.com/drugmap/u3-1402-patritum...
Saulius
-
Targeting Breast Cancer Cells and Leaving Healthy Cells Unscathed
...Now scientists at Johns Hopkins Medicine and the University of Oxford say they have found a new way to kill multiplying human breast cancer cells by selectively attacking the core of their cell division machinery. The method, only tested on lab-grown and patient-derived cancer cells, could advance efforts to find drugs that kill breast cancer cells in a subset of patients...
The research team looked for cell division mechanisms specific to cancer cells in a variety of lab-grown cells. During their search, they encountered a line of human breast cancer cells that are very dependent on cell structures called centrioles to divide and survive....
Further observations revealed that the centriole-dependent breast cancer cells had a section of genome that had been abnormally copied many times, an alteration found in about 9% of breast cancers. The researchers observed the genes encoded in the highly copied region and found a gene that was producing high levels of a protein called TRIM37 shown to control centrosomes...
They used a PLK4 inhibitor known to disrupt proteins that make centrioles, which interfered with TRIM37. When they added the drug to the lab-grown cancer cells with normal TRIM37 levels, they found that the cells were able to divide, even though the drug had removed the cell's centrioles. When the drug was added to breast cancer cells with high TRIM37 levels the cells were not able to divide and most cells stopped growing or died.
"The idea would be to identify tumors with high levels of TRIM37 and use a PLK4 inhibitor to selectively kill cancer cells and leave healthy cells relatively unharmed," explained Holland.
https://www.genengnews.com/news/targeting-breast-c...
paper: https://www.nature.com/articles/s41586-020-2690-1....
-
Combining nanotechnology and immunotherapy to fight MBC.
https://medicalxpress.com/news/2020-09-breast-cancer-nanotech-immunotherapy.html
“Efstathios "Stathis" Karathanasis, an associate professor of biomedical engineering, is directing the novel technique—sending nanoparticles into the body to wake up "cold" tumors so they can be located and neutralized by immune cells. The team also includes researchers from Cleveland Clinic and Duke University.““The NCI recently awarded a five-year, $3 million grant to Karathanasis and his team to continue their research, initially on animal models with an eye toward human trials. Much of the groundwork behind the project is described in a paper published in Cancer Research, the official journal of the American Association for Cancer Research.
-
Olma,
Really interesting idea. As with a lot of these great ideas, though, it's not ready for prime time (although a lot of us are!)
-
Olma61 - interesting idea, waking up cold tumors so that immunotherapy can neutralize them. Kind of scary too, given how hard it is to really treat cancer effectively.
-
Exercise and bone loss. Interesting article on exercise/bone loss in premenopause vs menopause. I wonder if post menopause needs to do more or different exercise to achieve same benefit. Also, which drugs were patients using? I still plan on exercising!! Trying to figure out how to get full article. https://www.practiceupdate.com/journalscan/73090/2/1?elsca1=emc_enews_daily-digest&elsca2=email&elsca3=practiceupdate_onc&elsca4=oncology&elsca5=newsletter&rid=NDg2NTE3NjI4ODEyS0&lid=10332481
-
Stereotactic Radiosurgery in Combination With Anti-HER2 Therapy for HER2+ Breast Cancer Brain Metastases
September 14, 2020
Interview with Rupesh R. Kotecha MD8:20 run time. Transcript is also available. {Particularly interesting mention of radiosurgery and concurrent HER2-directed therapy.} https://www.practiceupdate.com/c/102793/67/13/?els...
-
A Novel Staging System for De Novo Metastatic Breast Cancer Refines Prognostic Estimates
Published in Metastatic Breast Cancer - September 17, 2020 (also cited as July 09, 2020)
- In this study of 16,187 patients with de novo metastatic breast cancer selected from the National Cancer Database (2010–2013), the authors sought to identify prognostic groups using anatomic and biologic factors. Of these patients, 65.2% had a single metastatic site and 42.9% had bone-only metastases. The number of metastatic sites (1 vs >1) and ER status were used as stratification points, along with HER2 and PR status, cT stage, tumor grade, and presence of bone-only metastases. Significant differences in 3-year overall survival were observed among the three groups (stage IVB vs IVA and stage IVC vs IVA).
- These results support the stratification of patients with de novo metastatic breast cancer into three prognostic groups.
https://www.practiceupdate.com/c/104220/67/13/?els...
https://journals.lww.com/annalsofsurgery/Abstract/...
doi: 10.1097/SLA.0000000000004231
-
Aaa, dear Lumpie, it would be interesting to get whole article... Not very clear who falls into stage A, B or C:/ Saulius
-
I agree Saulius, Sounds so interesting I am tempted to buy access.
-
Oh, I would be so broke if I had to do pay for papers!
Sci-Hub is the link to get access to PubMed behind the paywall; there are many copies of this site out there
https://www.sciencemag.org/news/2016/04/whos-downl...
You find and copy the doi number of the paper and paste it into the site, it will be retrieved
Having said that, I tried it just now and the system hung on me.. not sure if its the site or the journal, Annals of Surgery is going to be a pretty rare request In general the site works like a charm, this is the first time I had trouble
-
thanks for this tip, Cure-ious
-
Aaa, thanks Cureious, site hangs for me too:/ I am using Firefox... will try other browsers later:) Saulius
-
Verzenio [reduces risk of] Recurrence and Metastasis of Early Breast Cancer
For people with high-risk HR-positive/HER2-negative early breast cancer, the oral medication Verzenio (abemaciclib) reduced the likelihood of recurrence by 25% when combined with adjuvant (post-surgery) hormone therapy, researchers reported at the European Society for Medical Oncology's ESMO Virtual Congress 2020 and in the Journal of Clinical Oncology.
If approved for this indication, Verzenio has the potential to set a new standard of care, according to lead study investigator Stephen Johnston, MD, PhD, a professor of breast cancer medicine at the Royal Marsden NHS Foundation Trust in London. It is "potentially one of the most notable treatment advances in the last two decades for this population of breast cancer patients," he said in a press release...
Between July 2017 and August 2019, Johnston and colleagues recruited 5,637 people with high-risk HR-positive/HR-negative early breast cancer from 38 countries for a Phase III study known as MonarchE...
At the two-year mark, 7.8% of the participants taking Verzenio had experienced a recurrence compared with 11.3% of the participants not taking Verzenio—a 25% reduction in risk.
Verzenio plus hormone therapy also improved distant relapse-free survival, a measure of the time to metastasis to another part of the body. At the two-year mark, 6.4% of the participants taking Verzenio and 9.7% of the participants not taking the drug had experienced metastasis—a 28% risk reduction...
Even though the study has not yet been completed—final results are projected for delivery in June 2027—Giuseppe Curigliano, MD, PhD, the chair of ESMO's guidelines committee, is optimistic. "This is a very important trial, and the findings will change practice," he said in an ESMO press release.
https://www.cancerhealth.com/article/verzenio-prev...
-
Gut Microbiota May Influence pCR in Early-Stage Breast Cancer
A study out of Scotland, to be presented at this year's virtual European Breast Cancer Conference in October, has linked levels of 2 short-chain fatty acids (SCFAs) in female patients with early-stage breast cancer to pathological complete response (pCR) to neoadjuvant chemotherapy (NACT), according to the abstract released today.
The 2 SCFAs are propionate and butyrate, and they were shown to be lower in the gut bacteria of patients achieving pCR compared with those not achieving pCR after surgery.
"In this study we have started to look at whether the function of the gut microbiome could be one factor that influences the effectiveness of chemotherapy," said Kirsty Ross, MBChB, MSc, a specialist registrar in medical oncology at the Beatson West of Scotland Cancer Centre, Glasgow, United Kingdom.
-
Palbociclib and Trastuzumab in {HR+}, HER2-Positive Advanced Breast Cancer
September 27, 2020 Clinical Cancer Research
- The phase II PATRICIA study was designed to evaluate the safety and efficacy of palbociclib plus trastuzumab in postmenopausal women with HR+/HER2+ advanced breast cancer. The median progression-free survival was 10.6 months in patients with luminal B tumors, 8.2 months in patients with luminal A tumors, 4.3 months in those with HER2-enriched breast cancers, and 3.7 months in women with normal-like tumors.
- The combination of palbociclib and trastuzumab is safe and relatively effective in patients with HR+/HER2+ advanced breast cancer who have progressed on prior treatment. Additional studies are enrolling to test the combination of palbociclib, trastuzumab, and endocrine therapy for superiority over treatment of choice.
DOI: 10.1158/1078-0432.CCR-20-0844 -
Trastuzumab With or Without Chemotherapy for HER2-Positive Early Breast Cancer in Older Patients
September 24, 2020 Journal of Clinical Oncology
- Patients aged >70 years were randomized to receive trastuzumab monotherapy or trastuzumab plus chemotherapy following surgical management of HER2-positive early breast cancer. Although the 3-year disease-free survival noninferiority primary endpoint for trastuzumab monotherapy was not met, the shorter survival was less than half a month at 3 years. In addition, there was significantly less deterioration in health-related quality of life in the trastuzumab monotherapy group compared with the trastuzumab plus chemotherapy group.
- Trastuzumab plus chemotherapy should remain the standard of care; however, these results warrant reflection for older patients with contraindications or preference to avoid chemotherapy. Trastuzumab monotherapy may be reasonable for appropriately selected patients.
DOI: 10.1200/JCO.20.00184 -
Experimental Cancer Treatment Destroys Cancer Cells [in mice] Without Using Any Drugs
One of the latest methods pioneered by scientists to treat cancer uses a Trojan horse sneak attack to prompt cancer cells to self-destruct – all without using any drugs.
Key to the technique is the use of a nanoparticle coated in a specific amino acid called L-phenylalanine, one of several such acids that cancer cells rely on to grow. L-phenylalanine isn't made by the body, but absorbed from meat and dairy products.
In tests on mice, the nanoparticle – called Nano-pPAAM or Nanoscopic phenylalanine Porous Amino Acid Mimic – killed cancer cells specifically and effectively, posing as a friendly amino acid before causing the cells to destroy themselves.
The self-destruction mode is triggered as the nanoparticle puts production of certain chemicals known as reactive oxygen species (ROS) into overdrive. It's enough to bring down the cancer cells while leaving neighbouring, healthy cells intact...
Nano-pPAAM was shown to kill around 80 percent of breast, skin, and gastric cancer cells in mice, about on a par with current chemotherapy drugs (but without all the side effects of course). While dangerous to cancer cells, it's based on a silica nanoparticle classed as safe to humans by US food regulators.
https://www.sciencealert.com/a-new-cancer-treatmen...
-
oh, that's interesting
-
Predictive Analytics Detects Breast Cancer Spread with 90% Accuracy
September 28, 2020 - A predictive analytics method was able to detect with 90 percent accuracy which stage 0 breast cancers [DCIS] are likely to spread and recur, according to a study published in the American Journal of Physiology-Cell Physiology...
The team stained these tissue samples so that the proteins of interest would fluoresce under the microscope. Then, using a computer vision application, researchers created a library of microscope images associated with either aggressive or non-aggressive ductal carcinoma in situ (DCIS) based on what had happened to that patient.
Researchers then showed the program roughly 100 micrographs it hadn't seen before, known as holdout images, to see how well it could accurately predict whether that patient's cancer was likely to recur...
The program is now able to correctly identify aggressive and non-aggressive disease 96 percent of the time, the researchers noted.
"That's pretty impressive when you consider that a human looking at these images would get the answer right about 70 percent of the time," Petty said. "And we've continued to work on reducing the level of false negatives."
The tool also reported false positives in four percent of cases, meaning it identified aggressive disease in patients who did not experience recurrence.
https://healthitanalytics.com/news/predictive-anal...
-
Advances in Lobular Breast Cancer Research
September 17, 2020
-
Trastuzumab emtansine plus atezolizumab versus trastuzumab emtansine plus placebo in previously treated, HER2-positive advanced breast cancer (KATE2): a phase 2, multicentre, randomised, double-blind trial
The Lancet Oncology Volume 21, Issue 10, October 2020, Pages 1283-1295
HER2-positive metastatic breast cancer is incurable and new treatments are needed. Addition of atezolizumab to trastuzumab emtansine might potentiate anticancer immunity and enhance the HER2-targeted cytotoxic activity of trastuzumab emtansine. We aimed to test this combination in HER2-positive advanced breast cancer that had progressed after previous treatment with trastuzumab and a taxane.
Addition of atezolizumab to trastuzumab emtansine did not show a clinically meaningful improvement in progression-free survival and was associated with more adverse events. Further study of trastuzumab emtansine plus atezolizumab is warranted in a subpopulation of patients with PD-L1-positive, HER2-positive advanced breast cancer.
https://www.sciencedirect.com/science/article/abs/...
https://doi.org/10.1016/S1470-2045(20)30465-4
{Abstract free; fee for full access unless you have access thru an academic/specialized library.}
-
Ugh 2027?
Verenzio -Even though the study has not yet been completed—final results are projected for delivery in June 2027—Giuseppe Curigliano, MD, PhD, the chair of ESMO's guidelines committee, is optimistic. "This is a very important trial, and the findings will change practice," he said in an ESMO press release.
-
2027 is a bummer, but when they are talking about preventing mets, they have to run the study long enough to see how it preforms over time. I am guessing 2027 is 10 years....?
-
2027... Noone will need Verzenio in 2027 anymore after TILs, enhanced CAR-Ts, TCRs, bi/tri-specific antibodies, ADCs with bystander effect, etc. will come in. Giuseppe must be a funny guy...
Saulius
-
FYI: Share will be hosting a program on:
Cannabis for Medical Disorders
Dr. Martinez, psychiatrist and a neuroscientist at Columbia University will discuss the research on cannabis for medical disorders, including risks of recreational cannabis use in medically ill patients. She will also discuss sources of cannabis plant extract for neuropathy and pain in cancer patients.
Thursday, 1-2pm ET
October 29https://www.sharecancersupport.org/cannabis-for-me...
-
New research sheds light on why tumor cells become resistant to chemotherapy
One way therapy resistance occurs is through hypoxia, or low oxygen levels. Hypoxia can occur within a tumor because it grows much more quickly than the surrounding tissue...
They found that mTOR inhibitors did mimic hypoxia and resulted in the production of different versions of three messenger RNAs (mRNAs), information carriers the body uses to produce proteins from our genes. These different versions are especially suited to allow protein production in stressful cancer conditions such as hypoxia and chemotherapy, and the production of proteins from them leads to tumor progression...
According to the researchers, when an experimental drug called ISRIB that interferes with the reprogramming of protein production—like what is happening with the three mRNAs—was administered, tumor progression was halted.
The findings have led to further questions.
One of the next steps involves looking at whether compounds such as ISRIB—a drug that has been shown to mitigate many negative effects of cancer therapy—can be used to potentially help prevent metastasis and therapy resistance.
-
Circulating Tumor DNA Analysis to Direct Therapy in Advanced Breast Cancer
- The Lancet Oncology September 29, 2020 The investigators evaluated the ability of circulating tumor DNA (ctDNA) to accurately guide mutation-directed therapy in women with advanced breast cancer. Testing was accurate (98% sensitivity with contemporaneous tissue biopsy sequencing), and treatment in the cohorts targeting HER2 and AKT mutations with neratinib and capivasertib, respectively, reached the targeted response rate.The authors concluded that ctDNA testing has sufficient validity for adoption in routine practice.
Commentary by Lee S. Schwartzberg MD, FACP... Perhaps most significantly, plasmaMATCH carefully analyzed the concordance rates between tissue biopsies and the ctDNA plasma samples for identification of genomic alterations. The sensitivity and specificity of targeted ctDNA samples were very high, >95%, when compared with contemporaneous tissue samples. Given the ease of obtaining blood samples for ctDNA analysis, these results support the use of liquid biopsy to screen for targetable alterations in all patients with MBC. The recent FDA approval of ctDNA panels as multiplex companion diagnostics provides a potentially reimbursable means for standard-of-care usage.https://www.thelancet.com/journals/lanonc/article/...(20)30444-7/fulltext{free access to press reporting (registration may be required) and to full article.} -
Counties with Persistent Poverty Rates Experience Higher Rates of Cancer Deaths
September 30, 2020
PHILADELPHIA – Residents of counties that experience persistent poverty face a disproportionately high risk of cancer mortality, according to a study published in Cancer Epidemiology, Biomarkers & Prevention, a journal of the American Association for Cancer Research.
"To prevent health disparities, we need tools, people, and systems to ensure that everyone in this country has access to the tools they need to thrive, including socioeconomic opportunities, equity, and respect, as well as prevention resources and health care services," Moss said.
"We need interventions in these communities to change cancer-causing behaviors, to make cancer screening more accessible, to improve treatment, and to promote quality of life and survivorship," she continued. "Efforts to reduce the risk of cancer in these counties will require strategic coordination, collaboration, and funding, with input from community members every step of the way."
https://www.aacr.org/about-the-aacr/newsroom/news-...
https://cebp.aacrjournals.org/content/29/10/1949
https://cebp.aacrjournals.org/content/29/10/1949
{Free access to reporting and abstract. Free for full article.}
-
'I'd love to feel a hug': Kristen Dahlgren shares one of the hardest side effects of breast cancer
NBC's Kristen Dahlgren explores a treatment that may change the way she "feels" after breast cancer.Before breast cancer, I never realized that women who have mastectomies lose feeling in their chests. It makes sense, of course — since the nerves are cut during the surgery — but it's not something that is often talked about.
....a doctor in New York City ... is doing a procedure that could change the way women feel after a mastectomy. Dr. Constance Chen, MD, a reconstructive plastic surgeon, is one of a handful of surgeons who is reconnecting nerves as part of natural tissue or '"flap" reconstruction. ... It's similar to the grafts that have been used since 2007 in arms, legs and hands.
https://www.today.com/health/kristen-dahlgren-expl...
-
Shannen Doherty Is Not Signing Off Just Yet
Fighting Stage IV breast cancer has forced some self-reflection, but the '90s icon and so-called diva refuses to slow down.
This story appears in the October 2020 issue of Elle magazine.
https://www.elle.com/culture/a34144792/shannen-doh...
{Press coverage of MBC. Creation of free account required to access full article.}
-
debew do these hypoxia induced proteins help to cause "stemness" of C cells, I wonder? the buggers that re-seed? Interesting!
-
Santa,
It looks like hypoxia (perhaps through the protein reprogramming mechanism they identified) induces a variety of C adaptations, including increased CSCs as well as plasticity and heterogeneity. If this mechanism is behind it all, hopefully the ISRIB drug will help.
Hypoxia and Regulation of Cancer Cell Stemness: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC40432...
Role of Hypoxic Stress in Regulating Tumor Immunogenicity, Resistance and Plasticity: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC62131...
-
Interesting article out from the National Cancer Institute about localized treatments for oligometastatic cancer (and an effort to re-define that term as well.) It's a call for more trials in this regard.
https://www.cancer.gov/news-events/cancer-currents...
-
Bevjen, I’m in one of the trials. It’s at MDA, called EXTEND and I was randomized to radiation to my hip bone met. The spot was stable for 3 years, hopefully, rads will kill it entirely.
Thanks for sharing that 🙂
-
Illimae,
I knew that you were in one of the trials, but didn't realize that it was linked to this.
I am having my second microwave ablation to a lesion in my liver (yay, local treatment!) on Oct. 19th and so even though it's not SBRT, I was happy to see an article reflecting this change in thinking. It provides some scientific basis for hope.
-
Thanksfor the oligometastatic article BevJen... an interesting read for those of us with only a couple of tumours and a few nodules!
-
Karen,
Good to see you popping in!
-
If local treatment for oligometastatic can extend survival, then is does matter if we find mets sooner, at least in some cases, right? (Contrary to the old party line that it does not matter.)
-
Makes sense to me. Good point.
-
Some of the recent research is very encouraging for those who are oligometastatic and for whom the lesion can be successfully excised. It is possible that this may provide long-term control or even be curative - which is very good news; however, this is the case for a *very small* percentage of patients. Additionally, and it is my understanding that timing is critical. The stage 4 diagnosis must be made and the lesion excised before there is an opportunity for the cancer to spread to additional locations. As we know, diagnosis is often not made so timely. I think that meaningful on-going surveillance will have to be the standard of care before this happens with any regularity. It's "catch it early" part deux!
-
My stage 4 Liver mets were found incidentally by a low back mri. I agree that we should get screening to catch metastasis early.
Is there a trade off between scan exposure and early diagnosis?
I think the reoccurrence numbers from some of the studies should prove we need access to scans paid by insurance, especially if we are higher risk category.
Illimae, I was offered that study but chose systemic because I had hoped to get surgical resection- gold standard. MDACC wanted to see response before they removed whole right liver lobe. Unfortunately, I am still looking for the secret sauce and the tumors grew and spread.
BTW- I did not know this, but I do not have final approval for my trial until tomorrow, either before or after the biopsy. Good thing I needed a new biopsy anyway. I start the drug on Thursday. They don’t expect any issues but could not make any promises. No wonder there is trouble getting people to participate in trials. 🤪
Dee
-
Lumpie,
You raise a good point.
However, I think that awareness is the key here -- most MOs were trained when local treatment wasn't even considered. My first MO, when asked about local treatment plus systemic, told me that she had NEVER (very emphatically) recommended local treatment for what is a systemic disease. How's that for an open mind? She wouldn't even consider it.
I also think the field of interventional radiologist in particular is showing that some things are helpful to patient condition. I am NOT oligometastatic, yet my IR, who has seen all of my scans, is willing to go back in for ablation #2 on my liver. I have diffuse bone mets, too. So I think that radiologists will be key to helping cancer patients fight for additional treatments. Just my opinion.
It makes no sense to me to say that figuring out if someone is metastatic and when is irrelevant. That type of thinking needs to be questioned by all of us.
-
Count me in as skeptical of the “catching progression or new mets early doesn’t matter “ line. The fact that de novo MBC cases fare somewhat better than early stage pts . who aren’t scanned and later go metastatic, seems to be evidence that letting Mets go undetected for longer periods, has an effect on outcomes. Yes de novo is “treatment naive” but still ... the logic of allowing pain, fractures and organ damage to take hold just escapes me.
Getting radsfor my single site of progression/ aka reawakened met site in my bone seemed a much better option than changing systemic treatment. Grateful it was offered and so far the wisdom of it has been borne out.
I would not have been considered oligo at diagnosis as I had more than five sites in bone.
-
AlabamaD, totally understandable. In my case, I already had surgery (lumpectomy) after chemo in 2017 and my single bone met remained stable, so rads was a good fit for me. I go to MDA too and was given the option of surgery since the big studies on whether it’s helps or not we’re both flawed. So far, so good but who knows in the long term.
-
BevJen, Yes - I think that local treatment is "new" though may of us wonder what took them so long. And to clarify, it is my understanding that excision is considered optimal but SRS is also very promising. I have had a few attempts at local treatment. Fortunately, my insurance agreed to pay for an attempt at ablation of a liver met - I guess that was in 2019. Many people reported to me at the time that their insurance had refused to pay for such treatment because it was deemed "experimental." I think that is a large part of the problem. Insurance gets in the way, at least in the U.S. But we also need clinical trials. Once there is decent evidence, I think insurance will be on board because, frankly, it's cheaper than the outrageous chemo prices we pay in the U.S... unless they;d just rather we die as expeditiously as possible which is also a possibility. Recent literature on radiation (SRS) is very encouraging. And I was aghast when my radiation oncologist said he thought he could get me 5 more years with CyberKnife to my liver. Nobody goes out on a limb and give numbers like that. And to someone with mets!?!? I will get my first post CyberKnife scan of liver ... probably later this month. My labs have been good and I am hoping for good news.
I posted this very encouraging article earlier this year about SRS of oligomets. Note the OS and PFS stats. They are very good.:
Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial
PURPOSE The oligometastatic paradigm hypothesizes that patients with a limited number of metastases may achieve long-term disease control, or even cure, if all sites of disease can be ablated. However, long-term randomized data that test this paradigm are lacking.
METHODS We enrolled patients with a controlled primary malignancy and 1-5 metastatic lesions, with all metastases amenable to stereotactic ablative radiotherapy (SABR). We stratified by the number of metastases (1-3 v 4-5) and randomized in a 1:2 ratio between palliative standard-of-care (SOC) treatments (arm 1) and SOC plus SABR (arm 2). We used a randomized phase II screening design with a primary end point of overall survival (OS), using an a of .20 (wherein P , .20 indicates a positive trial). Secondary end points included progression free survival (PFS), toxicity, and quality of life (QOL). Herein, we present long-term outcomes from the trial.
RESULTS Between 2012 and 2016, 99 patients were randomly assigned at 10 centers internationally. The most common primary tumor types were breast (n 5 18), lung (n 5 18), colorectal (n 5 18), and prostate (n 5 16). Median follow-up was 51 months. The 5-year OS rate was 17.7% in arm 1 (95% CI, 6% to 34%) versus 42.3% in arm 2 (95% CI, 28% to 56%; stratified log-rank P5.006). The 5-year PFS rate was not reached in arm 1 (3.2%; 95% CI, 0% to 14% at 4 years with last patient censored) and 17.3% in arm 2 (95% CI, 8% to 30%; P 5 .001). There were no new grade 2-5 adverse events and no differences in QOL between arms.
CONCLUSION With extended follow-up, the impact of SABR on OS was larger in magnitude than in the initial analysis and durable over time. There were no new safety signals, and SABR had no detrimental impact on QOL.
J Clin Oncol 38. Accepted on May 5, 2020 and published at ascopubs.org/journal/jco on June 2, 2020: DOI https://doi.org/10.1200/JCO.20.00818
-
Me too, Olma61.
Saying finding stage IV tumors early doesn't matter to length of survival implies treating tumors early when smaller or fewer doesn't matter to length of survival.
I understand there are clinical trials that indicate that is true. But show me the oncologist who would - upon diagnosing stage 4 mets in a patient - allow that patient to postpone treatment for six months or a year because "it doesn't matter when we start treatment or how extensive the tumors are when we start treating them."
No way. It HAS to matter what the blood supplies to tumors are like and how impenetrable a tumor is. My oncologist says immature tumors are easier to eradicate than mature tumors. And it makes sense to me that the bigger the tumor load the more cancer cells there are to seed additional tumors. The data on oligomets is growing.
-
My MO told me even 6 months later, the treatment would be the same. I was sad to hear this theory.
-
LillyIsHere: I think the treatment would be the same - largely because that's all they've got - but the outcomes are not the same. Higher disease burden generally = worse outcomes. Not always, but usually. They don't usually mention that part.
-
Dear all, the topic you discuss above is EXTREMELY important. The attitude doctors have is OUTDATED and comes from founding paradigm that stage IV is incurable. Yet, that is not true anymore, and now some patients are ALREADY cured with limited stage IV disease (or have a radiological pCR that is durable for the rest of their life = cure). Later (maybe even now) other patients with more widespread disease will be cured. So reacting earlier is PIVOTAL, and as I always say, waiting is A CRIME. I can tell you this... my wife, when first MRI results came, was suspected to have up to 2 mm wide-spread metastases in her liver, liver numbers suepr-normal. They said ,,suspicious for metastasis but must be observed in dynamics and compared to possible hemangiomas" and... waited... then in 2 weeks they re-scanned and they were up to 5 mm... then they said "uh, most probably metastases and biopsy is needed" and... waited for another 2 weeks until results came in and pathology confirmed extremely aggressive disease. Then they re-scanned again and mets were up to 8 mm, liver almost in failure (ALT, AST in hundreds), and they said "we cannot give chemo anymore because we are afraid liver can fail, so you decide whether you call it a day or try your luck". And so, with tears in our eyes we signed "we take chemo on our own risk". After that she reacted excellently to treatment, so we got lucky but boy oh boy... 12 3-weekly taxoteres... then another 6 after one year... why could they not give her THP (with primary tumor being 7 cam anyway) straight from the beginning??? Why wait for 4 more weeks to "confirm" that she is stage IV de novo? And what if the outcome would have been different? When I know how she reacted to treatment, I could tell you if they had started with THP when mets were suspected (2 mm), mets would have gone after first treatment... and maybe we could do not 12 chemos but 4 or 6 and have same result... so any MD or researcher who says that timing is not important lives "in another world". In this case, when they one day will get cancer, especially become stage IV, would they wait themselves and not go for treatment right away? I do not believe that. Saulius
-
Saulius,
I couldn't agree with you more. I think that most of the oncologists that we all deal with were trained at a time when the prevailing theory was that you just watch and wait to see what develops, as with your wife. But what the heck are we watching and waiting for? Clearly it's not going to improve outcomes and it becomes a self-fulfilling prophecy. Your wife's story is a cautionary tale, but I'm sure that happens to a whole lot of people. With me, they literally could not find anything on the scans for a whole year after my tumor markers started going up. I had to ask for additional scans during that time period that still didn't show anything. Then, boom, a year later -- mets. But now that I know what I know about scans and reading of scans, I wish that I had had some of those scans in that one year time period re-read because I'll bet that a radiologist could have found something. Maybe, maybe not. But again, when my liver mets were finally seen on a CT and an MRI, when I asked about local liver treatment, my original MO said "absolutely not -- I have never recommended that in 30 years of medical practice." So as patients, we have roadblocks along the way.
-
Tectonic Shift - you hit the nail on the head perfectly. Imagine being diagnosed with mets and telling your doctor “Ok doc, see ya in six months! I have a world tour coming up and I’ll start treatment when I get back!” 😂Of course they couldn’t stop us, but no way they’d be giving a blessing to that. Ditto for any Stage IV person wanting to take six months off from a treatment that keeps them stable.
-
OK ....been reading here re Oligometastatic and very touched by some really passionate stories....plus a recurrent theme that MOs aren’t seemingly up to date.... is that actually the case? Are we as a group of people with a vested interest, ie living, actually best placed to comment when we don’t really know the underpinning reasoning / research behind systemic V targeted ablation treatment?
I think we are... and we deserve a clearer explaination....so what do we DO about that?
-
Dee asked above, “Is there a trade off between scan exposure and early diagnosis?“ If my then oncologist had bothered to do a physical exam, to press on my upper abdomen, and ask if I had any pain there, I would have had the liver mets diagnosed a lot sooner even without a scan. Maybe even oligometastatic. Or maybe eligible for hormonal therapy. But as it was, I had numerous liver mets, some large, and had to go straight to chemo.
-
I am about to have what I am told is an ablative treatment. My most recent PET showed no current activity in my bone mets (that's where my mets are so far) but a slightly enlarged periclavicular lymph node behind my left clavicle. I met with the oncology radiologist today. She seems confident (she reports that her success rate is 90% on this sort of situation) that she can blast (and completely decommission) this node with 5 stereotactic sessions. The risk, which she describes as slight, is "swelling" in that arm, which I assume would be lymphedema. She has not to date had a patient have that side effect but wanted to disclose the possibility. She was very encouraging that we may be able to keep things at bay for a while with occasional blasts in areas as needed, assuming that Xeloda continues to work. Fingers crossed that she's right. Interestingly, she was a summa cum laude graduate in chemical engineering, before she went to medical school. Smart girl.
-
Lynn,
Very interesting, and I'm sure you will do well. I know that others have looked into SBRT for particular spots, and it seems that it is very well suited for that purpose. I wish you well, and it sure sounds like you are in good hands. When do you start?
-
Dear Lynn, so PET showed NEW activity in that lymph node? Or is it increasing (what size is it?)? I mean how have they determined that it is malignant? People can have inflamed/increased lymph nodes for various reasons. Just curious... Sorry Lumpie for hijacking this thread - we'll be over soon...
Dear BevJen, yes, you, my Sandra, there are so many who are victims of formalities and strict protocol following. I recon they waited for a month to confirm Sandra had stage IV de novo to give her THP combo which was approved for that time for stage IV only but it was a clear mistake, as they could have started with Taxotere+Herceptin right away (as for early stage disease, because stage III was already confirmed), and then add Perjeta later. They did the same thing in CLEOPATRA for the control group. If only I had known at that time what I know now, I would have demanded treatment right away, and Sandra would have had a much lower disease burden (here we talk about 2-3 times in volume) at the start of treatment:/ This is crazy...
Saulius
-
BevJen and Saulius-
Here's what the September 30th PET (I have a PET every 3 mo) report said:
No FDG avid axillary lymphadenopathy however, a small asymmetrical FDG avid focus is seen in the left periclavicular area with SUV of 2.8. This was not definitely seen in the prior scan. Though the size was not noted in the report, my MO spoke with the radiologist, who said it was 8mm and that it had visibly increased in size.
I have, per the report, "Multiple sclerotic foci throughout the spine and pelvis without any focal FDG uptake. Some sclerotic areas are also seen bilaterally in the ribs, over the scapulae and head of the humerus bilaterally", and this has been the case since mets were first found in Feb 2017 (initial stage II BC treated in 1991) but no pain. Other PET reports have noted sclerotic mets throughout the skeleton.
The radiologist cannot have meant that she could do anything with those innumerable skeletal mets when she talked about the possibility of further future SBRT "maintenance" (my word) blasting but rather specific spots which may occur. She was rational and encouraging, which was nice. I don't buy anything at face value, because all can change so quickly, but I intend to proceed with the SBRT and hope for the best with this spot. Fingers crossed....
-
Hope all goes well Lynne!
-
wishing you great results JoynerL, sounds like a good plan of action
On another note, I found a way to “rent “ that paper on “A Novel Staging System For MBC” . I will share some of it in another thread, a bit later, for anyone interested.
-
Dear Lynn, thanks for explanation. I am all hands for local treatments, just it was interesting how they make these decisions. Seems like your doctors are very much involved with your case and that is just great to hear. All the best for you, please keep us posted... Saulius
-
Lynne
Glad they are proceeding in the SBRT.
WHACK-A-MOLE!It worked on my lung met- no growth in 5 months
Dee
-
EAPC 2020: Dental Treatment Is a Risk Factor for Denosumab-Induced Osteonecrosis of the Jaw in Patients With Bone Metastases
PracticeUpdate Editorial Team October 09, 2020
Incidence of the disorder was found to be clinically relevant.
Avulsive or other dental treatment has been shown to be a risk factor for denosumab-induced osteonecrosis of the jaw in patients with bone metastases. The incidence of the disorder was found to be clinically relevant.
This outcome of a retrospective, observational study was reported at the virtual 11th Research Congress of the European Association of Palliative Care (EAPC).
{Physicians in Itally} set out to assess the incidence of osteonecrosis of the jaw in patients receiving denosumab and to evaluate the role of potential risk factors.
In 753 patients followed for a median of 17 months, 55% and 19% suffered from breast and prostate cancer, respectively, and 9.3% had undergone antibiotic prophylaxis before treatment. Denosumab was administered a mean of 15 (interquartile range, 6-24) times.
Overall, 53 patients (7%) developed osteonecrosis of the jaw (24-month crude cumulative incidence, 5.9%; 95% CI, 4.3-8.1).
Multiple regression results indicated the strongest predictive factor for osteonecrosis of the jaw to be avulsive or other dental treatment (P < .001).
Older age was significantly associated with a lower incidence of osteonecrosis of the jaw (P = .032).
Despite a lack of significance due to a small number of events of osteonecrosis of the jaw, chemotherapy or hormone therapy and angiogenesis inhibition were associated, respectively, with a lower and higher incidence of osteonecrosis of the jaw.
The role of angiogenesis inhibition deserves attention with regard to its relation to osteonecrosis of the jaw in patients with bone metastases.
https://www.practiceupdate.com/C/107864/56?elsca1=emc_enews_topic-alert
{Registration, no fee, may be required to access article.}
-
Thanks Lumpie. I'm up for Prolia Shot #10 the first of the year. I'm assuming I qualify as "OLDER" so maybe I'll have less risk.
Even though I looked up 'avlusive', I'm not sure what this means: Multiple regression results indicated the strongest predictive factor for osteonecrosis of the jaw to be avulsive or other dental treatment (P < .001).
-
MinusTwo: I don't have bone mets so I'm not super up on some of the necrosis concerns. I happen to know a couple of people who have had issues recently so I am somewhat attentive to related issues. I consulted Dr. Google and came up with a couple of articles referencing "a delicate surgery extraction or nontraumatic avulsion of the teeth" and "treated via nontraumatic avulsion and closure..." so I take this to be a particular technique for either extraction or something related/similar. Perhaps others can enlighten us. Thx.
-
It was a busy week so I am going to circle back to the oligo mets discussion. sometimes progress seems to come so slowly. I think that we are still living in the wake of the time when mets were difficult to diagnose and there were limited treatment options. Now, we are living in the time of mets being expensive to diagnose - and insurance not wanting to pay for it. I get very frustrated when presented with a mathematical equation that says: "it would cost us ...some number... $250K in tests to get you one more year of life and it's just not worth it." They're not practicing medicine, they're practicing economics. We can agree that we need more cost effective surveillance... and I hope that research will focus on that. But hearing that it's just too expensive and that we're not worth it is a offensive and... it's hitting us when we are down.
This affects me personally. I had no idea it was so difficult to get an initial cancer diagnosis. I thought if you had cancer it would be obvious because... they would just run a test and find out (note to readers, it also requires marginally competent physicians). And many of us are fighting the battle about brain mets. When they know that there is a > 50% chance that they will develop but the protocols still do not include periodic screening, that is very hard to understand.
Thanks for indulging me.
-
Lumpie, brain mets can be very difficult when you suspect them but doctors don’t want to order the MRI without clear symptoms. Being HER2+ and having an MO who specializes in it and brain mets, I was lucky but I have suggested that others fake a headache if necessary to get the scan. I hate to do that but sometimes we have to force the issue.
-
I know some who have faked headaches. The brain scan was one motivation for my enrollment in a clinical trial: a brain scan was part of the enrollment protocol. Crazy how we feel pressed to "play" the system.
-
Lumpie,
Some of us are old enough to remember a lot about the "military-industrial complex" and the controversies over that. Now, we are living with the "big Pharma medical complex" and, as you said, we are just a cog in the wheel. It is incredibly ridiculous that more attention is not paid to this. Yesterday I had a conversation with someone who seemed to be fairly intelligent and well educated. When I said that I had metastatic breast cancer, here was her response: oh, BC runs in my family. I get regular mammograms. But what is metastatic BC? That just goes to show that even though there are those ridiculous commercials with all of the people so happy to have MBC, there is not only a services gap for us, there is a recognition gap. And to top it all off, even medical education must be against us bc so many docs think that you cannot do anything for MBC folks. Very frustrating.
-
Yip...I feel somewhat written off at the moment, and I do think staff are just too swamped to actually read the research. They are firefighting so we have to flag stuff up.
As to playing the system, these are our lives, if the system doesn’t support us well enough then we are forced to play it. I think the women in here are smart enough and tough enough to do that....we do it for ourselves and also those who don’t have the wherewithal to play the game, which just might be a game changer. There are many before us who have played the system just to get the things we now take for granted. Absolutely no shame in that!
-
Early on in my diagnosis, my MO told me in a sad voice that my only options for treatment were systemic chemo infusions. And those would not be very long as MBC was basically a death sentence, more for palliative care. I thought to myself this cannot be true! With my background in research, I looked through PubMed for information and treatments for my disease. I was able to locate many articles on using systemic chemo coupled with localized treatments to treat ogliometastic breast cancer. I am currently NED and no longer having infusions. The MO says he is now treating me with curative intent due to my research and persistence.
Many thanks to the info I was able to get from BCO and this thread especially. My MO says he may be leery of treating any more librarians as they keep him on his toes and thinking. LOL!
-
JCSLibrarian,
Great story. The bigger question is this: do you still see that same MO? I would have run for the hills, especially based upon your research!
-
I agree with all the sentiments here about early MBC dx. Re: brain MRIs, although Her2 tends to move to the brain, scanning is not standard of care without symptoms. After year two of my dx, I talked it over with my MO saying we scan my body, but never my brain and I'd like to know sooner than later. She told me insurance will not pay without symptoms, "so give me something." It is sad that we must lie to get what we need, but she agreed and ordered the MRI. She listed that I was experiencing vertigo. Now that I have history, she's able to order one each year without me requesting or giving symptoms. It all can be so frustrating for us and MOs.
-
Thanks to everyone posting. The wealth of knowledge in this thread plus what you all bring to the thread is so helpful for everyone
-
I think brain MRIs should be standard. My grandmother died of breast cancer in the brain in the '70s. Okay there wasn't so much testing to do back then. But about 8 years ago a friend died of ovarian cancer in the brain. They had been scanning her body and thought she was NED from ovarian. Until one night she had a seizure. She was gone by morning. No one checked her brain.
-
TectonicShift: Yup. Regrettably, that is standard of care (at least in the US). If you are not exhibiting pronounced symptoms, "we don't go looking for problems."
Clearly, we need to be doing more advocacy around changing this standard. I know that some active MBC advocates are working on this issue but I don't know whether the advocacy is being "sponsored" and supported by any organization. It is my understanding that there is a clinical trial doing research around the premise that identifying brain mets earlier may improve outcomes. I'll post a link if I can find anything.
Here it is:
Screening Magnetic Resonance Imaging of the Brain in Patients With Breast Cancer
ClinicalTrials.gov Identifier: NCT04030507https://clinicaltrials.gov/ct2/show/NCT04030507?te...
Trial site is in Boston, MA. The study is recruiting.
-
Thank you, it is good to know they may be exploring this issue in research, Lumpie.
I am one who kind of exaggerated some real symptoms I was having at diagnosis, in order to get a brain MRI. The second time I had one, I had some real symptoms and got the MRI in the ER (but no brain mets found). My former MO once discussed having another one done, after one of her other patients insisted on it and did indeed have brain mets. But then she discouraged me, saying, well, if we find anything then you have to go through an MRI every 2 months. I declined simply because, at that point, I really DIDN'T want to look for a problem. But, in reality, yearly screening brain MRIs would make sense.
As for "give me something" I remember when I went for my spine rads, the nurse asked if I was having pain. I replied "only if my insurance co. wants me to". She laughed. That statement can actually be taken two ways, couldn't it? : o
I really do agree that MBC patients are still being "written off" in many ways, although so many of us are outliving the current "median OS" stats. They've given us some more effective treatments, maybe they should start treating us as if MBC already IS the proverbial "chronic disease" that it one day may become.
-
I insisted on a brain MRI at original DX due to my grandmother dying of breast cancer in the brain. I insisted. I've had a couple more since then too (almost 9 years ago).
From what I understand it's relatively difficult for cancer to spread to the brain but it's also relatively difficult for it to spread FROM the brain. The blood-brain barrier is very complicated and the brain is not like other organs. So if you have brain mets and can cut them out or zap them away, sometimes that really does the trick. I remember reading about a patient at MD Anderson who was stage IV with only oligomets in the brain. They treated with gamma knife I think, and like five or six or maybe seven years later she was still fine and NED. But if a brain tumor advances to the point of causing a seizure, it's usually too late.
-
ESR1 Mutations and Overall Survival on Fulvestrant versus Exemestane in Advanced Hormone Receptor–Positive Breast Cancer: A Combined Analysis of the Phase III SoFEA and EFECT Trials
https://clincancerres.aacrjournals.org/content/26/...
& plain language summary: "Patients with metastatic breast cancer carrying a particular mutation fare better on one form of hormone therapy than another and can be identified using a blood test, according to a new study.
In a combined analysis of two major Phase III clinical trials, called SoFEA and EFECT, researchers were able to show that patients with advanced hormone-receptor positive breast cancer, which has developed a mutation in its androgen receptors called ESR1, fared better on a hormone therapy drug called fulvestrant, compared with another called exemestane." https://www.icr.ac.uk/news-archive/new-study-sheds...
ESR1 can be identified through liquid biopsy
-
BevGen - I did not change MOs. My feelings were that he opened his mind to doing something else and being more attuned to his patients. We have a great relationship.
-
JCSLibrarian, I love your story! That is very encouraging. I'm glad that your MO was open minded too.
-
Dear JCSLibrarian... wow, you met a wise doctor... but again your story shows how important self-advocating is. Thank you for your story...
Saulius
-
I might have missed this earlier in the year but the SABCS 2019 videos are available for free online
https://watch.ondemand.org/sabcs2019.htm
-
great share, moth,thank you
-
Oncologic Outcomes No Worse With Newer Mastectomy Methods
— Nipple- and skin-sparing techniques match conventional mastectomies in retrospective study
MedPage Today October 14, 2020
For breast cancer patients receiving neoadjuvant chemotherapy (NACT), long-term oncologic outcomes for immediate breast reconstruction with nipple- or skin-sparing mastectomy were comparable to total mastectomy without reconstruction, a case-control study from Korea found.
https://www.medpagetoday.com/hematologyoncology/br...
Primary Source: JAMA Surgery
Secondary Source: JAMA Surgery
Source Reference: Fayanju OM, et al "Oncologic outcomes after neoadjuvant chemotherapy and postmastectomy breast reconstruction" JAMA Surg 2020; DOI: 10.1001/jamasurg.2020.4138.
{Free access to press coverage. Log in may be requited. Not sure about Journals - may charge a fee.}
-
Race Impacts Clinical Outcomes in HR-Positive, HER2-Negative, Node-Negative Breast Cancer
Journal of the National Cancer Institute October 08, 2020
- In this post hoc analysis of the TAILORx trial, the authors report higher rates of disease recurrence and mortality in black women compared with white women with HR-positive, HER2-negative, node-negative breast cancer. Multivariate analysis revealed that this racial disparity was not explained by 21-gene recurrence score, ESR1, PgR, HER2 RNA expression, clinicopathologic features, or treatment differences.
- There is a need for greater awareness of racial disparities and increased representation of black patients in clinical trials. Additional investigation is needed to clarify the reasons for this racial disparity.
Commentary by Lee S. Schwartzberg MD, FACP{Free access to both press coverage, abstract and full journal article.} -
Material and psychological financial hardship related to employment disruption among female adolescent and young adult cancer survivors
Cancer First published: 12 October 2020
The importance of addressing adverse financial effects of cancer among adolescents and young adults (AYAs) is paramount as survival improves. In the current study, the authors examined whether cancer‐related employment disruption was associated with financial hardship among female AYA cancer survivors in North Carolina and California.
Financial hardship related to employment disruption among female AYA cancer survivors can be substantial. Interventions to promote job maintenance and transition back to the workforce after treatment, as well as improved workplace accommodations and benefits, present an opportunity to improve cancer survivorship.
https://acsjournals.onlinelibrary.wiley.com/doi/10...
https://doi.org/10.1002/cncr.33190
{Free access to abstract. Fee for full article.}
-
Just for info, as this pertains to those of us moving into second line treatment where it seems we can’t access Faslodex in combo with a Cdk4/6 inhibitor if we’ve already had an inhibitor...

Scotland backs Pfizer's Ibrance for breast cancer
Phil TaylorJuly 11, 2019
Pfizer's Ibrance has been approved for use by the NHS in Scotland as a second-line treatment for advanced breast cancer after hormonal therapy.
The Scottish Medicines Consortium (SMC) said Ibrance – a CDK4/6 inhibitor – can increase the time before the condition progresses and delay the need for chemotherapy in people with hormone receptor-positive, HER2-negative advanced breast cancer.
Pfizer's drug was backed for use alongside anti-oestrogen drug fulvestrant for these patients under the SMC's Patient and Clinician Engagement (PACE) process, which is used for medicines to treat end of life and very rare conditions.
It is estimated that around 400 women could be eligible for treatment with the drug each year in Scotland. South of the border in England, the National Institute for Health and Care Excellence (NICE) is still deliberating on this use for Ibrance with a decision due before the end of the year.
At a PACE meeting to discuss Ibrance, patient groups and clinicians said that this stage of breast cancer is incurable and treatment options are limited.
"We know that this approval from the SMC will be meaningful for the many patients and families who are affected by this type of advanced breast cancer," said Pfizer UK's oncology medical director Dr Olivia Ashman. "We hope the same outcome will be reached by NICE later this year."
In the PALOMA-3 trial, Ibrance was shown to increase the time before the condition progresses, allowing patients additional months of life, and could also delay the need for chemotherapy with its associated side effects.
Ibrance has been approved for NHS use in Scotland since December 2017, when the SMC gave the green light for restricted prescribing of the drug in first-line HR+/HER2- breast cancer in combination with aromatase inhibitor drugs.
First-line use of the drug south of the border was rejected by NICE earlier that year but given the nod after Pfizer agreed a price reduction. Two other CDK4/6 inhibitors – Novartis' Kisqali(ribociclib) and Eli Lilly's Verzenios (abemaciclib) have also been approved by the SMC and NICE for first-line use.
Both are also trying to get the okay for second-line use with fulvestrant. Kisqali was turned down by NICE for this use in April and is still under review by the SMC with a verdict due later this year. Verzenios meanwhile has been approved in England for previously-treated patients, but only via the Cancer Drugs Fund.
Ibrance was the first CDK4/6 inhibitor to reach the market and is already a blockbuster with sales of around $4 billion last year. It is predicted to swell to $6 billion by 2022, staying well ahead of its rivals although both Novartis and Lilly's drugs are expected to compete closely for second place in the market.
Earlier estimates by EvaluatePharma give Kisqali the edge over Lilly's drug with predicted sales of $1.6 billion in 2022, with Verzenios not expected to be far behind.
-
[Early research in vitro and mice]
Calcium bursts kill drug-resistant tumor cells
Multidrug resistance (MDR)—a process in which tumors become resistant to multiple medicines—is the main cause of failure of cancer chemotherapy. Tumor cells often acquire MDR by boosting their production of proteins that pump drugs out of the cell, rendering the chemotherapies ineffective. Now, researchers reporting in ACS' Nano Letters have developed nanoparticles that release bursts of calcium inside tumor cells, inhibiting drug pumps and reversing MDR...
The researchers made a "calcium ion nanogenerator" (TCaNG) by loading calcium phosphate nanoparticles with the chemotherapy drug doxorubicin and then coating them with molecules that would allow TCaNG to target and enter cancer cells. Once inside cells, TCaNGs entered an acidic compartment, where the TCaNGs disintegrated, releasing both doxorubicin and bursts of calcium ions. When the team tested TCaNG on cancer cells in a petri dish in the lab, both ATP and P-gp production decreased, which allowed doxorubicin to kill the previously resistant tumor cells. When tested in tumor-bearing mice, TCaNG-treated mice showed significantly smaller tumors after 21 days of treatment than control mice, with no apparent side effects.
https://phys.org/news/2020-10-calcium-drug-resista...
DOI: 10.1021/acs.nanolett.0c03042
-
From the journal of International Journal of Clinical Oncology, potential biomarkers to evaluate effectiveness of Ibrance / CDK4/6 inhibitor.
-
[Early, basic research]
Breast cancer study uncovers new RNA targets for treatment and diagnostics
The team discovered that two lncRNAs named TROLL-2 and TROLL-3 are associated with the progression of breast cancer. Tamping them down inhibited breast cancer formation in mice...
They went on to show that when Tap63 is downregulated, there's a complex interplay between the lncRNAs and other proteins, including one called WDR26. That stimulates AKT signaling, promoting the development of invasive breast tumors....
The researchers believe their findings could be used in several ways to diagnose and treat cancer. For example, they could help predict which patients are likely to respond to AKT inhibitors. There are several in development, including Roche's ipatasertib, which the company is testing in breast and prostate cancers.
There could be treatment applications, as well, said Elsa Flores, Ph.D., who leads Moffit's department of molecular oncology and cancer biology and evolution program. The findings could point to targets for "therapies against metastatic cancers with alterations in TP53 and hyperactivation of the PI3K/AKT pathway," Flores said in a statement.
https://www.fiercebiotech.com/research/breast-canc...
-
News you can use:
From AACR Annual Meeting 2020
“...Circadian melatonin signal disruption by exposure to artificial light at night promotes bone lytic breast cancer metastasis"
https://cancerres.aacrjournals.org/content/80/16_Supplement/LB-212
A good plain-language summary is here:
https://foodforbreastcancer.com/
Bottom line: Sleeping in a very dark room may help prevent mets. Melatonin supplements If needed may be a good thing.
-
Studies have shown that women who work night shift have a higher incidence of breast cancer and now this.
I am definitely in this category...staying up all night , falling asleep with tv on, laying in bed restless looking at my tablet, etc.
Have been like this for years prior to diagnosis. Just recently was able to adjust my sleep schedule after another year of tossing and turning til 5 am. I am holding on for dear life, holding on to being able to fall asleep in the dark and wake up at sunrise.
And with that...good night
-
olms61 - I hope you slept well!
This article is scary about COVID-19 and cancer. “Patients with cancer and COVID-19 have a higher risk of severe disease and mortality, researchers reported.“
“If the patient was neutropenic, the mortality was very high -- six of nine died.”😳
I have been slightly neutropenic for a year. I also was planning to have all the kids for Thanksgiving. COVID +Cancer sucks.
https://www.medpagetoday.com/meetingcoverage/chest...Dee
-
Dee, thank you, I slept pretty well and had to get up early for my infusion today. All good.
Yes, COVID just makes our already complicated lives exponentially more complicated. Praying for a resolution to this and soon. -
yeah it's never a good time to get Cancer but, Cancer+COVID sucks.
-
Thank you for posting that, Dee. I have sent the article along to a few people in my life who need to know that information. :-)
-
Shetland the recommendation I got was 1. to black out all lights in bedroom, 2. to take 20mg (--work up to this slowly!) of melatonin at roughly the same time each night, and 3. to keep my BR cold. You can have all the blankets you want but the room itself should be cold (under 68 ideally). I believe the cold promotes the production of brown (metabolically active) fat.
Circadian rhythms govern the 'wake/sleep' cycles of cancer cells, too, and this can influence when the drugs are the most effectively administered. ('Chronomodulation')
-
Accuray announces ClearRT Helical kVCT Imaging For #Radixact - 510(k) pending
Note: this is a marketing piece. Long on images, short on details.
Provides some information on improved imaging soon to be available from Accuray, U.S. based makers of CyberKnife, one of the frequently used tools for SRS (Stereotactic radiosurgery).
-
Efficacy and Safety of Chloroquine in Combination With Taxanes for Advanced or Metastatic Anthracycline-Refractory Breast Cancer
October 24, 2020
Published in Clinical Breast Cnacer
- The authors of this small phase II study evaluated combination treatment with chloroquine and taxane or taxane-like chemotherapy in women with locally advanced or metastatic breast cancer refractory to anthracycline-based chemotherapy. The overall response rate of 45% exceeded the expected benchmark of 30%, and the median progression-free and overall survivals were 12 and 25 months, respectively. The combination was well-tolerated, with a rate of 13% of grade 3+ adverse events.
- Larger studies are warranted to evaluate this combination.
https://www.practiceupdate.com/C/107842/56?elsca1=...
https://linkinghub.elsevier.com/retrieve/pii/S1526...
DOI:https://doi.org/10.1016/j.clbc.2020.09.015
{Free access to practice update. Registration may be required. Free access to abstract. Fee or subscription for access to full article.}
-
Chloroquine is gaining some recognition in combo with taxanes: https://www.practiceupdate.com/content/efficacy-an...
Saulius
-
Thought this was interesting.
High-Dose SBRT More Effective for Painful Spine Metastases
— Roughly one-third of patients had a complete pain response at 3 and 6 months
AlsoMDACC has a trial for
Hydroxychloroquine, Palbociclib, and Letrozole Before Surgery in Treating Participants With Estrogen Receptor Positive, HER2 Negative Breast Cancer
https://clinicaltrials.gov/ct2/show/NCT03774472
Dee -
Article for clinicians on various treatments options for bone mets. Very interesting, if technical:
-
good article,Joyner. I printed it out to save. Thanks
-
Lynn,
That was a great article about bone metastases. I had seen bits and pieces of the info in there in different articles, but not in such a consistent, complete way. I did note that this was a study headed up by the Europeans -- confirms my belief that we should look at what docs in other countries are doing as well as info about US progress in treating MBC.
I think I'm going to send this one to my MO. Maybe then she won't think I'm crazy when I ask her about local treatment for bone metastases -- the standard American protocol seems to be treatment for pain, only. This article goes beyond that.
-
Stereotactic radiosurgery may be new standard of care for four or more brain metastases
October 27, 2020
Stereotactic radiosurgery conferred equivalent OS as whole-brain radiation but with less cognitive decline in patients with four or more nonmelanoma brain metastases, according to study results presented at the virtual ASTRO Annual Meeting.
"Up to 30% of [patients with cancer] develop brain metastases at some point during the disease process and these patients typically do not do well with current treatment modalities, including radiation and surgery,"... "Whole-brain radiation has been around for some time now; however, it is associated with significant side effects, which is why within the past decade there have been tremendous efforts to minimize the cognitive side effects of brain radiation."
At median follow-up of 6.6 months, results showed patients in the stereotactic radiosurgery group scored higher on memory function compared with baseline, whereas patients in the whole-brain radiation group scored worse compared with baseline. Researchers observed a clinically meaningful and statistically significant benefit with radiosurgery at 1 month and 6 months.
Moreover, half of patients in the whole-brain radiation group experienced a clinically meaningful decline in cognitive function 4 months after treatment compared with only 6% of patients in the stereotactic radiosurgery group.
The radiosurgery and whole-brain radiotherapy groups had similar local control rates at 4 months, median OS and median time to distant brain failure. However, patients assigned radiosurgery experienced shorter interruptions of systemic therapy, with time to systemic therapy of 1.7 weeks vs. 4.1 weeks with whole-brain radiation.
"This is particularly important because patients with brain metastases often have metastases outside of the brain, as well," Li said. "When these patients receive whole-brain radiation, we typically hold chemotherapy for 2 weeks and we continue to hold systemic therapy for up to 4 weeks for them to wash out before they can return to systemic therapy. These patients often need systemic therapy to control extracranial disease."
Radiation necrosis occurred in 17% of patients in the radiosurgery group and in 4% of all treated lesions. Grade 3 or higher toxicities occurred among 8% of patients (n = 2) in the radiosurgery group and 15% of patients (n = 4) in the whole-brain radiation group.
"Despite early termination of the study and the use of memantine in the whole-brain radiation therapy arm, we were able to show that stereotactic radiosurgery was associated with reduced risk [for] cognitive deterioration compared with whole-brain radiation as demonstrated by a constellation of neurocognitive tests, individually or by composite scores," Li said. "The results from this randomized, phase 3 trial strongly support the use of stereotactic radiosurgery in patients with four to 15 brain metastases to better preserve cognitive function and to minimize interruption of systemic therapy, without compromising OS."
Stephanie E. Weiss, MD, FASTRO
Fox Chase Cancer Center
https://www.healio.com/news/hematology-oncology/20...
Source: Li J, et al. Abstract 41. Presented at: American Society for Radiation Oncology Annual Meeting (virtual); Oct. 25-28, 2020.
{Reporting available w/o charge, registration may be required.}
-
Olaparib for Metastatic Breast Cancer and Mutations in Homologous Recombination–Related Genes
November 05, 2020 Journal of Clinical Oncology
- The authors of this phase II trial evaluated the PARP inhibitor olaparib in the treatment of 54 patients with metastatic breast cancer (76% ER-positive/HER2-negative) and either germline mutations in non-BRCA1/2 homologous recombination–related DNA repair genes (cohort 1) or somatic mutations in BRCA1/2 or other non-BRCA1/2 homologous recombination–related genes (cohort 2). The objective response rate (ORR) in cohort 1 and cohort 2 were similar (33% and 31%), but confirmed responses were only observed in patients with germline PALB2 (ORR, 82%; PFS, 13.3 months) and somatic BRCA1/2 (ORR 50%; PFS, 6.3 months) mutations.
- These findings appear to expand the patient population likely benefit from PARP inhibitors to include those with somatic BRCA1/2 and germline PALB2 mutations, in addition to germline BRCA1/2 mutation carriers.
DOI: 10.1200/JCO.20.02151 Journal of Clinical Oncology{Free access to reporting and abstract. There appears to be a fee for access to the ASCO full article.} -
Breast Cancer–Specific Mortality in Small-Sized Tumor With Stage IV Breast Cancer
October 28, 2020 The Oncologist
- This authors of this SEER database study evaluated breast cancer–specific mortality (BCSM) according to primary breast tumor size in over 5300 patients with metastatic breast cancer. Tumor size was not associated with BCSM. In patients with tumors <50 mm, the BCSM rate did not decline in association with decreasing tumor size. Among patients with triple-negative breast cancer, the BCSM rate was worst among patients in the T1a/T1bN2+ group.
- The authors hypothesize that T1a/T1b triple-negative breast cancers with regional lymph node metastases may be a surrogate for biologically aggressive disease.
{Free access to reporting and full article.} -
Re: Olaparib for Metastatic Breast Cancer and Mutations in Homologous Recombination–Related Genes November 05, 2020 Journal of Clinical Oncology
This is disappointing news for ATM or CHEK2 mutations. No response to treatment. I was hoping to have Olaparib as a future treatment option. Although I'm glad to hear the drug helps others..
-
Tinkerbell107: I note that it was a small study - only 54 patients. I hope that maybe they will look at larger pools before relying too heavily on what seems like it should be starting point info. (Hope you have lots of options - and don't need any of them for a long time!)
-
Santabarbarian, re chronomodulation — I try to get the 13-hour overnight fast, and take my pills so they reach peak levels during the night when, I believe, cancer cells are more active.
-
Lumpie: Thanks for the encouragement. Appreciate all your efforts in bringing forth the research studies.
-
Hi lumpie and tinkerbell
just anecdotal evidence but after 7 lines of chemo and being told i was out of options I privately financed a foundation one test, found somatic PALB2 and was put on olaparib. my 11cm li ver tumor is at 5,6 after 3 months../amy
-
Thanks for all, Lumpie. So important. WOW, Arolsson, and good luck, Tinkerbell-that does sound like a small study.
-
arolsson: That is great news! Just goes to show... there is still so much we don't know. I know that a lot of us think that figuring out how to effectively personalize medicine is really important to so many people's effective treatment. We are all still lab rats... but in a good way, a way that contributes to health and future treatments, I hope.
-
(I also posted this on reducing dose, AIs) . Reducing dosage. Reading "The Cheating Cell" Athena Aktipis https://press.princeton.edu/books/hardcover/9780691163840/the-cheating-cell . She explores looking at cancer from an evolutionary view. Rather than trying to eradicate/kill cancer which might actually select for cells which resist treatment, she suggests "managing" the cancer which might select for cancer that is less prone to develop resistance. One approach is "adaptive therapy" where the cancer is kept at an "acceptable" size without too much harm/risk to the patient. She also suggests "faking" described in her book and here. the cancer https://chemoth.com/metronomic/adaptive-chemotherapy... This article suggests that while a nice idea, we are not there yet. https://www.oncozine.com/personalizing-cancer-treatment-why-adaptive-therapy-isnt-there-yet/ . In some sense, adaptive therapy makes sense, can we really expect to eradicate? At the same time I want it gone gone gone, not just "manageable". She also describes, briefly, how we are abe to successfully treat and eradicate some types of cancer. I wish and hope the same for breast cancer. She is an evolutionary biologist at Arizona State University.
-
Tinkerbell107, I was on the small TBB Trial of Talzenna (another PARP inhibitor) for patients with BRACA-like mutations for almost a year. I have CHEK2 and FANCA germline mutations. The Olaparib Expanded trial evaluated similar BRACA-like mutations, and I was very sad when it did not show a response with many of the mutations (with exception of PALB2 and somatic BRACA1/2). However, as many have said, it was a very small trial. One on my friends who has a germline CHEK2 and somatic BRACA1 mutation responded well for a year on that trial, but was counted in the somatic BRACA mutation arm. I hope that further research will be done... I hope that women who might benefit from PARP inhibitors will have access to them. Despite my durable response to Talzenna, PARP inhibitors would probably not be recommended to me today...
-
Covering COVID-19 Vaccines
The Centers for Medicare & Medicaid Services (CMS) released its fourth COVID-19 interim final rule with comment period. This rule requires U.S. Food and Drug Administration-approved COVID-19 vaccines to be provided at no-cost to beneficiaries enrolled in Medicare and Medicare Advantage. Medicaid beneficiaries can receive the vaccine at no cost only during the public health emergency (PHE), and most private payors will also be required to provide the vaccine at no cost. While codes to bill vaccines will not be available until the vaccines have been approved, CMS has set reimbursement rates for single and multiple vaccine doses. Additionally, CMS is continuing efforts around transparency by requiring any provider who performs a COVID-19 diagnostic test to post their prices online.
Learn more about the fourth COVID-19 interim final rule.
Source: ASCO Advocacy News & Action
https://www.asco.org/practice-policy/policy-issues...
Links are to CMS webpage and should not involve a charge.
-
Healthcare Price Transparency
On October 28, the U.S. Department of Health and Human Services (HHS), the U.S. Department of Labor, and the U.S. Department of the Treasury released the coverage transparency final rule. Building on earlier administration actions requiring hospitals to disclose standard charges and negotiated rates with third-party payers, this new rule includes two requirements aimed at increasing healthcare price transparency in the commercial market.
First, health plans and payers will be required to provide participants, beneficiaries, and enrollees with personalized out-of-pocket cost information, and the underlying negotiated rates, for all covered health care items, services, and prescription drugs. Plans and payers must provide cost-sharing information through an internet-based self-service tool or in paper form upon request. An initial list of 500 services as determined by the departments must also be available for plans on January 1, 2023. The remainder are required to be available for plans on January 1, 2024.
Second, the rule requires payers and plans to post three data files for public use: 1) negotiated rates for all covered items and services between the plan or payer and in-network providers; 2) historical payments to, and billed charges from, out-of-network providers; and 3) in-network negotiated rates and historical net prices for all covered prescription drugs by plan or issuer at the pharmacy location level. These files are required to be made public for plan years that begin on or after January 1, 2022.
Learn more about the coverage transparency rule.
Source: ASCO Advocacy News & Action
https://www.asco.org/practice-policy/policy-issues...
Links are to CMS webpage and should not involve a charge/should be fully accessible.
{That is pretty huge if we can see what they are charging whom for services. Too bad it is so far off in the future.}
-
FDA Approves Liquid Biopsy NGS Companion Diagnostic Test For Multiple Cancers And Biomarkers
November 9, 2020On October 26 and November 6, 2020, the Food and Drug Administration approved the liquid biopsy next-generation sequencing-based FoundationOne Liquid CDx test (Foundation Medicine, Inc.) as a companion diagnostic device for multiple additional biomarkers detected in cell free-DNA isolated from plasma specimens.The companion diagnostic indications in the October 26 approval are 1) to identify mutations in BRCA1 and BRCA2 genes in patients with ovarian cancer eligible for treatment with rucaparib (RUBRACA, Clovis Oncology, Inc.), 2) to identify ALK rearrangements in patients with non-small cell lung cancer (NSCLC) eligible for treatment with alectinib (ALECENSA, Genentech USA, Inc). and 3) to identify mutations in the PIK3CA gene in patients with breast cancer eligible for treatment with alpelisib (PIQRAY, Novartis Pharmaceutical Corporation).On November 6, FDA approved the FoundationOne Liquid CDx test as a companion diagnostic device to identify mutations in BRCA1, BRCA2 and ATM genes in patients with metastatic castration resistance prostate cancer (mCRPC) eligible for treatment with olaparib (LYNPARZA, AstraZeneca Pharmaceuticals LP).FoundationOne Liquid CDx approval as a companion diagnostic for rucaparib, alpelisib, alectinib, and olaparib was based on the retrospective testing with FoundationOne Liquid CDx of available plasma samples from patients enrolled in four clinical trials that supported the approval of associated therapeutics. Efficacy for rucaparib, alpelisib, alectinib, and olaparib was shown to be maintained in patients with confirmed BRCA1 and/or BRCA2 gene alterations, PIK3CA mutations, ALK rearrangement, and BRCA1, BRCA2, and/or ATM gene alterations, respectively, by FoundationOne Liquid CDx. If the specific mutations and alterations associated with these approvals are not detected in the blood, then a tumor biopsy should be performed to determine if the specific mutations and alterations are present.View the Summary of Safety and Effectiveness for the FoundationOne® Liquid CDx test (P200006 and P200016).The FoundationOne Liquid CDx test was granted Breakthrough Device designation, in which the FDA provides intensive interaction and guidance to the company on efficient device development.A description of the FDA Breakthrough Device program can be found at Breakthrough Devices Program Guidance for Industry and Food and Drug Administration Staff.Source: ASCO Advocacy News & Action
https://www.asco.org/practice-policy/policy-issues... -
Copay Accumulator Programs Block Access to Necessary Cancer Treatments
October 27, 2020Beginning January 1, UnitedHealthcare (UHC) will ask physicians to provide information on the copay assistance funds patients receive for their treatments. UHC would then enforce a copay accumulator, which would ensure that no copay assistance funds are applied toward patients' deductibles or out of pocket maximum payments.In response, the Association for Clinical Oncology (ASCO), along with a dozen other medical specialty societies sent a letter to UHC urging the organization to not move forward with its proposed copay accumulator initiative or physician reporting on copay assistance."Our organizations oppose this change as it would endanger patients' access to care and undermine the doctor-patient relationship," the organizations said in the letter. "We urge UHC to explore other pathways to rein in drug costs without jeopardizing patients' health."The letter acknowledges that the specialty drugs targeted by this policy are expensive; however, they are also vitally important for patients with serious illnesses such as cancer. Additionally, most of the targeted drugs have no generic equivalents or therapeutic alternatives, meaning patients do not have lower-cost options.Copay assistance programs allow patients to access potentially life-extending medications with less concern for their personal finances. Blocking copay assistance funds from being applied toward patient deductibles could result in patients facing thousands of dollars in unexpected medical bills and the discontinuation of treatment with disastrous consequences.Read the full letter.Lean more about copay accumulatorsSource: ASCO Advocacy News & Actionhttps://www.asco.org/practice-policy/policy-issues...
{Login may be required for links. Sorry - not sure.} -
More than 100 Organizations Endorse ASCO-Backed Senate Bill to Improve Clinical Trial Access
October 13, 2020The Association for Clinical Oncology (ASCO) joined more than 110 organizations representing patients, medical researchers, providers, cancer survivors and their families in signing an endorsement letter for S. 4742, the CLINICAL TREATMENT Act. This bipartisan legislation, which was recently introduced by Senators Richard Burr (R-NC) and Ben Cardin (D-MD), would expand access to clinical trials and improve the quality of cancer research by requiring Medicaid to guarantee coverage of the routine care costs of clinical trial participation for Medicaid enrollees with a life-threatening condition. The House version of the bill, H.R. 913, currently has 55 cosponsors representing both parties.In a support letter to Senators Burr and Cardin, the organizations write, "Robust clinical trial participation improves the quality of medical research. Medicaid serves many demographics, including ethnic minorities and women, that are underrepresented in current clinical trial enrollment. Lack of participation in clinical trials from the Medicaid population means these patients are being excluded from potentially life-saving trials and are not reflected in the outcome of the clinical research. Increased access to clinical trial participation for Medicaid enrollees helps ensure medical research results more accurately capture and reflect the populations of this country."Tell your Senators to cosponsor S. 4742.Read the full letter.Source: ASCO Advocacy News & Action
https://www.asco.org/advocacy-policy/asco-in-actio...{Login may be required for links. Sorry - not sure.}
-
Executive Order Would Tie U.S. Drug Prices to What Other Countries Pay
September 15, 2020On September 13, President Trump signed an executive order (EO) aiming to address high prescription drug prices by tying payments for certain Medicare drugs to the costs the treatments sell for outside the United States (U.S.). According to the EO, prices for provider-administered drugs would be linked to a "most-favored-nation price" drawn from the lowest price among countries that have a similar per-capita gross domestic product.The EO grants authority to the Secretary of the U.S. Department of Health and Human Services (HHS) to implement a demonstration project to test a "most favored nation" policy for some drugs or biologicals under Medicare Part B or Part D. The details of the demonstration are unclear, but it could begin more quickly than the typical rulemaking process.The Association for Clinical Oncology (ASCO) is also concerned about the escalating price of prescription drug treatments—particularly cancer therapies. However, as the economic crisis in the U.S. deepens, ASCO believes it is critical that any solution to this complex problem be thoroughly tested before it is implemented to ensure it does not impede patient access to care or stifle innovation in drug development.Source: ASCO Advocacy News & Action
https://www.asco.org/practice-policy/policy-issues...{In-text link is to a government site and should be freely available. Login to this article may be required for links. Sorry - not sure. Who knows what will happen to this Executive Order post-election, but it is interesting.} -
FDA grants accelerated approval to pembrolizumab for locally recurrent unresectable or metastatic triple negative breast cancer - eff Nov 13
https://www.fda.gov/drugs/drug-approvals-and-datab...
-
Lumpie you seem to be on a roll....thank you!
-
I did get on a bit of a roll. These were non-scientific but may affect access to care for many in the US, so thought I would share. Hope these help....
-
Existing antidepressant helps to inhibit growth of cancer cells in lab animals
New research has shown that the antidepressant sertraline helps to inhibit the growth of cancer cells...
Cancer cells use different biological mechanisms to stimulate their growth. In certain types of breast cancer, leukaemia, skin cancer, brain tumours and lung cancer, among others, the malignant cells produce large amounts of serine and glycine, two amino acids. This production stimulates the growth of cancer cells to such an extent that they become addicted to serine and glycine.
[A screening process involving 1600 yeast trials] showed that the antidepressant sertraline was the most effective substance. "Other studies had already indicated that sertraline has a certain anti-cancer activity, but there was no explanation for this yet", mention researchers Shauni Geeraerts (LDMC and CMPG) and Kim Kampen (LDMC). "In this study, we've been able to demonstrate that sertraline inhibits the production of serine and glycine, causing decreased growth of cancer cells. We also found that this substance is most effective in combination with other therapeutic agents. In studies with mice we saw that sertraline in combination with another therapy strongly inhibits the growth of breast cancer cells."
https://www.eurekalert.org/pub_releases/2020-11/kl...
-
I've been a baby aspirin taker for years since dx. I thought this article was interesting. Aspirin may be beneficial in patients who are not BRCA+ but harmful in BRCA + patients.
https://www.upi.com/Health_News/2019/08/12/Aspirin...
-
Another interesting post that someone made in another thread:
https://journals.lww.com/oncology-times/fulltext/2...
https://www.biorxiv.org/content/10.1101/2020.01.21...
Metformin may be helpful when metastasis is happening but harmful when BC cells are dormant and the patient is on and AI
-
One more interesting study - not breaking - but a small study to look at iodine either alone or in conjunction with chemo.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC66829...
-
Eating more fruits and vegetables may help breast cancer survivors live longer
We examined data on nearly 9,000 women with breast cancer who were followed for up to 30 years, and observed that those who consumed higher amounts of fruits and vegetables after their diagnosis were less likely to die during the study period than those with lower amounts of fruits and vegetables in their diets. High fruit and vegetable consumption, and high consumption of just vegetables, was associated with lower mortality from all causes—most women with breast cancer die from other causes. Some subgroups of fruits and vegetables were also associated with lower all-cause mortality, including leafy green vegetables, cruciferous vegetables such as broccoli, fruits and vegetables high in vitamin C, and vegetables high in beta-carotene.
We also observed that eating high amounts of blueberries was significantly associated with lower breast cancer-specific mortality, as well as all-cause mortality. This may be because blueberries contain bioactive components that may prevent or slow breast tumors from growing or spreading.
https://www.hsph.harvard.edu/news/features/breast-cancer-survival-fruits-vegetables/
-
Fertility Preservation Boosts Live Births after Breast Cancer
— Also associated with better survival
Fertility preservation (FP) appeared successful for women undergoing breast cancer treatment, data from a Swedish cohort showed.
About 23% of women who underwent FP had one or more live births after treatment for breast cancer, as compared with 9% of those going without it. FP was associated with 5- and 10-year cumulative incidences of post-breast cancer live births that were more than twice as high as rates for women who did not have FP.
https://www.medpagetoday.com/hematologyoncology/br...
Primary Source: JAMA Oncology
Source Reference: Marklund A, et al "Reproductive outcomes after breast cancer in women with vs without fertility preservation" JAMA Oncol 2020; DOI: 10.1001/jamaoncol.2020.5957.
{Free access to medical reporting. Sign-in may be required. Fee or subscripton will be required for full article access.}
-
repurposing drugs for triple negative breast cancer
https://www.researchgate.net/publication/342904316...
proton pump inhibitors like Prilosec look like they might be helpful along with chemo
very small study of 42 patients: https://meetinglibrary.asco.org/record/190369/abst...
-
pembrolizumab (Keytruda) for leptomeningeal mets - not just in triple neg breast pt. Pts in this study weren't even all breast ca pts
"Pembrolizumab (Keytruda) led to a 38% central nervous system (CNS) response rate and was well tolerated in patients with leptomeningeal metastasis (LMM) from solid tumors, according to phase 2 results" https://www.onclive.com/view/pembrolizumab-shows-i...
-
I'll be watching this one closely. There are currently no targeted treatments for p53 mutations and lots of cancers develop these mutations especially in late stage.
FDA Grants Fast Track to PC14586, Potential Therapy for Specific p53 Mutation
https://breastcancer-news.com/2020/10/29/fda-grant...
Here's the trial info. It's in San Antonio, TX.
https://clinicaltrials.gov/ct2/show/NCT04585750
-
techtonicshift
That is an interesting trial. I have genomic TP53 c.847C>T (Arg 283Cys) VUS. It is common in breast cancer but an “unknown significance” for now.
Dee
-
Covid & cancer - additional determinants of mortality
https://www.nature.com/articles/s43018-020-00129-w...
-
I am not sure if this is the place to post foods and supplements to avoid while in AI:
-
-
[CRISPR used to treat cancer in mice]
..."There are no side effects, and we believe that a cancer cell treated in this way will never become active again." Peer told the news outlet, adding, "This technology can extend the life expectancy of cancer patients and we hope, one day, cure the disease..."
The scientists used the technique on hundreds of mice – and Peer said the method could potentially be used on humans within two years.
The study focused on two types of cancers — glioblastoma, an aggressive type of cancer that can occur in the brain or spinal cord, and metastatic ovarian cancer.
Researchers found that mice with cancer who received the treatment had double the life expectancy of the control group, and their survival rate was 30 percent higher, the [Times of Israel] reported.
-
Thank you for sharing! CRISPR is so facinating. I would love to see more about this from a better news source than the NY Post! I do often look to CRISPR editing as the hope to end BRCA1 and BRCA2 mutations :-)
-
-
Interesting article from National Cancer Institute about treating bone mets with radiation
https://www.cancer.gov/news-events/cancer-currents...
-
Practicing Oncologists Debate New Tactics for Brain Metastases in HER2+ Breast Cancer
October 21, 2020OncologyLive
New approaches for treating patients with HER2-positive metastatic breast cancer are showing signs of efficacy against brain metastases, generating excitement about the potential to make critical advances and sparking questions about optimal sequencing.
Interview format article
https://www.onclive.com/view/practicing-oncologist...
{No charge for access but sign in may be required.}
-
-
NCI-MATCH Trial Identifies Actionable Alterations in More Than One-Third of Patients With Cancer
December 3, 2020
As part of the National Cancer Institute Molecular Analysis for Therapy Choice (NCI-MATCH) trial conducted at more 1000 study sites, researchers have identified actionable alterations in nearly 38% of patients with cancer, and almost 18% of patients were assigned to treatments based on their molecular profiling results.1 The patient population included a large proportion of patients with less common cancers, including gastroesophageal cancer, sarcoma, and kidney cancer, in addition to patients with the most common cancers — colorectal, breast, and prostate cancers, as well as non-small-cell lung carcinoma (NSCLC).
https://www.cancertherapyadvisor.com/home/cancer-t...
{Free access, registration may be required.}
-
Increased Overall Survival in Patients With MBC and Liver or Lung Metastases Treated With Eribulin
December 03, 2020
- In this retrospective study of 443 patients with metastatic breast cancer and liver or lung metastases who received third-line treatment with eribulin (n = 229), gemcitabine (n = 134), or capecitabine (n = 80), the authors evaluated overall survival in real-world clinical practice. A larger proportion of patients who received eribulin were alive at 6, 12, 24, and 36 months compared with those receiving gemcitabine, and more eribulin-treated patients were alive until 36 months compared with capecitabine-treated patients. Overall survival and survival among patients with TNBC and HR+/HER2− disease was numerically increased among patients who received eribulin.
- These real-world data support data from randomized clinical trials regarding the consistent effects of eribulin in this patient population.
{Free access} -
That’s very helpful Lumpie...I’m looking at what 3rd line treatment might look like for me, so this info gives me a chance to discuss with my MO. Good timing too as I speak with her this week!
-
Lumpie
I asked my MDACC team if I was in the match trial. They said yes, but never once contacted me about anything potential. I am learning that you have to be proactive to get on a trial and that sometimes it's all about timing.
My local MO read that erubulin paper. He said I can keep it in my bucket but he prefers me to try a platinum drug combo next because of the Neuroendocrine part.
Thanks for keeping us all informed!
Dee
-
I got this email from onclive -re. MBC if anyone wants to register for the webinar- Webinar for MBC
if the link doesn't work and you want to,you can LMK your email and I can forward the email to you?
-
Dee: Yes, it can seem kind of random getting on trials. Part of it is definitely timing. Other times it is all sorts of factors from timing to reaching the right person to the sheer luck of matching what is needed at any given moment. NIH tells me that they have a "desk" that is supposed to screen prospective participants for all of their breast cancer trials, but I have not felt like there was much clarity around how that screen/match process operated - you just have to trust it. I have sometimes thought .... it would be great if there were a central service that would screen and match you for all available clinical trials approved in the US. Seems to me like that might promote participation, fill trials more efficiently and allow for better management of patient participation. But I suppose that would be a sizable undertaking. Maybe someday.
-
re finding trials, I signed with Cancer Research Insititute and the service gave me a list of potential trials and there is an option for them to notify you if something new pops up. I doubt it will work well in Canada but I did it just to see. https://app.emergingmed.com/emed/home
-
I stumbled upon this article, and thought it was a very good (but sobering) article about the mechanisms of metastatic recurrence in breast cancer. This article covers the how, why, when, where, and what we can do about it.
I had my first metastatic recurrences this year. I went from NED after a local recurrence to innumerable metastatic lesions in only a few months. That blindsided me, and hit me like a freight train. In these situations it sometimes helps me to understand the science and the mechanisms behind why and how these things happen. I thought this article might be helpful for others, too.
Here are a few key takeaways from the conclusions sections, but the whole article is really interesting:
"[O]ur current understanding of metastatic dormancy, metastatic evolution, acquired resistance and metastatic niches suggests that detecting and treating recurrence earlier might be our best opportunity to improve patient outcomes.
Despite metastatic disease being the main cause of death in cancer patients, knowledge about the biology of this lethal process is lacking. However, with advances in genomic sequencing technologies and accumulating data in favour of the predominance of the parallel model over the linear model of dissemination, four important lessons have been learned. First, in most patients who will experience recurrence, metastases are already present at the time of diagnosis. Second, despite their genomic similarity to the trunk of the tumour's evolutionary tree, metastases are distinct biological entities, containing important phenotypic differences compared with their primary source. Third, metastases, as well as primary neoplasms, are subject to evolution dictated by pharmacological pressure, tissue-specific environments and cellular plasticity. Finally, some micrometastases might exist in a non-proliferative, dormant-like state for months to decades.
Altogether, these data have significant clinical implications. First, attempts to prevent initial metastatic dissemination might hold little therapeutic benefit—even though early detection and treatment of most primary breast tumours is curative, tumours that are 'born to be bad' probably disseminate prior to diagnosis. Next, caution must be taken when using primary tumours as a proxy for clinical decisions on systemic therapies to prevent or treat metastatic disease, unless little divergence between paired lesions is observed. In this respect, non-invasive liquid biopsy biomarker assays could help to identify molecular changes in metastases. In addition, an urgent need exists to assess the phenotypic properties of DTCs in their native states, in order to understand how some DTCs, but not others, contribute to metastatic recurrence. Finally, it might be possible to exploit tumour dormancy in some, but probably not all, cases as a window of opportunity to tackle MRD and/or prevent metastatic relapse (Table 1).
Future directions should be centred on identifying dangerous versus indolent DTCs and finding new DTC drug targets, while also using modern imaging and biomarker assays to accurately determine who needs such therapy, in order to avoid overtreatment. Importantly, all of the above strategies—prevent, reverse, prolong and eradicate dormancy (Table 1)—will require the development and use of more clinically relevant models and human samples, as well as clinical trials of new 'intensive' follow-up monitoring programmes. With progress in these areas, it is hoped that new knowledge will converge in the near future to prevent recurrences and deaths from cancer."
-
buttons machine,
Really interesting article that is readable and makes a lot of sense.
I had my initial recurrence as a single site metastasis in 2006. At the time, I urged my oncologist to hit it hard -- fulvestrant was just coming into the picture, and I asked her if we could try that. Her answer was no. But I found this interesting in the article:" However, our current understanding of metastatic dormancy, metastatic evolution, acquired resistance and metastatic niches suggests that detecting and treating recurrence earlier might be our best opportunity to improve patient outcomes." It does upset me to read that, and to know that the guidelines at the time were telling docs that they should only go so far in treating metastases.
However, there is hope on the horizon with the advent of ctDNA and other new methods of genomic testing that may help many of us. Hopefully our MOs will be up to date on the new technologies and use them to our advantage moving forward.
-
Bev, 2006??? Are you kidding me? Science should be investigating you in and out - you are one of a kind!:) Best of luck for Friday again... Saulius
-
buttonsmachine, thanks so much for posting the excellent article about the mysteries of metastasis.
My BC recurred after 26 years. I was on Tamoxifen for 12 years or so after my initial surgery/chemo in 1991 (my initial MO just didn't want to "mess with success" and kept me on it, even though then current guidelines said 5 years only), and when my original MO retired, I changed to a supposedly preeminent MO who immediately changed me from Taxoxifen to Evista (raloxifene). I remained on raloxifene until metastasis was discovered in my bones 14 years later. Look at what I found online:
Switched from tamoxifen to raloxifene:
This means that raloxifene reduces risk of non-invasive breast cancer by about 38 percent compared to tamoxifen reducing risk for this type of cancer by about 50 percent; or raloxifene is about 78 percent as effective as tamoxifen in reducing the risk of noninvasive breast cancer over almost 7 years.Apr 19, 2010
When I changed from the preeminent MO to my current one, he replied to my question as to whether changing from tamoxifen to faloxifene might have "unleashed the beast", "Yes, it surely could have".
Thanks for the very helpful article.
-
Lynn,
Wow. I hadn't focused before on the fact that you were 26 years out when you had recurrence. That's a wild story. Saulius noted that scientists should follow me, now 16 years out from that first metastasis; likewise, they should be studying you. Your story and mine simply highlight how much science does not understand the mechanism of metastasis, especially metastasis after a long period of dormancy.
-
Bev-Jen-
Agreed. I didn't realize how far out you were, either!
And on the length of my period of dormancy, my most recent MO, head of a cancer center, said that my 26 years was his longest period of dormancy in one of his patients. I just pray that the length of that dormancy may in some fashion bode well for holding it now at bay for a while. We shall see.....
-
ctDNA in Neoadjuvant-Treated Breast Cancer Reflects Response and Survival
December 03, 2020
- The authors of this retrospective analysis evaluated circulating tumor DNA (ctDNA) levels in samples from high-risk, early-stage breast cancer patients in the neoadjuvant I-SPY 2 trial in order to correlate detection with therapeutic response and outcomes. In this analysis, ctDNA panels were informed by each patient's particular tumor genotype. The proportion of ctDNA-positive samples was significantly higher among HER2-positive (84%) and triple-negative (86%) subtypes compared with HR-positive/HER2-negative (48%) subtypes. The results indicate that clearance of ctDNA during the course of neoadjuvant chemotherapy was associated with improved survival even in patients who did not achieve pathologic complete response. Additionally, failure to clear ctDNA after neoadjuvant chemotherapy was correlated with risk of future distant metastases.
- The authors conclude that personalized ctDNA analysis can be used as a biomarker to predict therapeutic responses and outcomes for high-risk breast cancer patients.
- CONCLUSIONS: Lack of ctDNA clearance was a significant predictor of poor response and metastatic recurrence, while clearance was associated with improved survival even in patients who did not achieve pCR. Personalized monitoring of ctDNA during NAC of high-risk early breast cancer may aid in real-time assessment of treatment response and help fine-tune pCR as a surrogate endpoint of survival.
https://www.annalsofoncology.org/article/S0923-753...(20)43162-X/fulltext{free access to full article} -
2020 NCI Press Release
Postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancer that has spread to a limited number of lymph nodes, and whose recurrence risk is relatively low, do not benefit from chemotherapy when it is added to hormone therapy, according to initial results from a clinical trial presented at the 2020 San Antonio Breast Cancer SymposiumExit Disclaimer.
Some postmenopausal women with breast cancer may forgo chemotherapy
-
New Assay Platform Enhances Detection of Circulating Breast Cancer Cells
November 26, 2020
Detection of circulating tumor cells (CTCs) in a breast cancer model was improved by a novel assay platform that uses a dual-receptor recognition and signal amplification strategy, researchers say.
"Considering the urgent need for early diagnosis of metastatic breast cancer and recent advances in functional nucleic acid-mediated bioassays from our group, we designed the platform and demonstrated its feasibility for CTC detection," Dr. Zai-Sheng Wu of Fuzhou University in China told Reuters Health...
"...the newly developed...assay system is suitable for screening CTCs in complex environments and is expected to be a promising tool for estimating distant metastasis and predicting the recurrence of tumors."
Dr. Wu said, "The detection of CTCs from patients with breast cancer remains technically challenging because of their heterogeneity. Nevertheless, our group is already collaborating with scientists in Fujian Cancer Hospital to promote the transition from the laboratory to clinic trials."
The article contains discussion about methodology and shortcomings of the approach.
"The ability to detect rarer CTC populations would be helpful for risk stratification after surgery and to facilitate diagnosis or biomarker testing when there is limited tissue."
"Comparison of this technique using human blood samples from the clinic and CTC detection with this platform versus existing platforms would be a key step," he said, "then focusing on the clinical impact of more sensitive CTC detection, perhaps to determine need for adjuvant chemotherapy in certain post-operative settings."
https://www.medscape.com/viewarticle/941629?src=wn...
https://doi.org/10.1021/acssensors.0c01082
{Free access to full article.}
-
Trastuzumab Interruption Linked to Worse Outcomes in ERBB2-Positive Disease
October 22, 2020
A single-center study of trastuzumab interruption in patients with ERBB2-positive breast cancer found that dose interruption was associated with higher rates of disease recurrence and death compared with uninterrupted treatment.
Researchers from Memorial Sloan Kettering Cancer Center conducted the study because "findings from the PHARE and PERSEPHONE trials on the noninferiority of 6- vs 12-month durations of trastuzumab are conflicting, thus the clinical significance of early trastuzumab interruption on breast cancer outcomes remains uncertain."
The study included 1396 patients who had been treated with trastuzumab between 2004 and 2013. Early interruption was defined as a 6-week or longer interval between scheduled trastuzumab doses.
Findings indicated that the total dose of trastuzumab "plays an important role in breast cancer outcomes." Trastuzumab interruption with a cumulative dose of 56 mg/kg or less was associated with a reduced recurrence-free survival (adjusted HR, 1.96; 95% CI, 1.16-3.33).
"Given that most patients in this study were treated with anthracyclines, our findings may not be generalizable to patients receiving nonanthracycline treatment regimens," the researchers noted.
https://www.oncologynurseadvisor.com/home/cancer-t...
Reference: Copeland-Halperin RS, Al-Sadawi M, Patil S, et al. Early trastuzumab interruption and recurrence-free survival in ERBB2-positive breast cancer. JAMA Oncol. Published online October 15, 2020.doi:10.1001/jamaoncol.2020.4749
{Reporting and abstract available free. Subscription or $30 per article charge for full journal article.}
-
Thank you Lumpie. I do believe that giving cancer cells a "vacation time" makes them mutate and re-organize to metastasis. Sneaky disease.
-

😳 Didn’t expect this from SABCS20. Looks like I will be going back on a low carb diet. Before metastasis I lost 50 lbs on KETO. Kept off 45 and eat what I want. I will ask Dr Hamilton what she thinks on Monday.
Dee
-
AlabamaDee, thanks for posting this! More motivation for me to stick to my low carb eating plan! That was the only way I could lose any significant amount of weight post-menopause.
Some good info coming out of virtual SABCS
-
I thought low glycemic isn't the same as low carb or keto?
I gotta say don't think much of animal models anyway so I'm ambivalent about this
-
You are correct it isn't the same Moth, I would say it's more flexible.
Here is a handy chart-
-
AlabamaDee, thanks. Yes, it's good motivation to eat a low glycemic diet. It partly depends on how much you are eating and what foods you're eating together, because of how food metabolizes. My registered dietician cousin recommends I eat a diabetic's diet to maintain stable blood sugar. My weight is healthy and stable; my glucose and A1c are high-normal but basically stable. But I could do a lot better job with what I eat. sigh...
-
yes low glycemic and KETO are different. I just lived KETO for a year and know it worked for me. My A1c and glucose are fine and I have always been an overweight person. Not doing anything drastic until after Xmas.
-
yes, more flexible and, by definition, with low carb, I am eliminating most if not all of those high glycemic foods on that list. And, I would not eat some of lower glycemic carbs on a daily basis either. When I do choose a grain product or a fruit, I do consider the glycemic index.
Most people I know who do full keto are doing the same...it is pretty much automatically a low glycemic diet.
Nice chart, 2019whatayear, thanks for the link.
-
Dee, do you have a link to that article (if it was an article)? Thanks!
-
Lots of BC information in this Oncology Business Review daily. I hope that the link will open. It is possible to subscribe to this daily oncology journal.
-
Study can orient use of melatonin in the treatment of breast cancer
A Brazilian study published in the Journal of Pineal Research describes a group of genes potentially regulated by the hormone melatonin in some types of cancer, especially breast cancer. According to the authors, the results can be used to guide future personalized therapies for the disease...
As a result, they were able to understand how melatonin works in several cellular signaling pathways. "These genes targeted by melatonin relate to important biological processes in cancer, such as cell cycle regulation, cell death, and cell migration and senescence," he explained. "Melatonin appears to act more strongly on breast, oral, and stomach cancer...
According to Chuffa, genes regulated by melatonin in breast cancer are potential targets for the treatment of the disease. "Melatonin is a multitasking molecule and acts on various cellular substrates, so we're now taking the study deeper to find out how the hormone influences microRNA expression and hence the regulation of the cellular mechanisms identified," he said.
-
JoynerL
The low glycemic study was a presentation at SABCS20 that my trial doc commented on in Twitter. I can’t search the abstracts right now. Sorry. I do plan to ask her more about it on Monday
Dee
-
Wait, I just realized-- Dee, your doctor is Dr. Hamilton? She seems to be pretty awesome. I follow her on twitter.
There isn't an article to link the info was from a presentation at the San Antonio BC Symposium. There might be info here: SABCS News Or you can find some commentary from doctors and patients re. on twitter if you search the hastag #SABCS20
I'm sure more info will be coming out. The takeaway is really that a healthy diet is a low glycemic diet so the more you can follow that the better your overall health will be long term.
-
Thanks, all!
-
Re: whether common cholesterol drugs might improve the reach of immunotherapy--
https://www.cancer.gov/news-events/cancer-currents...
-
Hi!
Can anyone weigh in on the results of today's RxPonder results? I was diagnosed in 2018 premenopausal 1/4 positive nodes and a low Oncotype of 9. I sought out 3 MO opinions and they all said chemo would have little to no benefit to me so I skipped it. The results from this study seem pretty clear that was a terrible decision as the premenopausal group that received chemo plus ET had a 46%!! reduction in metastatic reoccurrence compared to the arm that did ET only. Ugh.
-
Garnersuz77: I read a summary really quickly, but the way I read it, it looked like it changed the risk by maybe 4%. Not nothing, but not huge either. And, of course, (as far as I know,) we didn't have studies before now showing this difference in prognosis. Of course, that is why we need more research. It is great to have all this "smart"/personalized medicine, but if we can't figure out the persons for whom it is smart, we don't really come out ahead. We will get there but... arg... it is to be on the long end of the wait.
-
The doctors discussing it were really leaning toward chemo not being of benefit pre or post if 1-3 nodes . They think the difference is mostly due to younger women being thrown into menopause due to chemo so the perceived benefit is more due to the sudden menopause vrs the chemo itself
With a score of 9 the endocrine therapy is what you need -Take heart!
-
Here's Dr. Kalinsky of Emory University on the subject:
-
Thank you all very much! I feel better now that I understand it better. The ovarian suppression benefit as a result of chemo vs. a large benefit from the chemo itself make a lot of sense.
-
hold your enthusiasm....
from Annals of Oncology Oct 2020
"Less than 20% (19.3%) of cancer science discoveries touted as breakthrough, landmark, groundbreaking, or highly promising translated into clinical therapy or practice with a median follow up of 15 years. Among clinically adopted treatments in our analysis, most were approved based on surrogate end points and only 9.1% found a survival benefit. Among 8 therapies with an OS benefit, the median benefit provided was 2.8 months. Our results suggest that claims of major discovery are associated only with modest rates of ultimate clinical success."
DOI:https://doi.org/10.1016/j.annonc.2020.10.484
-
MOTH
Sad report. I don’t even have to read the report to believe that. Those figures pan out in clinical trial reports and even the latest news drugs. Why do they spend so much money on a drug that only gets us OSR of about 3 months (median)
Because of the hope you are one of the few on the outlying edge of the numbers like my sister. She started on opdivo for NSCLC when it first came out and has survived with stable disease for 5 years and going strong.
If they don’t keep trying, they won’t find the right one! I’m thankful for the effort and hope the next breakthrough is the one!
Dee
-
oligometastatic peeps -
improved OS for those who had surgical resection of primary and oligomets
https://drive.google.com/file/d/18yi0zQK0L4oP5WY4T...
-
Moth,
Do you have another link for that article? I can't get it to load -- I just get the spinning wheel. Or do you have an exact title so we can find it ourselves?
Thanks
-
weird I just checked and it's working for me. It's a poster presentation ahead of publication from sabcs.
Someone tweeted a lower quality version here but it doesn't blow up nicely https://twitter.com/stage4kelly/status/13367092193...
-
Thanks. That one worked for me and I was able to blow it up a bit from twitter.
-
BevJen, there's been a google problem that includes documents. If you try again later, it might work fine.
-
Physicians Commonly Miss Adverse Events in Patients With Breast Cancer
Physicians commonly underrecognized adverse events of pain, pruritus, edema, and fatigue that patients with breast cancer experienced after radiotherapy, found a study presented at the 2020 Virtual San Antonio Breast Cancer Symposium (SABCS).
The study included 9868 patients from 29 practices in Michigan who had breast cancer and received radiotherapy after lumpectomy.
Study researchers reviewed 37,593 reports of pain, pruritus, edema, and fatigue from patient reports and compared them with the grade physicians gave the adverse events. Physicians graded adverse events using the Common Toxicity Criteria for Adverse Events (CTCAE).
Physicians were considered to underrecognize pain if they graded the severity as 0 — that is, absent — and the patient reported the severity as moderate, or if they graded the severity as 1 or lower and the patient reported the severity as severe. Pruritis and edema were considered underrecognized if physicians graded the severity as 0 and patients reported bother often or all of the time. Fatigue was considered underrecognized if physicians graded the severity as 0 and patients reported having significant fatigue most of the time or always.
Compared with White patients, Black patients had a 92% increased odds of having adverse events underrecognized (odds ratio [OR], 1.92; 95% CI, 1.65-2.23; P <.001).
Compared with patients aged 60 to 69 years, patients who were younger than 50 years had a 35% increased odds of having adverse events underrecognized (OR, 1.4).
"We need to do a better job — that's really what it is," commented SABCS Codirector Virginia Kaklamani, MD, UT Health San Antonio MD Anderson Cancer Center, Texas. "We need to conduct studies where patient-reported outcomes are being reported, and we as physicians need to listen more to our patients."
https://www.cancertherapyadvisor.com/home/news/con...
Reference: Jagsi R, Griffith KA, Vicini F, et al. Identifying patients whose symptoms are under-recognized during breast radiotherapy: comparison of patient and physician reports of toxicity in a multicenter cohort. Presented at: 2020 Virtual San Antonio Breast Cancer Symposium; December 8-11, 2020. Abstract GS3-07.
{Stunningly insightful. Many of us have complained about similar issues for years. Access to reporting is at no charge but may require log-in. Not sure about access parameters for prezo. Log in for SABCS may be required.}
-
Radiation From Wireless Devices May Cause Breast Cancer, New Study Shows
https://childrenshealthdefense.org/defender/radiation-wireless-devices-may-cause-breast-cancer/
-
Posted this on an exercise thread but I think it's worth posting here too.
Physical activity of any intensity, whether folding laundry or jogging, can lower the risk of an early death for middle-aged and older people, a new study suggests. Furthermore, the time of day you move your body could affect risk further.
Researchers analyzed data from 2,795 participants. They identified a group of 781 women with breast
cancer and 865 female controls, and a group of 504 men with prostate cancer and 645 male controls. Both groups responded to a questionnaire relating to their physical activities and gave data on the timing and frequency of their exercises.
The study found that exercising in the morning, between 8-10 a.m., showed the highest benefit in reducing the risk of both breast and prostate cancers. Researchers also found that men who exercised between the hours of 7 and 10 p.m. had a 25 percent lower risk of developing prostate cancer. No benefits from evening activity were seen in the group of women.
"Overall our findings indicate that time of the day of physical activity is an important aspect of physical activity that may potentiate the protective effect of physical activity on cancer risk," the researchers wrote. "The effect of timing of physical activity on cancer risk should be examined in future research with a more detailed assessment of activity patterns, also including occupational activity."
https://onlinelibrary.wiley.com/doi/10.1002/ijc.33310 -
Complementing the post above is a study in Kenya advocating the benefits of exercise and diet in lowering the risk of BC
-
Interesting BlueGIrl.
-
this is interesting, it's from a Phase 2b Trial.
https://www.onclive.com/view/gp2-gm-csf-combo-elic...
The GP2 immunotherapy plus granulocyte-macrophage colony-stimulating factor demonstrated potent responses and a 100% disease-free survival in patients with HER2/neu 3–positive disease who received adjuvant trastuzumab.
Says there's a Phase 3 Trial Coming
-
Alpha-TEA [in phase 1 trial] strikes down advanced breast cancer?
..."The patients with HER2 driven or positive breast cancer, they actually start losing these T-cells and so they lose that immunologic response," explained William Gwin, MD, an assistant professor at University of Washington School of Medicine and breast cancer specialist at Seattle Cancer Care Alliance.
But now a phase one clinical trial is underway with advanced HER2 positive breast cancer patients for the oral therapy alpha-TEA in combination with the antibody-drug Herceptin. Alpha-TEA works by activating T-cells.
"We can boost those and drive those T-cells that target HER2 and sort of restore that immune response against HER2," elaborated Dr. Gwin.
Attacking cancer cells but leaving the normal cells alone.
"It does seem to have similar effects to chemotherapy, but really without the side effects," Dr. Gwin shared.
https://www.wmcactionnews5.com/2020/12/15/best-life-alpha-tea-strikes-down-advanced-breast-cancer/
-
Dear Debbew, this is crazily good news...
It is interesting what dosages they use (they do not say this in clinical trial)? I already found they use up to 1500 mg/kg/day in dogs:) Saulius -
-
Thanks for adding that info, Saulius!
-
HER2 people, FDA approves Margetuximab!
https://www.onclive.com/view/fda-approves-margetux...
Debbew, I tried to look if one can buy alpha-TEA:) No luck - probably a serious agent, although well known for at least a decade. Actually my motivation is based on assumption that this is something "promising", as they never had clinical trials with alpha-TEA in BC patients, and now start directly with ABC (well, there's evidence in dishes with cell lines). And it is strange this substance is not widely out there, as it is a derivative of vitE. I surely can find folks who could synthesize it here in labs:)) but it would be idiotic to use it without quality control. Trastuzumab resistance is real and it would be so cool to overcome it with this "simple" compound...
Saulius
-
-
Systemic Therapy for Estrogen Receptor–Positive, HER2-Negative Breast Cancer.
Harold J. Burstein, M.D., Ph.D.
Some of the txt:
In recent years, the options for adjuvant endocrine treatment have broadened beyond tamoxifen. Aromatase inhibitors block the conversion of androgens into estrogens (Figure 1), suppressing residual estrogen levels by more than 90% in postmenopausal women. These agents are contraindicated in premenopausal women who are not undergoing ovarian suppression, because compensatory physiological responses induce ovarian estrogen production. Aromatase inhibitor therapy results in a greater reduction in the risk of recurrence than 5 years of tamoxifen, such that most postmenopausal women should consider aromatase inhibitor treatment either as initial therapy or after 2 to 3 years of tamoxifen. For women presenting with stage I or IIA cancers — the most common stage at diagnosis in countries where screening mammography is routine — the numerical advantage of aromatase inhibitor–based treatment over tamoxifen alone is modest: a 3% reduction in recurrence and a 2% reduction in mortality at 10 years. Aromatase inhibitors are of more value in the treatment of higher-risk cancers (according to stage or biologic features) because of the underlying prognosis39 and in the treatment of lobular cancers. Extending the duration of treatment from 5 to 10 years with either tamoxifen41 or aromatase inhibitors reduces the risk of recurrence, as compared with just 5 years of treatment. Patients at increased risk for a late recurrence because of nodal status or adverse biologic features of the tumor probably derive the greatest benefit from extended therapy; however, extended aromatase inhibitor treatment in years 8 through 10 is likely to confer a modest benefit, at most. The decision to extend therapy should incorporate the patient's preferences, informed by the estimated risk of recurrence beyond year 5, and the toxic effects of therapy to date (Figures 3 and Figure 4).
-
How about this?
Nanoparticle Trains Immune Cells to Attack Cancer
-
Cleveland Clinic [triple negative] Breast Cancer Vaccine Goes To Clinical Trials
The shot protects against alpha-lactalbumin, a protein in women's mammary glands that no longer appears after childbearing years but shows up in many cases of triple negative breast cancer, [Dr. Vincent Tuohy, a cancer researcher at the clinic who invented the vaccine] said.
The idea behind taking this vaccine is the body's immune response would destroy cancer cells before they develop and mature, Tuohy said...
In animal trials, the vaccine was shown to be very effective, Tuohy added...
If the trials are successful, Tuohy said he hopes people could eventually get the vaccine as part of their normal preventative care.
-
Interesting article from the National Cancer Institute about exceptional responders --what they've found out so far.
https://www.cancer.gov/news-events/press-releases/...
-
I have stage one and had a lumpectomy and just finished radiation. Does anyone know The name of the blood test that shows how many circulating tumor cells are in a persons blood? And is it possible to get that number down to 0? And if it gets down to 0 can aperson stop taking whatever inhibitor they are taking? Just wondering if anybody has had experience with this. Thank you.
-
Springdaisy - Signatera is one brand of the CTC test. AFAIK we don't have enough studies to show if 0 means you can go off hormone therapy.
Breast Cancer Index measures risk of recurrence but it's for AFTER 5 yrs of hormone therapy to see if hormone therapy should be extended. It's not FDA approved. https://www.breastcancer.org/symptoms/testing/type...
-
moth, thank you for the info. How could you have stage four if you only had stage one three years ago? My god that’s scary.
-
Hi Springdaisy - I guess I drew the short straw. When I ran the stats in Predict https://breast.predict.nhs.uk/tool 89% of women with my stats were alive at 5 years. I used that as a proxy for metastatic recurrence... so 1/10 like me would recur with terminal disease. Tried to do my best to lessen the risk - the only evidence based interventions seem to be exercise and maybe green tea. I did that. I exercised before I got stage 1 too so didn't work then either. Didn't work to prevent progression so I guess there's some powerful cancer genetics at work & I got to be one out of 10
triple neg has a different mets timeline than hormone positive. We're more likely to recur at all but if we do, it's in the first 5 years so if we make it past 5, the risk starts falling. Hormone positive has this long tail of ongoing risk so a different risk profile. This cancer thing sucks all around & part of what's missing in breast cancer discussions is that it still kills very many of us. So much talk of 'survivors' and pink ribbons that sometimes it's easy to forget it's fatal to many.
-
thank you for replying, moth. I wish you and everybody in this forum the best of luck. Yes, you are right, cancer sucks no matter what kind. Someone brought up the point the other day that they have rushed through the Covid vaccine so what about rushing through cures for cancer and other things? I never thought of it before but that’s a very good point. Although I don’t want cures that have been rushed through the system but they claim Covid was tested upon thousands of people and went by the rules of the CDC.
-
The trouble is cancer is not a disease any more than "virus" is a disease. Even within breast cancer effective treatments are radically different for all the different subtypes. So there will never be one cure for "cancer" any more than there will be one cure for all viruses, from cold viruses to polio to HIV.
I just finished a year and a half of chemo, which brings my 3 year "risk" of disease-free survival to 89% Improved, but not great.
My oncologist is very honest with me, "the only way to know you are a survivor is to die of something else" Breast cancers suck.
-
Anyone heard about this? Sounds great, I love to see a bigger trial group though.
https://www.targetedonc.com/view/fda-grants-fast-track-designation-for-her2-positive-metastatic-breast-cancer“A clinical update on ARX788 was announced in December during a presentation for the 2020 San Antonio Breast Cancer Symposium (SABCS) demonstrated an objective response rate (ORR) of 74% with ARX788 in the phase 1 HER2-positive breast cancer trial in China, which included responses in 14 of 19 patients and a disease control rate (DCR) of 100%. The ORR was 67% in the phase 1 HER2-positive pan tumor trial in the United States and Australia with responses in 2 of 3 patients and a DCR of 100%. Both these findings were found with the 1.5 mg/kg dose.2“
-
Preliminary study of how adiposity influences breast cancer biology, treatment resistance, and disease progression shows High BMI related to effectiveness of doxataxel!
This is a surprise revelation and shocking to me, 😳 Since my BMI was much higher when I was on taxotere. Hope they study this more.Dee
-
seems like the evidence so far is pointing to higher BMI = less taxane effectiveness
Well, I was in the high overweight BMI when I did Taxol and I had a great response, then again I was also on Herceptin and Perjeta so maybe that matters.
This definitely needs further study.
-
This is interesting:
-
Lumpie, How're you doing? We who appreciate this thread thank you and wish you a happy new year!
-
Hi santabarbarian! I am ok, thank you for checking....and I am very glad that you and others appreciate the topic/board. I have a couple of things I need to post. The new-ish med I am on is doing a job on my digestive system and I feel like I am always behind/moving in slow motion. Hope you are well and.... at this point, I am almost reluctant to speculate about how the year might ging.... but hope you ... and eveyone else, too!.... have a healthy and happy new year!
-
I say thank you too. This is the thread I check on nearly every day. Often the only one I check. I appreciate the work it takes to aggregate this information.
-
Me too - Thanks Lumpie.
-
Lumpie,
I hope you’re feeling better. I wanted to chime in and agree with the rest of the group that I definitely appreciate all the effort you put into this topic. Thank you
-
Yes. Thank you, Lumpie!
-
Me, too, Lumpie...thanks so very much! A much-needed forum!
-
Thank you for the post on gut health. We are complex animals and many things seemed to get overlooked, dismissed, or are poorly understood. The bacdterium mentioined, Bacteroides fragilis, normally in the colon wrecks havoc elsewhere, unsurprisingly. But does it escape unnoticed? Lifestyle is so important. Is kimchi, sour kraut, yogurt etc enough for a healthy gut?
-
-
Thank you Lumpie for your tending of this post! I too sometimes come to the site just to read the latest updates on this post
-
Adding my voice to the choir thanking Lumpie. I also follow this thread closely.
-
NCI aims to track BC recurrenceSharing this - long overdue -
-
As always Lumpie, you know we appreciate you! And also the growing group of folk who regularly post here...you’ve inspired them!
-
I will add my thanks Lumpie. I check this thread at least once a day!
-
Thank you Lumpie!
-
t Lumpie- glad to “see” you - we missed you while you were out recuperating .
Recommended treatment graph for metastaticDee
-
thanks Lumpie and all who contribute. That flow chart for metastatic BC was very interesting thanks Dee.
-
Thank you so much, everyone, for your kind and encouraging comments! You have made my week and I truly appreciate it.
-Lumpie
-
Shorter radiotherapy promising in breast cancer
Women with early invasive breast cancer who underwent one-week high- or low-dose hypofractionated adjuvant whole-breast radiotherapy regimen had similar five-year ipsilateral breast tumor relapse rates and safety outcomes, compared with those who received the standard three-week regimen, according to a study presented at the European Society for Radiology and Oncology 2020 Online Congress and published in The Lancet. The findings suggest the safety and efficacy of hypofractionated radiotherapy regimen as the new standard for early invasive breast cancer, said researcher Joanne Haviland.
https://www.mdedge.com/hematology-oncology/article...
https://www.thelancet.com/journals/lancet/article/...(20)30932-6/fulltext
DOI:https://doi.org/10.1016/S0140-6736(20)30932-6
{Report courtesy of AANP Smart Brief; Lancet article appears to be available w/o charge.}
-
COVID-19 Vaccine & Patients with Cancer
ASCO commentary on the covid-19 vaccine for cancer patients.
In short...
Are there people who should not be vaccinated?
At this time, only those with contraindications to a specific vaccine component should not be offered vaccination with that specific product. These contraindications are described in detail on the CDC's vaccination clinical considerations page.
... patients undergoing treatment may be offered vaccination against COVID-19 as long as any components of the vaccine are not contraindicated.
https://www.asco.org/asco-coronavirus-resources/co...
{I believe that this page is publicly available. If not, let me know and I can post details.}
-
Older women with early breast cancer may be able to avoid radiation after surgery
The omission of radiation therapy after breast-conserving surgery did not affect survival among certain older women with early breast cancer, according to results presented at the virtual San Antonio Breast Cancer Symposium.
Radiation therapy reduced the rate of ipsilateral breast tumor recurrence among women aged 65 years or older with hormone receptor-positive disease who underwent wide local excision and were receiving adjuvant hormonal therapy.
However, radiation therapy receipt did not affect rates of distant metastases, contralateral breast cancer or OS, 10-year data from the randomized phase 3 PRIME II trial showed.
https://www.healio.com/news/hematology-oncology/20...
Source: Kunkler IH, et al. Abstract GS2-03. Presented at: San Antonio Breast Cancer Symposium (virtual meeting); Dec. 8-11, 2020.
{Access to coverage should be free of charge. Registration may be required.}
-
Symptoms often underrecognized among patients receiving radiotherapy for breast cancer
Symptoms such as pain, fatigue and pruritus often went underrecognized among patients with breast cancer treated with radiotherapy, according to study results presented at the virtual San Antonio Breast Cancer Symposium.
Black patients and younger patients appeared at significantly higher risk for symptom underrecognition, results showed.
"We were disappointed to find that physicians frequently didn't recognize the severity of the symptoms patients themselves reported they were experiencing," Reshma Jagsi, MD, DPhil, Newman family professor and deputy chair of the department of radiation oncology and director of Center for Bioethics and Social Sciences in Medicine at University of Michigan, told Healio.
"Because physicians cannot help patients if they don't know who is suffering, improving symptom detection appears to be a way to improve the quality of care and to reduce disparities in cancer treatment experiences and outcomes," Jagsi added. "The findings also suggest that clinical trials should not rely on physician reports alone to evaluate the side effects of treatments; patient-reported outcomes provide an important complement to physician evaluations."
https://www.healio.com/news/hematology-oncology/20...
Source: Jagsi R, et al. Abstract GS3-07. Presented at: San Antonio Breast Cancer Symposium (virtual meeting); Dec. 8-11, 2020.
{Access to coverage should be free of charge. Registration may be required.}
-
LilyisHere.. This is the study my MO told me about. I am currently in year 7 with the end being this December. She and I agreed to extending two years instead of 5 with us discussing it at the end of 7. Reading your link I fall into the high ER and low grade tumors giving me an "excellent prognosis" which would explain the positive attitudes of all my doctors. I'm debating whether to continue to year 10. I wonder if there is any place you can see just how toxic the AI's are. That would help in my decision. Has anyone seen this ?
-
HHS Tells States to Open Vaccine Access to Vulnerable Adults
— Given healthy vaccine supply, second doses will no longer be withheld, says HHS Secretary
January 12, 2021
...Azar said it was time to broaden the scope of eligible recipients, and to expand the number and type of delivery sites. He outlined the administration's plans to carry out the following actions:
- Direct states to expand the populations eligible to receive COVID vaccine doses to those ages ≥65 and those ages <65 with comorbidities as validated by medical documentation (the latter will be determined by state governors)
Azar outlined the reallocation of vaccine doses to those states that are most effective in administering them, based on self-report, and to those states with the greatest numbers of adults who are over age 65. In 2 weeks, allocations will no longer be determined simply by a state's population but by the percentage of vaccines administered compared to the allocation a state received, he explained.https://www.medpagetoday.com/infectiousdisease/cov...
-
Lumpie,
Thanks for posting. I just wrote to our governor and our county executive about this (I live in Maryland) -- so far they are sticking to their guns about the original distribution schedule. Hope this changes.
-
After 48 Years, NCI Aims to Track Breast Cancer Recurrences
Change to SEER Eventually Planned
January 08, 2021
Patients with breast cancer want accurate information on the risk of their cancer recurring once they have completed treatment.
But those statistics have not been available from a robust population-based source.
Now, there is hope that they will ― at last ― be collected.
A new pilot project at the National Cancer Institute (NCI) is setting out to collect that information, although the researchers say it is a "long-term goal" that will take a few years.
But it has already been a long time coming. The mother lode of all US cancer data, the NCI's Surveillance, Epidemiology, and End Results (SEER) Program, started collecting cancer data in 1973.
{The SEER} database has never included information on cancer recurrence.
The NCI now has a "long-term goal" to implement additional "data elements" into SEER that will allow calculation of breast cancer recurrences...
Breast cancer advocates have long been calling for SEER to count recurrence, including metastatic recurrence.
https://www.medscape.com/viewarticle/943796?fbclid...
{Free access to reporting. Registration may be required.}
-
Lumpie - thank you for posting NCI starting to track/examine recurrence probability. Increadible that this is not being done. It seems like it could really influence treatment. I've been told that even if tumor from time 1 to time X were compared, cancer mutates so much, that it might be difficult to know if it is recurrence, a new cancer, or maybe even if the original cancer was not irradicated the first time. I wonder to if monitoring would be more rigorous and able to catch cancer recurrence/new cancer sooner.
-
Have you seen this? A clinical trial with your own MO.
Thanks Christine Hodgdon at https://thestormriders.org/ for posting this on Twitter
If you have the SF3B1 mutation, you may be eligible for the PRISMM trial which allows you to receive immunotherapy at your local cancer clinic without ever having to travel! https://clinicaltrials.gov/ct2/show/NCT04447651
Dee -
from JAMA an editorial on reducing recurrence in early TN
-
Stereotactic Ablative Body Radiotherapy in Patients With Oligometastatic Cancers
- The Lancet Oncology, January 07, 2021 The authors of this prospective National Health Service registry–based observational study evaluated the outcomes of 1422 patients with solid cancer extracranial oligometastatic disease treated with stereotactic ablative body radiotherapy. The 1- and 2-year overall survival rates were 92% and 79%, respectively. Grade 3/4 toxicity was rare.These real-world findings support both earlier trial data and this therapeutic approach in the selected patient population.
https://www.thelancet.com/journals/lanonc/article/...(20)30537-4/fulltext{Free access to reporting and abstract. Full article requires fee or subscription.} -
Oncotype DX Misses on Breast Cancer Risk in Black Women
— Accuracy of 21-gene recurrence score worse compared with white women
https://www.medpagetoday.com/hematologyoncology/breastcancer/90813
-
Efficacy of Margetuximab vs Trastuzumab in Patients With Pretreated ERBB2-Positive Advanced Breast Cancer -- A Phase 3 Randomized Clinical Trial
JAMA Oncol. Published online January 22, 2021
Results A total of 536 patients were randomized to receive margetuximab (n = 266) or trastuzumab (n = 270). The median age was 56 (27-86) years; 266 (100%) women were in the margetuximab group, while 267 (98.9%) women were in the trastuzumab group. Groups were balanced. All but 1 patient had received prior pertuzumab, and 489 (91.2%) had received prior ado-trastuzumab emtansine. Margetuximabhttps://jamanetwork.com/journals/jamaoncology/full...improved primary PFS over trastuzumab with 24% relative risk reduction (hazard ratio [HR], 0.76; 95% CI, 0.59-0.98; P = .03; median, 5.8 [95% CI, 5.5-7.0] months vs 4.9 [95% CI, 4.2-5.6] months; October 10, 2018). After the second planned interim analysis of 270 deaths, median OS was 21.6 months with margetuximab vs 19.8 months with trastuzumab (HR, 0.89; 95% CI, 0.69-1.13; P = .33; September 10, 2019), and investigator-assessed PFS showed 29% relative risk reduction favoring margetuximab (HR, 0.71; 95% CI, 0.58-0.86; P < .001; median, 5.7 vs 4.4 months; September 10, 2019). Margetuximab improved objective response rate over trastuzumab: 22% vs 16% (P = .06; October 10, 2018), and 25% vs 14% (P < .001; September 10, 2019). Incidence of infusion-related reactions, mostly in cycle 1, was higher with margetuximab (35 [13.3%] vs 9 [3.4%]); otherwise, safety was comparable.Conclusions and Relevance In this phase 3 randomized clinical trial, margetuximab plus chemotherapy had acceptable safety and a statistically significant improvement in PFS compared with trastuzumab plus chemotherapy in ERBB2-positive ABC after progression on 2 or more prior anti-ERBB2 therapies. Final OS analysis is expected in 2021.Trial Registration ClinicalTrials.gov Identifier: NCT02492711https://jamanetwork.com/journals/jamaoncology/full...
doi:10.1001/jamaoncol.2020.7932
{appears to be open access} -
Aspirin linked to better survival rates for bladder and breast cancer
https://www1.racgp.org.au/newsgp/clinical/aspirin-associated-with-better-survival-rates-for
-
Unexpected Survival Benefit Reported With Trilaciclib in Metastatic Triple-Negative Breast Cancer https://ascopost.com/issues/january-25-2021/unexpe...
key points:
phase 2 trial reporting
pts were pre-treated
trilaciclib is an IV cdk4/6 inhibitor
was given w. gemcitabine plus carboplatin
"The outcome in the PD-L1–positive subset (57.6% of those tested) was notable, with overall survival of 32.7 months vs 10.5 (hazard ratio = 0.34; P = .004)."
"We plan to initiate a registrational trial for trilaciclib in mTNBC in 2021, with overall survival as the primary outcome measure"
More from the manufacturer here: https://www.g1therapeutics.com/pipeline/trilacicli...
-
Large studies estimate breast cancer risk linked to specific genes
January 20, 2021
Two large studies published in the New England Journal of Medicine found pathogenic variants in BRCA1 or BRCA2 genes raise the carrier's risk for breast cancer by nearly eightfold or more than fivefold, respectively, and protein-truncating variants in BRCA1 was linked to a tenfold higher risk. Moderate breast cancer risk was also associated with mutations in PALB2, ARD1, RAD51C, RAD51D, ATM and CHEK2 genes, and specific genes were linked to risks for specific types of breast cancer.
CONCLUSIONS
This study provides estimates of the prevalence and risk of breast cancer associated with pathogenic variants in known breast cancer–predisposition genes in the U.S. population. These estimates can inform cancer testing and screening and improve clinical management strategies for women in the general population with inherited pathogenic variants in these genes. (Funded by the National Institutes of Health and the Breast Cancer Research Foundation.)
Reporting courtesy of AANP SmartBrief
https://www.medpagetoday.com/hematologyoncology/br...
https://apnews.com/article/us-news-genetics-cancer...
https://www.nejm.org/doi/full/10.1056/nejmoa200593...
DOI: 10.1056/NEJMoa2005936
{Coverage free of charge but may require registration; abstract w/o charge. Access to full article in NEJM requires fee or subscription.}
-
Breast cancer: Androgen therapy shows promise in preliminary study
Scientists have embarked on renewed investigations into androgen therapy — a former breast cancer treatment. Recent research in mice shows that it may help block tumor growth.
....
Androgen therapy was practiced during the first half of the 20th century, according to a paper published in the American Journal of Cancer Research. Doctors stopped using it for breast cancer, though, when scientists determined that "Androgens can be converted to estrogens."
This led researchers to believe that androgen therapy could do more harm than good, since an increase in estrogen is linked with breast cancer.
However, in a recent study published in Nature Medicine, researchers decided to take another look at this use of androgens. The team discovered that this hormone may, after all, contribute to fighting breast cancer.
The researchers — many from the University of Adelaide, in Australia — studied the effect of androgen receptor-activating drugs on cell cultures and mouse models of breast cancer. In these mice, the scientists had implanted tumors extracted from patients with breast cancer.
They found that activating androgen receptors had a "potent" suppressive effect on different kinds of breast cancer tumors, even those that had been resistent to "traditional" treaments with estrogen receptor inhibitors and CDK4/6 inhibitors.
-
Signatures of Mutational Processes and Response to Neoadjuvant Chemotherapy in Breast Cancer
- The authors of this retrospective analysis performed whole-exome sequencing on retreatment tumor samples in patients with previously treated, primary invasive HER2 negative breast cancer to evaluate the mutational signals which may be predictive of tumor response and resistance to neoadjuvant chemotherapy. Different breast cancer subgroups could be identified by differences in homologous recombination deficiency (HRD)–associated APOBEC-related mutations. For HR-positive tumors, the mutational signal S13 showed a strong correlation with an increased pathological complete response (pCR) rate while the S3 signal for HRD was borderline significant. Tumors with a high S13 signal had a median pCR of 22% versus 4% in tumors with low S13 levels. HR-positive tumors were noted to have signatures S3 and S4 associated with reduced disease-free survival, but these were nonsignificant in multivariate analysis. In contrast, HR-negative tumors had no mutational signatures associated with pCR.
- Whole-exome sequencing revealed that the clinical behavior of particular tumor types could be predicted by the mutational signatures. This requires validation and confirmation of relevant mutational signatures but may help to identify tumor types more rapidly responsive to neoadjuvant chemotherapy to inform treatment decisions.
{Free access to reporting and abstract. Full article requires subscription or fee.} -
There is an interesting Freakonomics Radio podcast called "How to fix the incentives in cancer research".
It focuses a bit on prostate cancer, but also gives general insight on cancer trials challenges and improving approaches.
-
NCCN Shares New Guidance Principles for Vaccinating People with Cancer Against COVID-19
The committee's recommendations state that all people currently in active cancer treatment should get the vaccine, with some advice to consider regarding immunosuppression and timing. The full document can be found at NCCN.org/covid-19, along with other vital information about the impact of COVID-19 on cancer care.
The guidance acknowledges that although these vaccines have been shown to be safe in general populations, their effectiveness among cancer and transplant patients is not precisely known at present.
The panel will continue to meet regularly in order to refine the recommendations for these and other issues, as they come up.
https://www.nccn.org/about/news/newsinfo.aspx?News...
-
Individualizing Surveillance Mammography for Older Patients After Treatment for Early-Stage Breast Cancer
Multidisciplinary Expert Panel and International Society of Geriatric Oncology Consensus Statement
January 28, 2021The first mammography guidelines for older survivors of breast cancer emphasize decision-making based on life expectancy.Conclusions and RelevanceIt is anticipated that these expert guidelines will enhance clinical practice by providing a framework for individualized discussions, facilitating shared decision-making regarding surveillance mammography for breast cancer survivors 75 years or older.doi:10.1001/jamaoncol.2020.7582{Abstract free, fee or subscription for full access.} -
Breast cancer now most common type of cancer
A World Health Organization report found that breast cancer, which has overtaken lung cancer as the most common type, accounted for 11.7% of new cases across the world last year. Obesity was a common risk factor for breast cancer among women, while high body mass index, tobacco and alcohol use, lack of physical activity, and low intake of fruits and vegetables contributed to nearly one-third of cancer deaths, according to the report.
https://www.reuters.com/article/health-cancer/brea...
{Free access to reporting. Summary courtesy of AANP.}
-
The Genomic Landscape of Breast Cancer Brain Metastases
January 17, 2021 - The Lancet Oncology
- The authors of this systematic review of 164 patients from 13 studies evaluated the genomic landscape in breast cancer brain metastases. There were 268 mutated genes present in at least two samples and 22 of these were mutated in five or more samples. Pathway enrichment analysis demonstrated the involvement of these genes in breast cancer–related signaling pathways, regulation of gene transcription, cell cycle, and DNA repair. Of the 22 mutations, 15 were shown to be actionable drug targets. There was receptor discordance between the primary breast cancers and the brain metastases.
- When possible, brain metastasis samples should be obtained to guide targeted therapy.
https://www.thelancet.com/journals/lanonc/article/...(20)30556-8/fulltext{Free access to reporting and abstract. Fee or subscription for whole article.} -
this is not a specific study but I saw this and found it interesting that some studies are based off of false assumptions. Including a number of breast cancer studies.
”As an example of outdated science keeping its momentum, Pielke writes of a 2015 literature review of some 900 peer-reviewed studies on breast cancer using a cell line "derived from a breast cancer patient in Texas in 1976." But in 2007, he says, it was confirmed that it was a skin cancer line, not one related to breast cancer, and that even now it is being improperly used in breast cancer research“
-
Wow. Guess it's trust but verify territory!
-
for an article on the issue of breast cancer cell lines, which also discusses the MDA-MB-435 cells referred to above (controversial, but probably melanoma lines), see this article in Breast Cancer Research
https://breast-cancer-research.biomedcentral.com/a...
From a stage 4 pt perspective I find in vitro studies pretty useless as they're not going to yield clinical results quickly but from a theoretical perspective, they are a source of fascinating insight into what causes mutations and how we might affect them.
-
There was a book written in the 1980s about the Henrietta Lacks cell line and cell line contamination and how it was covered up by scientists. The title is “A Conspiracy of Cells”
Also - https://pubmed.ncbi.nlm.nih.gov/19722756/
And https://www.discovermagazine.com/health/the-dirty-little-secret-of-cancer-research
-
Surgery Could Boost Survival for Women With Advanced Breast Cancers: Study
Women with advanced breast cancer who undergo surgery to remove the tumor after chemotherapy or another type of systemic treatment may live longer than those who don't have surgery, a new study suggests.
The findings challenge a long-held belief that surgery confers little benefit for women with stage 4 breast cancer unless the cancer is causing pain, bleeding or other symptoms.
https://consumer.healthday.com/12-30-surgery-could...
SOURCES: Daleela Dodge, MD, associate professor, surgery, Penn State Cancer Institute, Hershey, Pa.; Stephanie Bernik, MD, chief, breast service, Mount Sinai West Medical Center, New York City, and associate professor, surgery, Icahn School of Medicine at Mount Sinai, New York City; Annals of Surgical Oncology, Oct. 30, 2020
(Reporting is free to access. Not sure about journal article.}
-
Primary Trastuzumab-Resistance After (Neo)Adjuvant Trastuzumab-Containing Treatment for HER2-Positive Breast Cancer Patients
- In this retrospective study of 1096 patients with HER2-positive early-stage breast cancer who received (neo)adjuvant trastuzumab, the authors evaluated primary trastuzumab resistance outcomes, defined as a recurrence during or within 12 months of therapy. Among a total of 126 recurrences, 75 met the definition of primary trastuzumab resistance, which was associated with a worse prognosis and a lower response rate to subsequent trastuzumab-containing therapy.
- Primary trastuzumab resistance was associated with a poor prognosis, and further research is warranted to evaluate the optimal treatment strategy for these patients.
https://www.clinical-breast-cancer.com/article/S15...(20)30218-4/fulltext{Free access to reporting; fee or subscription for full article.} -
FDA Approves MARGENZA™
On December 16, 2020, the FDA approved margetuximab-cmkb (MARGENZA™, MacroGenics) in combination with chemotherapy, for the treatment of patients with metastatic HER2-positive breast cancer who have received two or more prior anti-HER2 regimens, at least one of which was for metastatic disease. This new approval is based on the SOPHIA trial.
FDA Approves Margetuximab for Metastatic HER2-Positive Breast Cancer
FDA Approves Margenza Plus Chemotherapy for Pretreated Metastatic HER2-Positive Breast Cancer
-
Breast Cancer Brain Metastases: Clinical Challenges and Recent Advancements
At SABCS 2020, investigators shared current research findings and moreBy BCRF - January 5, 2021Researchers are addressing clinical challenges and exploring the biology of brain metastases to develop novel treatment strategies and combat this devastating occurrence.At this year's San Antonio Breast Cancer Symposium (SABCS), researchers gave an overview of the treatment landscape for patients with breast cancer brain metastases (BCBM) and highlighted some promising new areas for future research.https://www.bcrf.org/sabcs-2020-updates-on-breast-...
{Excellent and brief summary of latest research on BCBM. Free access to this reporting.} ...and a journal article.... Evolving treatment strategies of brain metastases from breast cancer: current status and future directionTher Adv Med Oncol. 2020; 12: 1758835920936117.Published online 2020 Jun 23. doi: 10.1177/1758835920936117Remarkable progress in breast cancer treatment has improved patient survival, resulting in an increased incidence of brain metastasis (BM). Current treatment options for BM are limited and are generally used for palliative purposes. Historically, local treatment, consisting of radiotherapy and surgery, is the standard of care due to delivery limitations of systemic treatments through the blood–brain barrier. However, as novel biological mechanisms for tumors and BM have been discovered, several innovative systemic agents, such as small-molecular-targeted therapy and immunotherapy, have begun to change the treatment paradigm. In addition, efforts to maximize antitumor effects have been attempted using combination therapy, informed by tumor biology. In this comprehensive review, we will highlight various clinical trials investigating the treatment of BM in breast cancer patients, discuss presently available treatment options, and suggest potential directions of future therapeutic targets.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC73133...
(Free access to full article!} -
Safety, tolerability, and pharmacokinetics of BAT8001 in patients with HER2-positive breast cancer: An open-label, dose-escalation, phase I study.
The introductions of anti- human epidermal growth factor receptor-2 (HER2) agents have significantly improved the treatment outcome of patients with HER2-positive breast cancer. BAT8001 is a novel antibody-drug conjugate targeting human epidermal growth factor receptor-2 (HER2)-expressing cells composed of a trastuzumab biosimilar linked to the drug-linker Batansine. This dose-escalation, phase I study was designed to assess the safety, tolerability, pharmacokinetics, and preliminary anti-tumor activity of BAT8001 in patients with HER2-positive locally advanced or metastatic breast cancer. This trial was conducted in subjects with histologically confirmed HER2-positive breast cancer (having evaluable lesions and an Eastern Cooperative Oncology Group performance status of 0 or 1) using a 3 + 3 design of escalating BAT8001 doses. Patients received BAT8001 intravenously in a 21-day cycle, with dose escalation in 5 cohorts: 1.2, 2.4, 3.6, 4.8, and 6.0 mg/kg. The primary objective was to evaluate the safety and tolerability of BAT8001. Preliminary activity of BAT8001 was also assessed as a secondary objective. Between March 2017 to May 2018, 29 HER2-positive breast cancer patients were enrolled. The observed dose-limiting toxicities were grade 4 thrombocytopenia and grade 3 elevated transaminase. The maximum tolerated dose was determined to be 3.6 mg/kg. Grade 3 or greater adverse events (AEs) occurred in 14 (48.3%) of 29 patients, including thrombocytopenia in 12 (41.4%) patients, aspartate aminotransferase increased in 4 (13.8%) patients, γ-glutamyl transferase increased in 2 (6.9%) patients, alanine aminotransferase increased in 2 (6.9%) patients, diarrhea in 2 (6.9%) patients. Objective response was observed in 12 (41.4%; 95% confidence interval [CI] = 23.5%-61.1%) and disease control (including patients achieving objective response and stable disease) was observed in 24 (82.8%; 95% CI = 64.2%-94.2%) patients. BAT8001 demonstrated favorable safety profiles, with promising anti-tumor activity in patients with HER2-positive locally advanced or metastatic breast cancer. BAT8001 has the potential to provide a new therapeutic option in patients with metastatic HER2-positive breast cancer.
First published: 02 February 2021
Relevant trial: ClinicalTrials.gov (NCT04189211)
https://www.meta.org/papers/safety-tolerability-an...
https://onlinelibrary.wiley.com/doi/10.1002/cac2.1...
{Free access to abstract. Registration may be required. Free access to full article.}
-
Fecal matter transplants could help certain cancer drugs work in more people, study shows
Checkpoint inhibitors like Keytruda and Opdivo can be incredibly powerful cancer-killing drugs — when they work, that is, which is less than 70% of the time. For years, scientists have hoped to find a way to identify a combination of therapies that might help these drugs work for a larger number of people.
New clinical trial results published Thursday in Science provide some of the strongest evidence yet for an unusual but promising mashup: pairing immunotherapy drugs with fecal microbiota transplants, or FMTs.
https://www.statnews.com/2021/02/04/fecal-matter-t...
New fecal microbiota for cancer patients
The composition of the gut microbiome influences the response of cancer patients to immunotherapies. Baruch et al. and Davar et al. report first-in-human clinical trials to test whether fecal microbiota transplantation (FMT) can affect how metastatic melanoma patients respond to anti–PD-1 immunotherapy (see the Perspective by Woelk and Snyder). Both studies observed evidence of clinical benefit in a subset of treated patients. This included increased abundance of taxa previously shown to be associated with response to anti–PD-1, increased CD8+ T cell activation, and decreased frequency of interleukin-8–expressing myeloid cells, which are involved in immunosuppression. These studies provide proof-of-concept evidence for the ability of FMT to affect immunotherapy response in cancer patients.
Science, this issue p. 602, p. 595; see also p. 573 Science 05 Feb 2021: Vol. 371, Issue 6529, pp. 602-609
https://science.sciencemag.org/content/371/6529/60...
DOI: 10.1126/science.abb5920
{Fee for full articles. The topic was just too ... verboten... to pass up.}
-
If it works, it works right? Facinating!
-
Lumpie - thank you for the post on fecal matter, one more question to ask the DR. But it sounds so new, it is unlikely she would know much about it, also sounds like it might be drug/cancer specific. Gut health seems to be another area of contention.
-
Interesting article on the benefit of green tea antioxidant in fighting cancer
https://www.technologynetworks.com/cancer-research/news/antioxidant-found-in-green-tea-may-increase-levels-of-p53-3455.
-
This guy really drills into the cellular level of things
https://jonlieffmd.com/blog/intelligent-cancer-cells-communicate-with-exosomes
-
Kanga re Green tea - a fast route is the supplement EGCG - the active ingredient. If you prefer the tea, Matcha is the best for this nutrient.
-
Lumpectomy is associated with IMPROVED SURVIVAL compared with mastectomy for early stage breast cancer - A Propensity Score Matched Comparison Using the National Cancer Database
-
Thanks for posting that, moth!
That is very important information.
-
Personalized approach needed to manage {metastatic} breast cancer pain
An analysis of patterns of opioid use among 24,752 working-age women with metastatic breast cancer found that most who received an opioid prescription after diagnosis stopped opioids after a few months, but opioid prescriptions increased among a subgroup who could benefit from pain-management plans, based on data reported in Scientific Reports. Prior opioid use was predictive of prolonged use and higher opioid dosage.
Full Story: Healio (free registration)/HemOnc Today (2/20){Free access with registration to reporting; free access to full article. Blurb courtesey of AANP SmartBrief.} -
Armpit Swelling After COVID-19 Vaccine May Mimic Breast Cancer
Axillary adenopathy, or swelling under the armpit, has been reported by women after receiving the Pfizer and Moderna COVID-19 vaccines, but it is also a common symptom for breast cancer.
...clinicians should consider recent COVID-19 vaccination history in the differential diagnosis of patients who present with unilateral axillary adenopathy, according to a new article.
In an article published in Clinical Imaging, Dodelzon and colleagues describe four cases involving women who received a COVID-19 vaccine and then sought breast screening. In describing these cases, the authors sought "to inform the medical community to consider this benign and self-resolving diagnosis in the setting of what can be alarming presentation of unilateral axillary adenopathy.
They hope they will decrease unnecessary biopsies and help reassure patients.
https://www.medscape.com/viewarticle/946448?src=mk...
{Free access to reporting. Registration may be required.}
-
Wow, Lumpie, thanks... my wife will get the 2nd Pfizer/BioNTech dose on the 10th of March and will have her ultrasound on 25th... I'll try to write if something unusual will be reported. Thanks again, Saulius
-
Interesting article out from the National Cancer Institute which says that the Oncotype DX test may be less accurate for African Americans than for White women (also commenting on the need for more diversity in all cancer trials.)
https://www.cancer.gov/news-events/cancer-currents...
-
Here is an article on a topic Lumpie posted about 2/26 - about armpit swelling in women whose mammos closely follow administration of covid vaccines: https://www.sciencedaily.com/releases/2021/02/2102...
"When women undergo breast imaging shortly after receiving a COVID-19 vaccine in the arm, their tests may show swollen lymph nodes in the armpit area. Radiologists say that this is usually a normal finding, and if there are no other concerns, no additional imaging tests are needed unless the lymph nodes remain swollen for more than six weeks after vaccination. The team has published an approach to help avoid delays in both vaccinations and breast cancer screening."
-
jelson
Our local news anchor is a BC survivor herself and ran a story on the lymph node swelling issue. It featured a women who ended up getting a biopsy just to make sure the axillary node wasn’t cancer returning.
Glad to see the word get out on this vaccine SE.
Dee
-
Disappointing results for pembrolizumab (Keytruda)
March 4, 2021 Lancet Oncology https://www.thelancet.com/journals/lanonc/article/...(20)30754-3/fulltext
'Pembrolizumab did not significantly improve overall survival in patients with previously treated metastatic triple-negative breast cancer versus chemotherapy.'
-
Breast cancer is the most frequently diagnosed cancer and the second most common cause of cancer death in women in the USA. In the metastatic setting, despite available therapies, the majority of patients will die from their disease. Thus, new treatments are needed.
Clinical Development of New Antibody–Drug Conjugates in Breast Cancer: To Infinity and Beyond
-
From Springer, all the CDK4/6 data utd compiled
"Do you want to view the latest CDK4/6 inhibitors trial data all summarised in one place? Read our independent clinical trial summary article which features inhibitor trial data, links to key efficacy and safety results and related news items."
https://ime.medicinematters.com/oncology/advanced-...
-
Cognitive impairment tied to breast cancer treatment
A study published in Psycho-Oncology found that from 21% to 25% of patients with breast cancer experienced cognitive impairment during and after treatment. Researchers reviewed 17 studies involving 1,978 breast cancer patients and found chemotherapy appeared to play a more significant role in cognitive dysfunction than radiotherapy and endocrine therapy.
https://www.healio.com/news/primary-care/20210304/...
https://onlinelibrary.wiley.com/doi/10.1002/pon.56...
https://doi.org/10.1002/pon.5623
{Blurb courtesy of AANP SmartBrief. Access to reporting free, may require registration. Access to full article appears to be free.}
-
COVID Relief Bill Contains Lots of Healthcare Provisions
— Includes new incentives for states that haven't expanded Medicaid
For those (in the US) who rely on COBRA, ACA plans or Medicaid for health insurance coverage, this article provides a brief but helpful summary of how coverage is likely to be affected. This includes subsidies and relief from the high cost of coverage for many.
https://www.medpagetoday.com/infectiousdisease/cov...
{Free access but registration my be required.}
-
The recent history of breast cancer in America with "Radical" author Kate Pickert
Interview with book author re history, treatment, evolution of treatment and advocacy around breast cancer. Coverage of early stage and MBC. Very interesting, worth a listen IMO.
https://www.lbbc.org/news-opinion/recent-history-b...
https://bookshop.org/books/radical-the-science-cul...
-
Thanks for the link Lumpie.
-
yes, this looks interesting and there’s an audio book which is great for me
-
From the National Cancer Institute about the new FES PET test for estrogen positive cancers:
https://www.cancer.gov/news-events/cancer-currents...
-
The Next Four Years: How Will Health Care Coverage Change?
By Jane Perkins and Leo Cuello via The American Bar Assocation
During the 2020 election campaign, voters repeatedly identified health care as a topic most important for the next administration to address. Candidate Joe Biden drew a sharp contrast to President Trump on health care and won the 2020 election. So, what can we expect over the next four years? We identify four health care issues that demand attention: controlling the COVID-19 pandemic, protecting Obamacare (also known as the Affordable Care Act and ACA), resuming the path toward expanded health care coverage, and addressing health inequity.
https://www.americanbar.org/groups/crsj/publicatio...
{Pertains to U.S. coverage. Access to affordable coverage is a huge issue for many of us, hence the posting. Free access to article, which is brief rather than exhaustive.}
-
'An accelerated cauldron of evolution': Covid-19 patients with cancer, HIV, may play a role in emergence of variants
Some hospitalized patients with weakened immune systems were shown to have mutating viruses months before the variants were discovered in the outside world
March 11, 2021
{A case report} is one of about 15 similar ones involving immunocompromised patients and recently published in medical journals or preprint servers that have become an important puzzle piece for researchers seeking to understand the origins of the coronavirus variants taking over the world. Those reports lend support to an intriguing theory that some individuals with weakened immune systems due to cancer, HIV or other illnesses may act as incubators for new mutations — an idea bolstered by the astonishing fact that the B.1.1.7 variant, first recognized in the United Kingdom, and B. 1.351, from South Africa, were found in some hospitalized patients months before their discovery in the outside world.
"The evidence points to these immunocompromised patients as an accelerated cauldron of evolution," said David Pollock, a professor of genomics at the University of Colorado School of Medicine.
...the cases have triggered intense debate about how to best manage immunocompromised patients with the coronavirus — whether additional testing or sequencing should be more routine, different isolation procedures considered and alternate treatment protocols followed.
...One of the biggest questions facing doctors treating coronavirus patients with weakened immune systems is how the combination of therapies for SARS-CoV-2 and for cancer, or other underlying illnesses, affect viral mutation.
"I will tell you, to be completely honest, we don't know the best thing to do," Haidar said.
...One common thread among those reported to have prolonged covid-19 infections is a deficiency in what are known as B cells, which produce virus-attacking antibodies — a situation that may allow the virus to replicate with abandon.
According to preliminary findings posted March 2 while a paper is under peer review, Jennifer Dien Bard, who runs the virology lab at Children's Hospital Los Angeles, and her colleagues described seeing two patients with such a condition who kept returning to the hospital and who had persistently positive coronavirus tests with high viral loads.
...The evidence strongly suggests that a patient's inability to mount an immune response "plays a significant role in allowing the virus to really thrive and replicate," she said. Still, she noted, "these are two interesting cases among hundreds of other cases. The likelihood of this happening even to immunocompromised patients is rare and low."
https://www.washingtonpost.com/health/2021/03/11/i...
{Article from Washington Post. Highlights, rather than the entire article, are included owing to length and copyright considerations. If you have questions, PM me. Note that patients discussed in this article had HIV, lymphoma, leukemia and potentially organ transplants. None was noted to be a breast cancer patient and specific chemotherapeutic regimens were not discussed in detail.}
Additional coverage of similar topic, primarily related to organ transplant patients, can be found here:
https://www.medpagetoday.com/infectiousdisease/vac...
{If anyone is aware of studies examining immune response to covid vaccines among those undergoing chemotherapy, I would love to hear about that!}
-
Lumpie--this is for immunosuppressed--not those undergoing chemo. . but it looks like John Hopkins might be studying effect of virus on other vulnerable populations--so they may do something on those undergoing chemo:
https://www.medpagetoday.com/infectiousdisease/vaccines/91631
-
Heads up triple neg peeps - our drugs might not be all that after all.
FDA to reconsider drugs which were given accelerated approval
atezolizumab (Tecentriq)+ Abraxane
"The agency previously granted the therapies accelerated approval, but confirmatory clinical trials assessing their continued effectiveness have since failed.
As a result, the FDA's Oncologic Drugs Advisory Committee has scheduled a special three-day public hearing from April 27 to April 29 to allow patient testimony and expert commentary about the drugs in question. Once the meeting is completed, the committee will consider whether the approvals of the drugs... should be withdrawn and whether further study is needed." https://www.curetoday.com/view/fda-to-evaluate-sta...
-
Moth,
I think the trip negative questioning only pertains to atelizomab, not keytruda. The additional research with keytruda is for very specific other cancers, per the article.
-
ah, yes, BevJen, correct. I will update the post to correct
-
Moth,
No worries. I am hyper fixated on keytruda bc that's what I'm on, so I scoured all of the reports on that.
I am surprised by the atezo, because my center was one of the testers of that. Plus, that's what you are on, correct? And you seem to be doing well on it.
Bev
-
the atezo trial results have been all over the place. Atezo+abraxane seemed to have some good prelim results, atezo+ taxol was a dud in the trials (though there was some subgroup analysis that again showed some benefit for a subpopulation....but it was underpowered & not part of study design). Atazo + taxol is what I started on & have had good response - I think I've beat the median pfs. I think the more mature atezo+abraxane data might be coming this year.
some onco twitter chatter was that they were wondering if PD-L1 had to be a certain threshold (not just positive/negative) for it to work but I think also some think there's another mutation that it's targetting. There are a few good responders with durable response so ... fingers crossed that I'm one of the unicorns. I've technically had two oligoprogressions on it but my liver mets continue to slowly shrivel up - which apparently is classic immunotherapy response: slow to start, longer duration rather than wham/bam/tumor dead (& then resistance) that you get from effective chemo.
-
Time to Revisit Distant Nodal Status in Breast Cancer Curability?
— Comparable survival for distant and regional nodal involvement, when treated similarly
by Charles Bankhead, Senior Editor, MedPage Today March 16, 2021
You may need to set up a free account to view the article.
-
eribulin PLUS pembrolizumab for mTNBC phase 1b/2 reporting https://pubmed.ncbi.nlm.nih.gov/33727258/
higher ORR (34.5% ) and OS (21 mo) in PDL1+ 1L pts
there were a number of complete responses in the trial (Stratum 1 was 1st line); there were complete responses in stratum 2 as well (2nd or 3rd line tx)
-
2019whatayear, that looks like an important article that relates to questions I have seen BCO members post, about whether contralateral node involvement makes them stage iv or not. I read it as saying that contralateral lymph node involvement should be treated with curative intent, as stage III or oligometastasis.
-
Yes SP a lady I follow on Twitter posted it. Really interesting seems like in these cases if I was the patient I’d push for the aggressive curative intent
-
As someone with Her2+ cancer, I have found the topic "Articles of Interest" on Her2Support.org helpful for research news too.
https://her2support.org/vbulletin/forumdisplay.php?s=0224bf18cca3db2e508558a147904455&f=31
-
Oral taxane tesetaxel is being withdrawn from development
https://finance.yahoo.com/news/odonate-therapeutic...
"clinical data package for tesetaxel is unlikely to support FDA approval." ... so it turns out it didn't actually work all that well
-
In fact, women appear hardwired to experience COVID-19 and the vaccines differently. Data from the CDC suggests side effects from the vaccines are worse in women; for example, 63 of the total 66 reported cases of anaphylaxis happened in women.
Why Women Experience COVID and the Vaccines Differently Than Men
-
Antibody drug conjugates article on Springer
Clinical Development of New Antibody–Drug Conjugates in Breast Cancer: To Infinity and Beyond
https://link.springer.com/content/pdf/10.1007/s40259-021-00472-z.pdf
I have skimmed the paper. Lots of hope for ADCs including ER/PR + Her2-
Dee -
Research article associating breast adipocyte size and COX-2 expression in DCIS cells with higher potential for DCIS to develop into invasive breast cancer.
https://www.nature.com/articles/s41523-021-00232-w
I don't yet understand all of the details but it reinforces that looking at BMI primarily is not always a good answer.
-
PKNC - is breast adipocyte the same as "dense breast". I wonder if that is why I have had so much trouble
-
I’m not sure, but what I think this article is getting at, is that the size of the breast fat cells, which tend to be larger in obese and post menopausal women (any weight) due to inflammation, are associated with cancer progression.
-
BlueGirlRedState: No, breast adiposity is NOT the same as dense breasts. In fact, it is sort of the opposite. On imaging, fat, aka "adiposity," is very translucent, so it is relatively easy to see tumors and high risk tissue in fatty or adipose breasts. Dense tissue looks like solid white on imaging. It is hard to see through, so it is difficult to see tumors hiding in dense tissue. The benign dense tissue and a tumor look very much the same. That is why mammograms are not as effective at finding breast cancer in women with dense breasts. Research and development is looking at techniques to combat these challenges... things like artificial intelligence and thermography. I may be able to scrape up a link to some propaganda from GE on their R&D which discusses this a bit if anyone is interested. As someone with dense breasts - which unquestionably hid my BC for *at least* a year if not longer - I am very glad to know that work is being done to try to overcome this screening challenge.
PS: Anyone else find it amusing and frustrating that many of us spend too much time, effort and distress on trying to rid our bodies of fat elsewhere, but that fat, which comprises the majority of healthy, mature, female breasts is deemed cosmetically desirable? Not everyone, but many....a la "Why can't my muffin tops relocate to my breasts?"
-
🤔😂 Lumpie!
-
Lumpie - thank you for the laugh. One person posted that her DR told her that changes she was seeing in her fingers were because she was losing fat there, rather than in her "handles". It just is not fair. I was considering DIEP at one time, turning love handles into boobs sounded good. But I was not a good candidate, not the right kind of fat in the right places.
-
BlueGirlRedState: Oh dear. I am so glad no one told me I had "the wrong kind of fat" at an inopportune moment. That could have been dangerous!
-
since starting letrozole in early January I have gone down some brassiere sizes.
-
Sharing FYI:
You may qualify for our sponsored post-mastectomy bra program {from AnaOno} powered by Natrelle Inspires!
Enter your information to submit your request. Bra requests will be fulfilled on a first-come-first-serve basis, and quantities are based on the number of Natrelle Inspires bras sold. The program is available to newly-diagnosed (within one year) patients, processing fees such as shipping and handling may apply.
https://anaono.typeform.com/to/MTU5gpeb?utm_source...
Gratuitous comment: I have purchased from AnaOno before. I love their products (comfortable, high-quality) and, in my experience, they have great customer service.
-
Cyclophosphamide-Free Adjuvant Chemotherapy for Ovarian Protection in Young Women with Breast Cancer
https://www.practiceupdate.com/C/116102/56?elsca1=emc_enews_topic-alert
TAKE-HOME MESSAGE
- This randomized, phase III trial conducted across eight hospitals in China was designed to evaluate the menstrual resumption rate and disease-free survival in women with ER-positive, HER2-negative, early-stage breast cancer receiving epirubicin and cyclophosphamide followed by weekly paclitaxel (EC-P) or epirubicin and paclitaxel followed by weekly paclitaxel (EP-P). The menstrual resumption rate at 12 months after chemotherapy was 48.3% in the EC-P group compared with 63.1% in the EP-P group, with an absolute difference of 14.8% (P < .001) and an estimated odds ratio of 1.83. For the second primary endpoint of disease-free survival (DFS), the 5-year DFS rate was 78.3% in the EC-P group compared with 84.7% in the EP-P group. There was no statistically significant difference in distant disease–free survival or overall survival. Post hoc exploratory analysis found that the successful pregnancy rate was higher in the EP-P group (9.6% vs 2.7%; P = .03).
- Cyclophosphamide-free chemotherapy may be associated with a higher probability of menses resumption with potential fertility implications and minimal impact on disease-free and overall survival.
-
New report out
“The hormonal (endocrine-related) therapies that serve as a backbone for treatment of both (breast and prostratecancers improve survival but also increase cardiovascular morbidity and mortality among survivors. This consensus statement describes the risks associated with specific hormonal therapies used to treat breast and prostate cancer and provides an evidence-based approach to prevent and detect adverse cardiovascular outcomes.“
https://www.ahajournals.org/doi/10.1161/HCG.0000000000000082 -
Thanks AlabameDee. Interesting (selfishly) to me that they included tamoxifen and raloxifen under SERMs but not toremifene.
Also ugh.
-
Alabama - thank you for the post, one more question to ask the oncologist, see if it is being monitored and what to do about it. Probably another damn drug. Starting to feel like the little old lady who swallowed a spider to catch the fly that wiggled inside her. I don't know why she swallowed the fly..........
-
FDA to scrutinize unproven cancer drugs after 10-year gap
Each year the U.S. approves dozens of new uses for cancer drugs based on early signs that they can shrink or slow the spread of tumors.
But how often do those initial results translate into longer, healthier lives for patients?
Tuesday ... the Food and Drug Administration convenes the first meeting in a decade to consider clawing back approvals from several cancer drugs that have failed to show they extend or improve life.
...many researchers say it has failed to crack down on medications that don't deliver on their early promise, leaving a glut of expensive, unproven cancer drugs on the market.
spending on cancer drugs has more than doubled since 2013 to over $60 billion annually, according to the data firm IQVIA. New medications typically cost $90,000 to $300,000 a year. And those prices have risen much faster than patient survival.
The FDA is prohibited from considering cost, but it is supposed to keep ineffective drugs off the market.
...Harvard researchers dug into that claim, they found that only about 20% of cancer drugs had actually been shown to extend lives.
https://apnews.com/article/us-news-health-science-...
{Free access to reporting.}
-
That seems like great news Lumpie. It is frustrating that it took so long.
-
Even if a drug does not extend life, if it improves quality of life, it deserves approval. (Anyone who is in treatment for stage iv cancer knows this!) Also, sometimes a drug may not show great results for a whole study group, but may work well for some people, and it should be available to them
-
Shetland Pony, I agree, thanks for saying this. I was apprehensive at reading that.
-
One of the rapid approvals they were reconsidering was the drug I'm currently on - atezolizumab/Tecentriq. Two very conflicting trial results (Impassion 130 and Impassion 131)
It was a 7-2 vote to keep it for mTNBC https://www.onclive.com/view/fda-panel-supports-at...
"The FDA's Oncologic Drugs Advisory Committee voted 7 to 2 in support of maintaining the indication of atezolizumab in combination with nab-paclitaxel as a treatment for adult patients with unresectable locally advanced or metastatic triple-negative breast cancer whose tumors are PD-L1 positive."
-
When you read quotes from Zeke Emanuel, understand that he wrote this in 2014:
https://www.theatlantic.com/magazine/archive/2014/...
and recently updated thoughts:
https://www.advisory.com/daily-briefing/2019/08/26...
So that's the oncologist in the article above saying it doesn't matter if you die from a big tumor or a small tumor because you're still dead.
Good lord, I don't want a guy like that deciding what drugs that have already been approved are not "worth" keeping available to cancer patients.
-
Tectonic shift - yes, I saw his name and I am a long time non-fan of that guy. Imagine him as your personal oncologist, I shudder at the thought.
He doesn't belong anywhere near public health care planning but unfortunately, he is well connected.
Love this take on old people /not really
"These people who live a vigorous life to 70, 80, 90 years of age—when I look at what those people 'do,' almost all of it is what I classify as play. It's not meaningful work," he said. "They're riding motorcycles; they're hiking. Which can all have value—don't get me wrong. But if it's the main thing in your life? Ummm, that's not probably a meaningful life."
And here’s commentary on the other guy, from a Statnews article :“His critics, however, say Prasad is putting too much weight on statistical tables, instead of listening to the real-world experience of real-life patients and physicians. They also dismiss him as a generalist who doesn't really understand the specialty fields he so angrily attacks — and doesn't try to.
"He never wanted to hear the other side," said Dr. Ben Davies, a urologist at University of Pittsburgh who has clashed online with Prasad. "In general, there's an absolutism to his voice, which grates a lot of researchers the wrong way."
Dr. Tomasz Beer, a prostate cancer researcher at OHSU — and the man responsible for bringing Prasad up to Portland — has been called upon to defend some of his more controversial remarks: "I've gotten calls from people at respected institutions saying, 'Why the hell did you hire this guy?'" Beer said. "My answer: We support academic freedom and he's doing good work."
-
Thanks for sharing the articles. It shows us what we are up against.
😳”But if it's the main thing in your life? Ummm, that's not probably a meaningful life.“
Oh the arrogance of such a quote. Who is this person to assume he knows what later in life activities qualify as meaningful. Just being a grandparent and great grandparent is soooo meaningful, not only for the person but for society. I could go on. 😡
I just had a conversation with an endocrinologist for a couple of issues to get her opinion. While she responded reasonably to the issues, when we discussed my weekly burst prednisone therapy that gives me tolerable QOL from my trial SE, she actually said that prednisone was just as bad as narcotics. 🙄. I won’t be going back to her.
Dee
-
Picking an age to die by (Ezekiel J. Emanuel) makes no sense considering the wide range in health/ quality of life in all age groups. And everyone has to define that for themselves. I think back to years ago when I stopped to apologize to a bicyclist I thought I had run of the road. He told me everything was fine and that he was turning. Then he asked me to guess how old he was. Turns out he was 95!! We chatted a while. When I asked him what the secret was to such a long life, he asked me to lean in really close so that noone else would hear. "Keep breathing" he whispered. I laughed, and replied, "and a sense of humor"
-
wonderful interaction blue girl. And reminds me of when I was driving to my appointments pretty early on, Ariana Grande’s song used to come on the radio “Just keep breathing, breathing, breathing...”. I turned it into a mantra. And humor is definitely a plus! Love this.
-
this is going to sound terrible but that doctor and all his viewpoints shows how sanctimonious and pompous some doctors can be. Thank goodness they're not all that way.
-
Vaccine Therapy to Prevent Recurrences in HER2-Positive Breast Cancer
Brief interview with Lee S. Schwartzberg MD, FACP about vaccine research. Spoiler alert: seems promising. Read the transcript or listen to the narrative.
https://www.practiceupdate.com/C/117405/56?elsca1=...
{No charge to red/listen but registration may be required.}
-
Regarding drug approval: part of the consideration is whether the now drug is less expensive than currently available options. This seems questionable to me. We still don't fully understand why some drugs work in one patient but not in another. Patients have allergic reactions to some drugs but not others. It seems to me that having more in one's proverbial arsenal is an advantage in an of itself.
As regards an age to die: kind of silly. People's outlooks change. Think of how many people early in life practically say "broken bone? Euthanize me!" but in later life say "not so fast!." One's outlook changes with one's circumstances.
-
In breast, prostate cancer survivors, hormonal therapies may raise CV risk
Hormonal therapies for the treatment of breast and prostate cancers may improve survival among patients with cancer, but also may confer poor CV {cardiovascular} outcomes among survivors.
3 minute read with links.
https://www.healio.com/news/cardiology/20210428/qa...
{Access to article is free but may require registration.}
-
i refuse to register/create accounts just to read an article (pet peeve). Can someone that is already registered tell me what vaccine they're talking about for HER2+? Is it the one presented at SABCS 2020 or something else? I'm in a Moffit run Vaccine Trial, getting the DC-1 vaccine.
-
this is almost the whole transcript. I hope this would lead to something that helps those of us who are already MBC as well

-
thanks!
-
cancer immunotherapy & increased risk of venous embolism (blood clots)
https://www.cell.com/med/pdf/S2666-6340(21)00063-5.pdf
Roopkumar et al., Med 2, 423–434 April 9, 2021 ª 2021 Elsevier Inc. https://doi.org/10.1016/j.medj.2021.02.002
Cancer itself raises riks of blood clots. Now it seems immunotherapy treatment adds additional risk. This study found 24% of pts on immunotherapy developed embolism.
-
SBRT Safe for Cancer Patients With Multiple Metastases
Given the critical need, NRG Oncology NRG-BR001 trial sought to determine the safety of delivering curative-intent SBRT to patients with 3 to 4 metastases or 2 metastases within close proximity to each other.
https://www.medpagetoday.com/radiology/therapeutic...
Love the phrase curative-intent!!
Dee
-
woooh nice one Dee!
-
Cryoablation Promising for Early Breast Cancer
Almost all patients and physicians report satisfaction from cosmetic results; overall recurrence rate 2.06 percent
Cryoablation seems promising for early breast cancer and has minimal risks, according to a study presented at the annual meeting of the American Society of Breast Surgeons, held virtually from April 29 to May 2.
Richard E. Fine, M.D., from the West Cancer Center & Research Institute in Germantown, Tennessee, and colleagues examined the safety and efficacy of cryoablation for women aged 60 years and older with unifocal, ultrasound-visible invasive ductal carcinoma ≤1.5 cm in size; tumors were hormone receptor-positive, human epidermal growth factor receptor 2-negative. One hundred ninety-four patients (mean age, 75 years; mean tumor size, 7.4 mm) met the eligibility criteria and received successful cryoablation treatment per protocol, receiving a freeze-thaw-freeze cycle for 20 to 40 minutes. Patients were followed up at six months and then annually to five years.
The researchers observed no significant device-related adverse events or complications reported among the protocol-treated patients. Most adverse events were minor. Fifteen patients underwent sentinel lymph node biopsies; one had breast cancer-related positive sentinel lymph nodes, with no recurrence at 60 months of follow-up. Overall, 27, one, and 148 patients underwent adjuvant radiation, received chemotherapy, and began endocrine therapy, respectively. During the follow-up visits, more than 95 percent of patients and 98 percent of physicians reported satisfaction from the cosmetic results. Only four of the protocol-treated patients had recurred at a mean of 34.83 months of follow-up (2.06 percent overall recurrence rate).
"Cryoablation potentially represents a dramatic improvement in care for appropriate low-risk patients, and at three years' posttreatment, the ICE3 trial results are extremely positive," Fine said in a statement.
https://www.practiceupdate.com/C/117648/56?elsca1=...
https://www.breastsurgeons.org/meeting/2021/docs/p...
{Report based on presentation at the annual meeting of the American College of Breast Surgeons. Reporting and access to press release are free. While this approach was targeted to a specific subset of patients, further de-escalation of treatment and fewer side effects sure would be a plus for those able to benefit.}
-
This is the second recent study to come out showing BETTER breast cancer survival from lumpectomy + rads than from mastectomy
"The cohort included all women diagnosed as having primary invasive T1-2 N0-2 breast cancer and undergoing breast surgery in Sweden from 2008 to 2017"
almost 50,000 Swedish pts
"Breast conservation seems to offer a survival benefit independent of measured confounders and should be given priority if both breast conservation and mastectomy are valid options."
https://jamanetwork.com/journals/jamasurgery/fulla...
My editorial comment: We urgently need to add this evidence into discussions of pt decision making about surgery. My perception is still that too many pts make a non evidence based decision, and that a system which financially rewards surgeon + cosmetic surgeons teams for more aggressive surgery might be contributing to poorer outcomes for women.
-
moth you are right. So many women are afraid to keep their breast; a knee jerk fear.
-
I, too, have talked with SO many friends, colleagues... even medical professionals.... who automatically assume that a mastectomy is more effective. I hope that better information gets to the people who need it. Part of the problem is that people are often obliged to make a decision quickly and with inadequate information. It can also be difficult to get insurance coverage to correct post-partial cosmetic issues. I wonder if this may impact some patient decisions.
-
I completely agree that this information needs to be made known to newly diagnosed patients.
Will BCO be making content on this? I hope so.
Unfortunately the mastectomy vs lumpectomy w/radiation decision is often made when people are in the shock and awe phase, and under pressure to act quickly. To make matters worse, I think our culture of celebrity plastic surgery leads a few women to believe that they will get Hollywood results from their reconstruction, which is just not usually the case when it comes to breast cancer.
My personal opinion (having done both surgeries, and lived with the consequences) is that unless it is medically necessary for some reason, a mastectomy should not generally be offered when a lumpectomy with radiation is a viable alternative. Just my opinion! I know others will disagree, and that's okay.
-
I posted about this in another thread but will repeat here, since here is where this discussion is getting more traction. I don't think we know enough of why patients choose one option or the other to conclude that there is this widespread, uninformed, knee-jerk decision process. It is not unreasonable to want a breast (or both) removed after a breast cancer diagnosis. That was my case, I had very dense breast tissue that rendered any screening, including 3D mammograms and MRIs, completely useless. Also, we don't know the reasons for the better outcomes in that study, and it could be that radiation is behind the better outcomes, and which surgery one chooses, lumpectomy or mastectomy, is irrelevant, and that what should be reviewed is when to offer radiation. I am very happy I had a mastectomy. Down the road I chose to have a prophylactic one on the non cancer side. For one thing, I went through 20+ years of useless cancer screening, and I am happy I will never get another mammogram. We shouldn't jump to conclusions so quickly.
-
LaughingGull, I do think that situations like yours where screenings risk being ineffective or too burdensome can be good reasons to opt for a mastectomy. It's certainly not a one size fits all matter.
As an aside, I think you raise an interesting point that if the radiation is in fact responsible for the better overall survival, maybe radiation should be offered after some mastectomies, where it currently is not, as you say.
-
Just to be clear that study compared 3 groups.
Lumpectomy + rads had better outcomes than mx + rads. Mx - rads was worst.
Certainly there are many other reasons why someone might want a mx.
-
The truth is, we don't know the cause for the better outcomes, right? Not clear from the study.
I was offered radiation after the mastectomy. There is some criteria for radiation post-mastectomy (which I dont remember precisely but related to how widespread the cancer was) and I qualified. Insurance didn't complain.
-
The outcomes are regarding deaths from recurrence and it doesn't include deaths from heart damage from radiation. I belong to the group of women who asked to have BMX for several reasons that are unique for me (us): difficult to read mammograms of very dense breast, to avoid radiation on the left side next to the heart to avoid future heart disease, to reduce anxiety for future 6 months scans, to reduce local recurrence in the other breast, etc. So, there is no size fits all.
-
clarifying further, this study looked at both breast cancer specific mortality & overall mortality so damage from radiation would also have been captured
-
I thought I would post this caveat re post-op mammograms:
"Mammograms will be recommended if you had a special type of mastectomy called nipple-sparing mastectomy, also known as subcutaneous mastectomy. In this surgery, you keep your nipple and the tissue just under the skin. Enough breast tissue remains to warrant the continued use of screening mammograms.
"Breast MRI is another and possibly more effective way to screen women who have had breast reconstruction and are at high risk for recurrence."
Obviously, your care team should be providing guidance on on-going screening, but recommendations change so it is good to go in "forearmed" with up to date research and recommendations, especially if you are high risk or have had a more complex case or surgery and have been transitioned back to your PCP for post-early stage care.
Source: https://www.breastcancer.org/symptoms/testing/type...
PS: I knew I had read about post-mastectomy mammograms so I went searching for when those were recommended. It must be the particular subset noted above. Surgical options change... recommendations change.... take care & stay healthy out there!
-
Survival is not the only criteria when choosing MX vs lumpectomy. I have extremely dense breasts. I have been going through regular (every 6 months) ultrasounds for the last couple of years and at the end I found the tumor myself. I don't want to have to go through this ever again and so MX is the best choice in my case. I don't believe choosing either approach should be restricted.
-
Went back to the study and indeed, it says that lumpectomy + rads had better outcomes than mx + rads. My bad. However, it also says: "It remains unclear whether this is an independent effect or a consequence of selection bias"
-
Thank you Lumpie. I had a nipple-sparing mastectomy and my doctors told me I no longer need mammograms. I should ask on the next appointment. I wonder what other women like me are recommended.
-
Lilly I also had a nipple sparing mastectomy, and no one has mentioned getting a mammogram at all. I have had one MRI however but that was related to determining an issue with a neuroma. I, too, had extremely dense tissue, cancer on left side close to chest wall. I really didn't want the radiation, although I knew it was still on the table depending on margins. I would love to be able to see more of the data from this study. As a previous poster stated it may be the radiation itself is the key driver. Thanks, Moth, for sharing this.
-
I apologize that I'm out of sequence, but I'm chiming in on the heart disease / negative impacts from Tamoxifen in this article. It states - "Anti-estrogen therapy with tamoxifen also increases the risk for metabolic syndrome." I am living proof of that. I didn't even know what this was until I got it from Tamoxifen. My HbA1C went from 5.0 to 5.7 within 3 months on the drug. Unfortunately, I stayed on Tamoxifen for 3 months more because I didn't grasp what was happening to my liver and my PCP just breezed over it. Now, I have to severely restrict my carbs in the hope that I can circumvent diabetes, tiny amounts set off a blood sugar spike. I wish I had never taken the drug because it did nothing for my DCIS and may have permanently damaged my liver. Just a warning to all women that there are always those who fall into the "unintended side effects" camp.
May 2, 2021 11:27AM - edited May 2, 2021 11:28AM by Lumpie
In breast, prostate cancer survivors, hormonal therapies may raise CV risk
Hormonal therapies for the treatment of breast and prostate cancers may improve survival among patients with cancer, but also may confer poor CV {cardiovascular} outcomes among survivors.
3 minute read with links.
-
Dear all, I am sure you all know it but ESMO2021 is so much about this drug, another big TROP2 gamechanger for mTNBC (and not only!): Dato-DXd, build on same platform as Enhertu (T-DXd) by Daiichi Sankiyo! Saulius

-
Any knowledge or experience with unintended SEs with Exemestane/Afinitor? I was alarmed to read one article about very rare instances of lung damage. I'm off Afinitor during radiation, last day is Thrusday (hooray!), Other risks - kidneys, blood-sugar, BP..... Somewhere I saw a graph comparing Exemestane with/wiithout Afinitor, and it seems like the benefits drop rapidly
-
BlueGirlRedState, check out the pneumonitis thread started by DogersGirl https://community.breastcancer.org/forum/8/topics/...
-
Thanks moth, I've added it to my favorites
-
BlueGirlRedState- Ref Afinitor and pneumonitis: Report ANY sense of shortness of breath to your MO so they can monitor your lungs
Thanks Moth for sharing the link. I shared my struggles hoping to help othet
-
When I was diagnosed with DCIS in 2017, I felt somewhat pressured to go with lumpectomy/radiation. One of the questions I asked my MO was—if I get a future recurrence, won’t reconstruction be more difficult? She kind of scoffed at my silly question. Well, recurrence happened about 18 months later. Had a mastectomy which took a long time to heal due to radiated skin. I wasn’t able to consider any reconstruction due to Covid and I’m not even sure that I was able to get any other surgery due to radiated skin. Now, lo and behold recent mammogram identified suspicious lesion on right breast. I’m getting biopsy in a couple days. If I had been brave enough to get bilateral mastectomy in 2017, I believe I would be much better off today. Right now I’m just scared and sad. Hindsight is 20/20 but I think individuals need to be given enough info to make a truly informed decision that’s right for them. I was sold on the notion that DCIS doesn’t spread, etc, etc. I’m learning that the rate of subsequent cancer occurrence is higher than I really understood.
-
CDK inhibitors may boost the effectiveness of immune therapy in metastatic breast cancer
Reviewed by Emily Henderson, B.Sc.May 10 2021A class of drugs that inhibits breast cancer progression when used with hormonal therapy might also boost the effectiveness of immune therapy in cases of recurrent, metastatic breast cancer, according to a new study led by researchers at The Ohio State University Comprehensive Cancer Center - Arthur G. James Cancer Hospital and Richard J. Solove Research Institute (OSUCCC - James).
Published in the journal Cell Reports, the findings of the animal study suggest that drugs called CDK4 and CDK6 (CDK4/6) inhibitors might improve the effectiveness of immune therapies for metastatic, estrogen-receptor-positive (ER+) breast cancer.
We know that CDK4/6 inhibitors effectively slow the progression of newly diagnosed breast cancer, but they don't kill cancer cells. Consequently, the disease often recurs, and then it is usually fatal because we have no effective therapies for recurrent disease. Our findings suggest that combining CDK4/6 inhibitors with immunotherapy might offer an effective treatment for recurrent, metastatic ER+ breast cancer."
Anna Vilgelm, MD, principal investigator, a member of the OSUCCC - James Translational Therapeutics Program and assistant professor at the Ohio State College of MedicineSpecifically, the study shows that CDK4/6 inhibitors can improve the efficacy of T-cell-based therapies such as adoptive T-cell transfer or T-cell-activating antibodies in animal models of breast cancer.
Immune therapies are proving to be effective treatments for a variety of cancers but not for advanced breast cancer. One problem is that breast tumors often have low numbers of cancer-killing T lymphocytes within the tumor. Such tumors tend to respond poorly to immune therapies.
Related Stories
- Combination of BMI and body shape predictor can help determine the risk of obesity-related cancers
- Targeted therapies could exploit unique metabolic features of pancreatic cancer cells
- Low dose of a four-drug combination helps prevent cancer metastasis in mice
"In addition, breast cancer patients with low numbers of tumor-infiltrating lymphocytes often have worse survival compared to patients with high numbers of infiltrating lymphocytes in their tumors," says Vilgelm.
The new study shows that CDK4/6 inhibitors cause breast tumors to secrete small proteins called chemokines that attract T cells. This can help to improve patients' response to cancer immunotherapies.
For this study, Vilgelm and her colleagues used the oral CDK inhibitor palbociclib, mouse models, breast cancer cell lines and analyses of The Cancer Genome Atlas (TCGA) to study the influence of CDK4/6 inhibitors and chemokine production in the tumor immune microenvironment and on patient outcomes.
Key findings include:
- Pre-treatment with a CDK4/6 inhibitor improves recruitment of T cells into tumors and improved the outcome of adoptive cell therapy in animal models;
- CDK4/6 inhibitor-treated human breast cancer cells produce T-cell-recruiting chemokines;
- TCGA analysis showed that chemokine expression is a favorable prognostic factor in breast cancer patients;
- mTOR-regulated metabolic activity is required for chemokine induction by CDK4/6 inhibition;
- T-cell-recruiting chemokines may be useful prognostic markers for stratifying patients for immunotherapy treatment.
"Overall," Vilgelm says, "our findings suggest that CDK4/6 inhibitors may offer a therapeutic strategy that can attract T cells into breast cancer tumors, which may increase their sensitivity to immune therapies."
-
Jetcat, I'm sorry you're going through this. I just wanted to chime in and say that prior radiation doesn't necessarily rule out implant reconstruction, although you're correct in that there can be more difficulty with healing. I had an implant after radiation with no trouble, although it has since been removed for other reasons related to the cancer and I'm half flat now. There's also the DIEP and other flap procedures.
Anyway, don't lose hope, there are options out there. Best wishes.
-
Thank you. When I was first diagnosed I was still working in a corporate type job and probably would have done some type of reconstruction. Now that I’ve retired at 62, I actually wouldn’t be upset about going flat. My surgeon did an outstanding job of a very tight, smooth closure. Half flat isn’t bad either but I really think I’ll pursue another mastectomy if I even have a choice.
All the best to you !
-
Dear all, some fresh news on HER2+ drugs in HER2low sub-population (found by one silent member on these forums): https://t.co/xme5TSU2GD?amp=1
Also, for the first time Enhertu's bystander effect is really proved: https://clincancerres.aacrjournals.org/content/ear...
-
it is like every time I want to read an article they want me to sign up but I’m not going to do that it’s really getting annoying. I’m not going tohave 10 million passwords floating around.
-
Springdaisy, I was able to read the article without a password by selecting the option for a physician.
-
Springdaisy, usually abstract is enough to know if you want to read deeper. I'd say I am usually directly interested in 5 % of articles, and try to get those by choosing physician:) or looking around for other free-access. Saulius
-
New technology makes [mouse mammary] tumor eliminate itself
Scientists at the University of Zurich have modified a common respiratory virus, called adenovirus, to act like a Trojan horse to deliver genes for cancer therapeutics directly into tumor cells. Unlike chemotherapy or radiotherapy, this approach does no harm to normal healthy cells. Once inside tumor cells, the delivered genes serve as a blueprint for therapeutic antibodies, cytokines and other signaling substances, which are produced by the cancer cells themselves and act to eliminate tumors from the inside out...
With [this] system [called SHREAD: for SHielded, REtargetted ADenovirus] the scientists made the tumor itself produce a clinically approved breast cancer antibody, called trastuzumab, in the mammary of a mouse. They found that, after a few days, SHREAD produced more of the antibody in the tumor than when the drug was injected directly. Moreover, the concentration in the bloodstream and in other tissues where side effects could occur were significantly lower with SHREAD. The scientists used a very sophisticated, high-resolution 3D imaging method and tissues rendered totally transparent to show how the therapeutic antibody, produced in the body, creates pores in blood vessels of the tumor and destroys tumor cells, and thus treats it from the inside.
https://www.eurekalert.org/pub_releases/2021-05/uo...
-
debbew, I came here to post the same news. It sounds so promising. They are trying to apply their process to covid 19, I wonder if it will help streamline clinical trials for actual patient use.
-
This sounds interesting, if still a ways off:
-
From April 21: Patients undergoing hormone therapy for breast and prostate cancers may be at increased risk for cardiovascular disease (CVD) as they age and should be closely monitored for potential cardiovascular events, according to a scientific statement from the American Heart Association (AHA).
-
Lymph Node Findings on PET: Cancer or COVID Vaccine?
— Post-jab radiotracer uptake "could prompt unnecessary biopsies and treatments"
-
On COVID vaccine and cancer:
Cancer Patients Develop 'Adequate' Immune Response to COVID Vax
-
Joyner, thanks for posting that link. These two paragraphs really stood out to me, which were not quite as optimistic as the headline, but I'm still glad people are beginning to study this. (I added the bold, for emphasis.)
"A total of 92 of the 102 cancer patients in the study were found to be seropositive for SARS-CoV-2 antispike IgG antibodies after the second dose of vaccine, compared with 100% of the controls, the researchers reported, adding, however, that the median IgB titer in cancer patients was significantly lower than in controls (1,931 vs 7,160 AU/mL).
...
"As the correlation between antibody levels after vaccination and clinical protection has not yet been established, further research is required to determine the magnitude and duration of protection the vaccine provides to patients with cancer," the authors concluded. "Nonetheless, our findings do suggest that vaccinating such patients during anticancer treatment of any kind should be a top priority."
-
Immunotherapy & chemotherapy together might NOT give very good covid 19 vaccination response - or it might be having breast or lung cancer that drove the difference
https://jamanetwork.com/journals/jamaoncology/full...
"the only treatment regimen associated with significantly lower IgG levels on multivariable analysis was chemotherapy with immunotherapy; however, only 14 patients received this combination therapy, and no association was seen with either chemotherapy or immunotherapy alone. Given that chemotherapy combined with immunotherapy is only used in select cancer types (eg, lung cancer, triple-negative breast cancer), it is possible that other cancer-specific factors drove the observation in this small subset."
-
Some good insights from ASCO 2021 how science is slowly wining and how bad MBC actually is:
1095 Survival among patients with untreated metastatic breast cancer. JK Plichta, SM Thomas, S Sammons, et al
Take-Home Message
- This study evaluated the survival outcomes of metastatic breast cancer (MBC) patients who opted to receive no treatment for their disease. The medial unadjusted overall survival (OS) in the untreated group was 2.5 months versus 36.4 months in the treated group (P < .001). Higher tumor grade, higher comorbidity score, increased age, and triple negative (vs HR+/HER2−) tumor subtype (all P < .05) were all associated with decreased OS in the untreated cohort; however, the number of metastatic sites was shown not to be associated with OS.
- Patients with MBC who choose to forgo treatment are more likely to have comorbid conditions, be of advanced age, and have clinically aggressive disease. The prognosis for untreated MBC is extremely poor.
Saulius -
BSandra: Your post comes less than a week after I met a woman on the golf course who was diagnosed 8 years ago at age 57 with De Novo Stage 4 Triple Negative breast cancer. I wish that scientists could figure out why some women seem to come out on top of this damn disease and appear to flourish. I had seen her several years ago in my weight lifting class at the gym and of course, I had no idea that she had breast cancer. I don't know if this is relevant or not, but at age 65, she looks more like 45 and has a natural, lean, muscular build - I assume her body fat is very low. Perhaps she has an exceptional internal metabolism and immune system, or is simply a good responder to treatment. What is the bitter pill is that she had a mammogram 6 months before her diagnosis that was passed on as clear, and that she found the lump herself in the shower.
-
Dear PAKNC, every C is very personal. Science is looking for patterns and medians - it is so darn difficult (maybe even impossible!) to analyze single cases and find correlations. There's something special in her disease, for sure, but also stage 4 is not equal to another stage 4. One small metastasis in one organ is stage 4 too but can hardly be compared to an extensive multi-organ involvement. I am sure her good performance status helped to go through treatments - at stage 4, if we dream of a cure, we have to throw everything at it. Time window is also important. Good metabolism usually negatively correlates with disease progression. Then genetics too. Too many factors. But again, I'd like to meet such a person in person:)
Also some interesting insights from ASCO 2021. Many publications are breath-taking. Like "Mastering the Use of Novel Anti-HER2 Treatment Options" by P. Tarantino that states
"Finally, it is now established that a subset of patients with HER2-positive mBC can achieve long-lasting responses to HER2 blockade. Indeed, the CLEOPATRA trial showed that 16% of patients receiving frontline dual blockade are free from progression after 8 years of treatment.10 This observation raises the
following compelling scientific questions: (1) Are these patients cured? (2) Can we identify this population up front? (3) For how long should these patients receive maintenance anti-HER2? (4) Can we increase this percentage by adopting more intensive treatment strategies?"Scientist are extremely careful about asking a question "Are these patients cured", so if they ask it, they believe there are some cures. Cures in MBC! With first line treatment! And yet there are 4-5 new treatment lines (very effective ones!) after the first one for this population, so... WE ARE GETTING THERE!
Saulius
-
Oh, yes, Saulius, possibly curing deNovo HER2+ MBC was discussed at esmo 2021 also. I grabbed four slides that were shared on Twitter, I’ll try to post here. Also, I saw an older YouTube video, which I can’t find anymore, where the researcher talked about the need to study the question and how it could be similar to leukemia patients on Gleevec who were doing very well but no one knew how or when or if the medication could be discontinued until they finallyset up some trials.

-
-
of course at the end he asks “are we crazy” 😂 if daring to think outside the box is crazy maybe so. Wish I could
have seen the whole presentation


-
fascinating. Thanks and for posting
-
PAKNC, I'd be wondering where her mets are. I know another mTNBC long hauler online and her single solitary met was to a distant lymph node. I know there's discussion about reclassifying those as 3C as those tend to be the outliers in mTN & likely should be treaed with curative intent.
my only takeaway from ASCO at this point is that it is increasingly clear that breast cancer is not one disease & so we can't really talk about a cure for breast cancer any more than it makes sense to talk about a 'cure for cancer' (as in generic cancer). We have some hope for groups in small subsets with very speciic presentations but I don't think that even takes us closer to cures for others - each one has to be painstakingly broken down and the pathways sorted. Given how much variability and how many genes are involved, I don't think it's a simple plan at all. -
Dr. Winer is one of the best MO. He is my friend's MO and he was not taking new patients when I tried.
-
Yes, Lily, I searched him on YouTube and saw him speak in a few videos, he seems very caring as well as smart
-
Dear Olma, yes, I have seen that presentation and have these slides:)P BTW, I have also posted the trial Dana Farber is designing for a HER2+ mbc CURE - but no one reacted:) That comes from SABCS'20. Reposting:) People... there are cures in stage IV already, just they are not proved - time is needed. Drugs are super effective already, now they have to be used wisely and first "official" cures will come... Saulius

-
I have an odd question: Early on (2017-2018), when I was on Ibrance/Faslodex, I recall that the folks on the Ibrance string were mentioning/quoting a revered oncologist whose name was "Saulius" or at least something close thereto. Is that you, Saulius, or am I just totally misremembering? I lost sight of that onc visionary and would love to be reminded of whom he(?) was, anyway. Thanks!!
All of this makes me wish I were HER2+ (I guess)!
-
very interesting! Thanks, Saulius. Looks like they would hit the cancer with three systemic therapies, then local, then another systemic. Would they recruit only oligo patients or include those with more widespread mets?
Moth, unfortunately, made a good point. HER2+ is only 20 - 25% of all breast cancer and then metastatic fewer than that and de novo an even smaller subset.
Although anti HER2 therapy has proved useful for a few other cancer types, such as gastric, and now the HER2 low breast cancer studies...I think the original hope was that it would be more widely useful when the HER2 growth factor was first discovered.
But “ precision medicine “. does seem to be the answer, even though we hear frequently about research that could lead to THE cure for all cancer, nothing ever happens. Like that story from Israel a year or two ago and alsoimmunotherapy . Just saw this one the other day, hope it progresses beyond mouse studies - https://medicalxpress.com/news/2021-05-immunotherapy-revolutionize-cancer-treatment.html
-
And on the topic of further personalizing breast cancer treatment, here is a discussion of exactly that. Creating smaller sub-categories based on mutations other than just hormone receptors or lack thereof -
-
Thanks for this Olma...an interesting read.
-
Olma - thank you for the link. Genetics seems to be the key if we can just learn the markers and targeted therapy. Several years ago when I was sharing my experience with DIY cold capping and how it worked ( how to rotate the caps in the cooler etc) she remarked that she that I was lucky being strongly ER+ and that there were drugs, but she was triple negative with no drugs to treat it. I did not say anything, but I did not feel lucky since estrogen is natural and neccesary even in small amounts after menopause. I wish for ways to attack the cancer without attacking me. This is the 3rd recurrence. Tamoxifen, AIs are all systemic. Do they really work? Would I be much worse off without them?
-
Bluegirlredstate
I love the way you said “I wish for ways to attack the cancer without attacking me.“
the truth about anti-estrogens is how much they wreck our bodies- osteopenia, joint degeneration, muscle aches, heart health, dryness-skin, eyes, vaginal etc. we suffer through because they often work.
I am a little miffed when someone said, “at least it’s not chemo.” Yes-I do get to keep my hair and avoid some of the very harsh SE but hormone therapy takes a toll too. It’s not fun to have a golf ball size tumor in my liver, but I am thankful that my trial drug is working to keep the tumors from growing for now.
Dee
-
Youre welcome ladies, glad you found the articles useful. Quick comment about hormone therapies- I started feeling worse when I began the anastrozole than I did for my six months on Taxol, Herceptin and Perjeta. And, I quickly put on weight in my midsection.
I joke that the steroids in the Taxol infusion had me sohyped up so I “thought" I felt good...but seriously I was a fortunate one who didn't suffer that much on Taxol.
Yes, hated the baldness and I did have fatigue and low Hgb. But..the anastrozole has me fatigued, achy, makes my hands almost useless at times, muscle cramping especially at bed time, etc.
Tamoxifen carries a risk of uterine cancer, etc.
Sure, taking a pill every day is easier than showing up for infusions, but it's still a systemic therapy that effects our entire bodies.
If or when they perfect an immuno therapy that is a one shot deal, doesn't kill us and worksfor most or all of us — well, now, that will really be an achievement
-
Not “breaking research” but the history of the Warburg affect on cancer cells. I read about this nearly four years ago when I was first diagnosed with stage 4 and have been on a keto regime ever since. I started a thread about keto on the site a while back with links to other sites and info if anyone is interested.
https://www.reddit.com/r/ketoscience/comments/nto84d/cbs_this_morning_on_twitter_talks_about_otto/?utm_source=share&utm_medium=ios_app&utm_name=iossmf -
Dear JoynerL, I am not an oncologist - just an ordinary guy from Lithuania who's trying to save his wife. But you know... if I could live my life again (I am not that old- maybe there's still time?:), I could be an oncologist-researcher - what an exciting (and horrible) field. Let's hope it will turn from "horrible" into "exciting-only" soon.
Dear Olma, I am sorry I mostly post on HER2+ MBC because this is the field that is most important to my family. One thing I have to note is that HER2+ drugs (ADCs) are quite quickly making it into HER2low, as they get bystander/pan-inibitor properties. I think in a long term Her2low people will benefit from these drugs, and therefore Her2+ field is so exciting. There are stage IV people already in these threads who got NED on anti-her2 drugs, themselves being her2low (but having her2 mutation).
Saulius
-
Dear Saulius, please don’t apologize, your posts are very helpful and full of good information. And yes, you stay so well informed that you do sound like an oncologist! I am a HER2+ gal also - so all HER2 positive posts are of interest to me. Just the fact that the experts will discuss treating any of us with curative intent is very exciting. I wonder if the Dana Farber study has begun? I see Dr Winer mentioned the 77 patients, it seems to be referring to the planned study on the slide you posted
Kanga_Roo - interesting article. I just happened to come across this paper a few days ago “Hyperglycemic Conditions Proliferate Triple Negative Breast Cancer”
https://www.researchsquare.com/article/rs-520490/v1
It’s a preprint so not peer reviewed yet and it’s just about cells in a Petrie dish but still interesting.
-
Dear Olma, thanks a lot for your kind words. It'd be absolutely great if anyone who "attends" Dana Farber, or anyone in Boston, or Massachusetts, or even USA, could ask what is the state of that "possible" trial or trials similar like these? Of course, usually I wait for half a year/one year after something was announced I write and ask. I wrote really to quite a few top oncologists around the world and, to my surprise, got every and each answer. Extremely kind and understanding people. As close to top developments as one can get - trial and clinic wise. Just give them concrete questions, and you'll get all your answers. So dr. Parsons and dr. Lin, you still have half a year until Saulius' letter comes!:)
-
Saulius,
I have to echo what you've said. I've sent questions to a number of docs and they do respond, especially if you send very specific questions. They have always been kind.
And I do have to laugh about when your next few letters will be going out!
-
Phase 3 trial: ultra high single dose radiation was superior to 3 SBRT tx for oligomets
https://doi.org/10.1016/j.ijrobp.2021.01.004
edit: oops ok for reasons I don't understand I can't get the link to work but I think if you copy & paste this into a browser it should work redjournal.org/article/S0360-3016(21)00006-7/fulltext
"The study confirms SDRT as a superior ablative treatment, indicating that effective ablation of oligometastatic lesions is associated with significant mitigation of distant metastatic progression."
-
Moth, sounds like a good finding but I think the link is off somehow unless I’m the problem, which is entirely possible, lol. Would you mind checking, if you have time?
-
argh, I fought with that link 3 times and thought I'd outsmarted it with the DOI link instead but I guess not!
I'm editing it now one more time...
-
Thanks Bev, it is very nice to see you back here!:) Also, an ASCO summary on her2 ADCs in trials for her2low - looks very very promising! Saulius

-
That's great news for those with HER2-low MBC. The drug SYD 985 ( trastuzumab duocarmazine)already finished phase 3 trials for HER2+ (not low)and should be coming to market soon.
-
"Tamoxifen treated BC patients showed a reduced rate of hospitalization and strikingly no fatalities for COVID-19. In vitro experiments confirmed a protective role of tamoxifen while an increased susceptibility to SARS-CoV-2 infection of ER+ cells treated with fulvestrant was observed".
-
Olma61 - I loved the video about bones. I was so encouraged that I stopped by the gym on the way home to lift weights. I’m also increasing my walking. Thank you!
-
Oh, you’re very welcome! Happy to see this,
-
Olma61 and GoKale3420, which video is the bones video? Can't find it.
-
The link I posted was actually in the Bone Mets thread under Stage IV - here's the link on YouTube, might also be on lbbc.org
-
Thanks for Sharing that bone info. That was really educational and helpfu
-
YW and yes, I thought it was so comprehensive, whether for newly diagnosed or or “seasoned” metsters.
By the way, have not seen Lumpie, the OP of this thread posting lately and her last activity shows as May 7th. Hope she is okay, does anyone know her
-
Lumpie sometimes takes a breather for several weeks, just to recharge, so hopefully that’s what’s going on.
-
Lumpie, we appreciate you and this super-valuable thread!! Love to you!
-
You are so kind to be concerned. Doing ok here! Taking a bit of a breather, visiting some fully vaccinated family at long last, stopping off for some R&R and doing advocacy around access to health care. Plus sometimes I just get in a rut and feel like I read the same studies over and over ... you probably know what I mean ... though I did see something a couple of days ago I thought I should post. As soon as I find it among my billion emails, I will pass it along. Thanks, all! Take care and be well. -Lumpie
-
Glad you popped in Lumpie. I really appreciate this thread. Glad you are out there living life!
-
Yes, good to hear from you! Enjoy th well-deserved R and R , thanks for checking in
. -
Consequences of DDT Exposure Could Last Generations
DDT continues to haunt human bodies. In earlier studies, she found that the daughters of mothers exposed to the highest DDT levels while pregnant had elevated rates of breast cancer, hypertension and obesity.
Cohn's newest study, on the exposed women's grandchildren, documents the first evidence that DDT's health effects can persist for at least three generations. The study linked grandmothers' higher DDT exposure rates to granddaughters' higher body mass index (BMI) and earlier first menstruation, both of which can signal future health issues.
Nice synopsis here: https://www.phi.org/press/consequences-of-ddt-expo...
Read the PHI press release on the study here.
{Study} ORIGINALLY PUBLISHED BY Scientific American
Also reported in Cancer Epidemiology, Biomarkers, and Prevention
https://cebp.aacrjournals.org/content/early/2021/0...
DOI: 10.1158/1055-9965.EPI-20-1456
{Journal article requires subscription or fee. Others should be accessable without charge.}
-
New study will begin enrolling third quarter of 2021 - for Metastatic Triple Neg
testing Agents to boost Trodelvy action
Open label Phase 1b/2
"Open-label Phase 1b/2 study will evaluate the safety and preliminary efficacy of Anktiva (N-803) and PD-L1 t-haNK in combination with antibody-drug conjugate Trodelvy and low-dose chemotherapy in subjects with advanced triple-negative breast cancer (TNBC) after prior therapy"
-
Study finds breast cancer's response to tumor stiffness may predict bone metastasis
Tumor stiffening, which develops as diseased breast tissue becomes fibrotic, plays a major role in how breast cancer cells spread throughout the body. The paper, "Breast tumor stiffness instructs bone metastasis via maintenance of mechanical conditioning," published today in the journal Cell Reports, found that the stiffness of the breast tumor microenvironment can cause changes to cancer cells that make them more aggressively spread to the bone. The resulting changes are maintained as "mechanical memory," which instructs the cancer cells to send signals that lead to the breakdown of bone. Once this happens, patients often suffer debilitating complications like spontaneous fractures...
The study, which is the first to demonstrate the concept of mechanical memory during cancer metastasis, developed a novel mechanical conditioning, or "MeCo," score, to quantify the cellular changes. Eventually, researchers hope the MeCo score can be used to help identify breast cancer patients who might benefit from repurposed antifibrotic treatments to prevent bone metastasis.
-
[Early research] New discovery could yield a potential new treatment for breast cancer
In a study published this month in Cell Reports, the team used small molecules known as peptides to disrupt a complex of two proteins, RBM39 and MLL1, that is found in breast cancer cells but not in normal cells.
The research team discovered that the abnormal interaction between RBM39 and MLL1 is required for breast cancer cells to multiply and survive. The team developed non-toxic peptides that prevent these proteins from interacting in breast cancer cells, disrupting their growth and survival.
https://www.news-medical.net/news/20210629/New-dis...
-
[Early research] RNA-binding proteins represent a new class of drug targets for triple-negative breast cancer
The researchers systematically silenced RNA-binding proteins in these cancer cells one-by-one using the CRISPR gene editing technique. They found 57 RNA-binding proteins that, when inhibited, kill cancer cells with the known hyperactive cancer-driver. The advantage of the synthetic lethal approach is that normal cells, which don't produce that cancer-driving molecule, should be left untouched by the treatment. Of these 57 RNA-binding proteins, YTHDF2 appeared most promising...
The researchers [got a] detailed look at how the various cells that make up a breast tumor behave without YTHDF2. The approach revealed that YTHDF2-deficient cancer cells die by stress-induced apoptosis, a carefully controlled mechanism cells use to destroy themselves. Apoptosis is supposed to shut down malfunctioning cells so tumors don't arise, but it doesn't always work. By removing YTHDF2, they managed to re-activate this cell death signal.
To test how safe it might be to treat cancer by inhibiting YTHDF2, the researchers engineered mice that lack YTHDF2 in every cell of the adult body, not just transplanted breast cancer cells. The mice appeared completely normal -- not only did they not have tumors, there were no changes in body weight or behavior.
-
ddebbew - I saw where RNA may help with cancer, I didn't see which kind. That's great news, now if it only helped ALL cancers
-
HomeMom,
I had the wrong link for the last article I posted. I've fixed it now. The testing was done on TN BC using human cells and mouse models. The study identified an RNA-binding protein which was needed for the cancer cells to survive but not needed by normal cells. The next step would be to target this protein with a drug.
ETA: Here's a more detailed article that came out today: https://www.genengnews.com/news/rna-binding-protei...
-
I found this article very interesting:
Seed and Soil: Tracing the Journey of Spreading Cancer Cells
-
Oral paclitaxel may still be a future option despite being denied FDA approval a few months ago. "The FDA was supportive and encouraged the Company to continue development of oral paclitaxel and encequidar for the treatment of metastatic breast cancer. The FDA also agreed that a well-designed and well-conducted trial may adequately address the deficiencies raised in the CRL." https://www.obroncology.com/news/athenex-provides-update-from-fda-type-a-meeting-regarding-oral-paclitaxel?ap=334&vhid=
Interesting article LIllyishere
-
-
COVID Vaccine Protects Cancer Patients -- Second Dose Key
— Study reinforces need to prioritize these patients for vaccination, authors say
MedPage Today July 8, 2021
The Pfizer-BioNTech mRNA COVID-19 vaccine achieved satisfactory levels of seropositivity in patients undergoing treatment for cancer, although protection occurred later compared with a healthy population, Israeli researchers found.
Just 29% of cancer patients were seropositive after the first dose of vaccine compared with 84% of controls, with median titer scores of 42.3 and 72.0, respectively. However, the seropositivity rate climbed to 86% among cancer patients after the second dose...
"Although the immunogenicity pattern was gradual and slower than in the noncancer population, after the second dose most patients were seropositive and no documented cases of COVID-19 infection were determined," they wrote in JAMA Oncology. "Our study lends credence to the widely adopted recommendation to prioritize patients with cancer for SARS-CoV-2 vaccination."
The objective of this study was to evaluate the serologic status and safety of the Pfizer-BioNTech vaccine in patients with solid tumors who were receiving active cancer treatments.
Types of treatment included chemotherapy (58%), biologic agents (35%), and immunotherapy (36%), with some patients receiving more than one type of treatment.
... patients with breast cancer comprised 29% of the seronegative group, and 74% of these patients were treated with chemotherapy, with treatments being diverse. "Hence, we cannot assume that a specific class of drugs may hamper immunogenicity but rather that lympho-suppressive agents may induce a lack of effective seroconversion,"
Any intention to forego a second vaccine dose in some jurisdictions because of a shortage of vaccines "warrants reevaluation of unique populations, such as patients with cancer, in view of lagging immunogenicity,"
Primary Source: JAMA Oncology
Reporting: https://www.medpagetoday.com/infectiousdisease/cov...
{Access to reporting should be free but may require registration. I was also able to access the full article without charge.}
-
First-Line Pertuzumab Plus Trastuzumab Plus a Taxane for HER2-Positive Locally Recurrent or Metastatic Breast Cancer
- Annals of Oncology In this multicenter, single-arm study, the authors evaluated the safety and efficacy of investigator-selected taxanes in combination with pertuzumab and trastuzumab for the management of HER2-positive, locally recurrent or metastatic breast cancer as first-line therapy. There was no difference in overall survival among taxanes, but patients treated with paclitaxel had fewer side effects compared with those treated with docetaxel or nab-paclitaxel. HR-positive disease was associated with improved outcomes; the presence of visceral disease was associated with poor outcomes.These results are consistent with the findings of the CLEOPATRA trial but expand the taxanes that can be effectively combined with trastuzumab and pertuzumab in HER2-positive breast cancer. Treatment with paclitaxel may result in less toxicity.CONCLUSIONS: Mature results from PERUSE show a safety and efficacy profile consistent with results from CLEOPATRA and median OS exceeding 5 years. Results suggest that paclitaxel is a valid alternative to docetaxel as backbone chemotherapy. Exploratory analyses suggest risk factors that could guide future trial design.
Source:Open Access Published: July 01, 2021 DOI:https://doi.org/10.1016/j.annonc.2021.06.024Reporting at: https://www.practiceupdate.com/c/120482/67/13/?els...{Access w/o charge.} -
great article about oligometastes and local treatment
https://ascopubs.org/doi/full/10.1200/JCO.21.00445
Oligometastases (<=5 lesions in one location) is getting more attention and guidelines.
The treatment of patients with oligometastatic disease is and must remain individualized and based on multidisciplinary decisions.
size could become part of the definition: metastatic lesions should be considered oligometastatic (ie, potentially eligible for local treatment) only when the size of the smallest lesion has reached a certain threshold, which could be proposed around 8-10 mm in diameter
Dee
-
Yes, this is good news, the more they consider making this standard treatment or at least, justifiable, the better.
I am disappointed that they ruled out oligoprogressive disease rather strongly - because I wasn’t oligo at diagnosis but I was oligoprogressive/persistent with one lesion under 10mm and did have local treatment which put me back to NED. And two years later I’m still NED.
Hopefully more research can justify local treatment for small instances of progression
-
Guys, from what I read and see around, de novo multiple involvement/progression in one organ might also be seen as oligo-disease, as usually these tumors, although abundant, are of a very uniform genomic setting and systemic treatments, if they work, they work for all tumors. So, this has nothing to do with local treatments, but with definitions of what oligo might be in the future. Maybe they will come up with another term too. Saulius
-
So, do I understand this correctly that they are defining oligometastic by diameter of lesion rather than length?
-
cowgal- If I understand the article, they are looking at the age of the tumors as represented by the tumor growth/size. The thought is if the smallest tumor is less than 8mm diameter it is not mature and there could be others lurking close by. If the smallest tumor is greater than 8mm then there is more confidence of oligometastes due to the tumor cell doubling time. Which would potentially qualify you for the local treatments. It's a bit confusing but still progress in some ways.
Olma was not in that parameter but responded. I was in that category but was refused surgery at MDACC -they insisted on a systemic working first. Can’t look back though
BSandra-good point.
Dee
-
cowgal, my understanding of lesion measurement from pathology peeps is that it is the longest cross section measurement. That's how they always report right now & that oligo editorial seemed to say the same thing. It's diameter in a round lesion but since most things are not perfectly round, it's longest x section...
It's an interesting article. It is an editorial, so it's an opinion, a guidance from some experts. I imagine others will disagree with definition parameters etc. and with the recommendations as a whole.
I think the idea of waiting until a lesion is a certain size to see if others crop up or whether it truly is oligo is interesting. I also noted down the tumor doubling times - they seemed higher than I've seen in past articles but I might have just jumbled up the numbers in my head.
There was also an interesting comment about thoracotomy finding more small lesions than thoracoscopy but that although the studies on superiority of one procedure over the other hadn't given OS results yet, they thought the removal of the small ones would not be beneficial.
I can see it's a big dilemma for oncologists and oncology surgeons now. If presented with a de novo pt, how aggressively do we cut?
I think we're missing a piece of the puzzle about overall tumor burden and overall inflammation... if reducing tumor burden drastically reduces inflammation then perhaps the next mets are more controlled (both by systemic treatments and by the pts own immune system) which should yield a longer OS.
& I did not like at all the dismissal of oligoprogression for a surgical approach. Booo, raspberries at the authors.
-
Moth, Dee, these articles never really explain how they define that something is oligo. What they want to say probably is that oligo-lesion is sort of in-situ metastatic tumor. But if it is not in-situ, then it is invasive, and even several mm can contribute to further spread (as also noted in the article), so I do not get the idea of "waiting". You notice a lesion that is 2 mm, and then wait until it is 8 mm, and then suddenly other 2 mm satellite lesions occur nearby because of that 8 mm lesion, and then you are like "you were curable 2 months ago but now, ups, you are incurable, sorry". Would it not be smarter to start asap with treatment of 2 mm lesion and then see if others pop-up? This way most more patients would be cured: those who are "oligo", and those who aren't "oligo" but whose tumor did not spread into surrounding environment. I never liked the "oligo" hypothesis. Too many flaws and no real criterion to define it. One of the flaws again is the denial of "oligo-progression". What if someone has achieved pCR in distant organs, and not in initial tumor (a few undetected cells left), and then initial tumor once again metastasizes with only few lesions in the beginning and they are detected? Saulius
-
Sailuis- I agree. The article doesn’t make clear on definitions or parameters for treatment, but does attempt to put oligo in the spot light. I like our discussion and it makes me wonder how the professionals are viewing this article.
BTW-I had oligo progression and had SBRT to a lung met that lit up on my PET while the liver was quiet. No more progression in the lung now.
Dee
-
You see, Dee, you are a real example. Now take the scenario if your lung nodule would have not been treated (I am pretty sure your lungs would have progressed more as that lesion came up being under treatment)... but it was treated and today we see that decision was absolutely correct, although according to oligo-hypothesis you did not fall into "oligo" a category and would have not qualified for local treatments. From what I read, whether lesions are 5, or 25, if the drug/local treatment works, they can be obliterated, so "oligo" (meaning "few") does not make sense, as well as waiting - not only primary tumor causes metastases but also metastatic tumors spread further, so why wait? Stage 3C (let's say it is some stage 3.5:) is curable in practice with multiple lymph node metastases and has survival rate of ~40% at 15 years, so maybe some stage 4 are also more like 3.8, and also are curable, therefore you cannot give up on any patient and curative strategies have to be in mind as much as possible. There might be a huge difference between, let's say, these two cases: case 1 - T4N3M1 with 3 genetically nonuniform metastatic lesions >1 cm in the liver, and case2 - T4N3M1 with 20 genetically uniform (for example, de novo) metastatic lesions <1 cm in the liver. Oligo theory says that case1 has more chances for a cure than case2, but actually there's no real evidence for that, as we do not know genomic arrangement of every lesion or micromet. Just remember - we usually biopsy 1 or 2, and then give treatments, and they don't work. Why? Most probably because disease is nonuniform, and remaining 3 mets have different genomic arrangement. Local treatments "do not care" of non-uniformity, and that is why they are amazing. Our immunologist said surgery lives its golden age - he said, if I recall correctly, Norwegians cyberknifed 120 metastases in one person's lung, and the person is alive and doing ok, so actually local treatment possibilities have a big future and some 20 lesions with image recognition and AI a few years ahead might be an "easy" surgery.
I also love these discussions but I think professionals would be reluctant to discuss such things - they are too afraid to be viewed as unprofessional!:) Saulius
-
Saulius- you have great thought provoking points! Cyberknife(SBRT) to 120 lesions😳. They must have been tiny.
My oligo story started with 2 liver tumors both 2mm and under so I qualified for liver surgery but they would have to take the whole right lobe. My local clinic was ready to proceed but I wanted a second opinion at MDACC. They said no due to potential micrometastisis. After 4 failed systemic treatments the 2 tumors turned in to 3 in both lobes with suspect tiny lesions. They would not do SBRT to my liver at MDACC because at the time lesions (4.5cm 3cm 2.5cm) would require too much radiation. but I did get the y90 to those. Unfortunately more tumors grew in the liver but Y90 bought me time to find a systemic that would work.
my local RO only allowed a few lung lesions that are less than 3cm because of the amount of radiation involved. My lung lesion was almost 2cm. Glad it’s dead.
My current 2 larger liver lesions are heterogeneous and the larger one could use Y-90 or some other ablation to whack-a-mole it down, reduce tumor burden etc. but I am on a trial and they said no. I am going to push for it again if that tumor is wobbling in size while the other one is shrinking. Scan & plan Aug 9.
So you can see why oligo articles interest me 😉
Dee
-
Great analysis, guys! Interesting discussion
-
Moving Away From the Maximum Tolerated Dose
The FDA recently expressed a new commitment to testing cancer drugs at lower doses, rather than defaulting to the highest dose most people can tolerate.
CANCER DRUGS ARE ROUTINELY tested and approved for use at the maximum tolerated dose (MTD), which is defined as the highest dose most people can take without experiencing unacceptable side effects. But the MTD may not be the right dose for every cancer patient, especially if side effects and toxicity associated with cancer treatment can cause a person to stop taking the drug altogether.
To minimize the negative side effects of cancer treatment, Winer and colleagues published guidance for conducting dose de-escalation studies in the Dec. 1, 2020, Journal of Clinical Oncology. The roadmap is intended to describe how to better design and implement clinical trials to study lower drug dosages—without compromising the clinical benefit to the patient.
https://www.cancertodaymag.org/Pages/cancer-talk/M...
{No charge, and I was not required to log in, to read coverage article.}
Article contains a number of links to additional articles/coverage of the topic.
There was a report on the MBC Patient Survey at the American Society of Clinical Oncology's (ASCO's) annual worldwide meeting. You can read about it here in Medicine Matters / Oncology.
The PCDI will be talking about the results of both the Patient and Oncologists Surveys at a complimentary SHARE Cancer Support presentation on June 28, 2021 at 3PM ET, so if you're interested, please register. {No charge.}
-
Dear Dee, wow, I cannot believe MDACC said no to surgery. Potential micromets, I understand, but still... crazy... Saulius
-
https://news.illinois.edu/view/6367/339688859
New approach eradicates breast cancer in mice
Researchers discovered a small molecule, ErSO, that eradicates breast cancers in mice by targeting a pathway that protects cancer cells. -
CP418 - Wow, great article! I would love to sign up for a clinical trial.
-
https://www.biospace.com/article/releases/bayer-an...
I did a quick online search for more information about the ErSO therapy that CP418 posted about, and I found the article (link above). The research team and Bayer Company have agreed to work together on this.
-
Sounds very interesting but the BBC article I saw on it said that if it all goes well, it should be available in a DECADE!!! Seriously?! Why should it have to take that long when they got a vaccine for a novel coronavirus out in under a year. Why cant they move it along faster and let those with no other options to take a chance on it? the covid vaccine got an emergency approval. Couldnt they do that with a cancer treatment like this?
-
I saw the BBC article on ErSO and it said that if all goes well, it will be available in a DECADE!!! Serioulsy??!! Why should it have to take that long? They got the vaccine for a novel coronavirus out in under a year. Could they give this cancer treatment an emergency approval like they did for the vaccine? Let people who have no other options take a chance at it.
-
Here is a Study published November 2020 highlighting the benefits of high dose IV Vitamin C (1g/kg = 50g) twice weekly during radiation. Not to be confused with vitamin C supplements. At high IV levels, C becomes oxidative which cancer cells cannot handle. In this study, high IV-C significantly reduced NLR/systemic inflammation from radiation treatment. Enormous boost to the immune system. I had IV-C twice weekly throughout my cancer treatment, and will gladly continue it through radiation. It takes 1.5 hours while you watch a movie, nap or listen to music. I considered those my "spa days." - Esther
Observational Study J Altern Complement Med . 2020 Nov;26(11):1039-1046. doi: 10.1089/acm.2020.0138. Epub 2020 Sep 1.The Effect of High Dose Intravenous Vitamin C During Radiotherapy on Breast Cancer Patients' Neutrophil-Lymphocyte Ratio
Hyunwoo Park 1 , Jihun Kang 1 , Jongsoon Choi 1 , Somi Heo 2 , Duk-Hee Lee 2Affiliations
- PMID: 32876471
- DOI: 10.1089/acm.2020.0138
Abstract
Background: Breast cancer is very common, and the incidence is growing every year. Most breast cancers are treated with radiation after surgery. As a side effect of radiation therapy, inflammation, as well as the neutrophil-lymphocyte ratio (NLR), level increases. However, high NLR levels act as independent prognostic factors for increased mortality in all cancers. In this study, the authors investigated whether administration of vitamin C, which is effective in suppressing inflammation, may help to reduce high levels of NLR produced by radiation therapy. Methods: This study was performed retrospectively among 424 patients who were diagnosed with breast cancer and were treated with postoperative radiotherapy at Kosin University Gospel Hospital from January 2011 to December 2017. Among them, 354 patients received radiation therapy without vitamin C (the control group), and 70 experimental patients received vitamin C intravenously twice a week for at least 4 weeks during radiation therapy. The experimental group was divided into two groups according to the dose administrated: a low-dose vitamin C group (less than 1 g/kg, 52 patients) and a high-dose vitamin C group (more than 1 g/kg, 18 patients). The authors conducted three NLR measurements: before and after radiation therapy and at 3 months after radiation therapy; the authors then compared the change in NLR over time between the groups using repeated measures analysis of variance. Results: In the control group and the low-dose vitamin C-administered group, NLR was increased at the endpoint compared to before the radiotherapy, whereas NLR values in the high-dose vitamin C group were 8.4 ± 1.7, 5.9 ± 1.3, and 4.3 ± 1.5, showing a continuous decrease and a statistically significant difference (pinteraction = 0.033). These results were similarly observed in models adjusted by the patient's age and American Joint Committee on Cancer stage, with borderline significance (pinteraction = 0.065). Conclusions: Elevated NLR, a measure of systemic inflammation, has been associated with higher mortality cancer patients, including breast cancer patients. In this observational study, NLR was significantly decreased during radiation therapy in patients administered high-dose vitamin C.
Keywords: breast cancer; high-dose vitamin C; neutrophil–lymphocyte ratio; radiotherapy.
-------------------------------------------
P.S. A G6PD lab test (for G6PD deficiency which is rare) is performed before the first dose of IV Vitamin C and must be in normal in order to receive High Doses of IV Vitamin C.
-
Esther I did the same. Very glad I did it too.
Did it during chemo 2 x per week. I did not do it during rads but did it again post rads along combined with HBOT (hyperbaric oxygen) which makes the C even more pro-oxidant and also helps skin healing. I loved getting it during my chemo weeks because the fluids alone were a good boost. HBOT is also *very pleasant* as long as you aren't claustrophobic. I would drift off for a great nap. HBOT literally PUSHES oxygen into your bloodstream and you leave feeling normal/ way less anemic.
People interested in getting this therapy: you will need one blood test to make sure your body can handle the high dose of C. An Integrative Med Doctor can do it as well as give the C. It's expensive (~$200 a time where I live).
My MO was not enthusiastic... No double blind clinical trial, etc. (Though tons of clinical data.)
I said, "is there any *risk* to taking high dose IV C?" His reply: "needle sticks introduce a risk of infection." Sooooo yeah, since I was already a pincushion, that was not a risk that dissuaded me. I had locally advanced TNBC and wanted to throw everything at it.
-
PS my N/L ratio stayed low during treatment I think it was apx 2 or 2.5 most of the time.
-
Regarding the oligo discussion, here’s a new video from Living Beyond Breast Cancer- two doctors discuss treatments and clinical trials they are doing for oligometastatic disease, what curative intent means, etc. I think at least one of them is at MD Anderson.
One thing that confused me was when they discussed size of lesions to be considered oligo - they said 5 to 7 centimeters...they must have slipped and meant to say millimeters, because 5 cm lesions aren’t “small” lesions as far as I know.
Anyway, these guys seem more conservative than the ones who wrote the article above, and they didn’t want to discuss oligo progression at all. They strictly study patients who are oligo at diagnosis. I’m not clear if they only recruit deNovo pts or if they include early stagers with spread. I’d need to watch again to have more clarity on details. The discussion of circulating tumor cell tests to detect mets, measure tumor burden etc, was interesting too.
-
Olma, Dr. Tripathy is at MDA (top right in video). In my experience so far, they’ve focused on oligo de novo. When I was diagnosed in late 2016, I participated in a CTC study of blood samples but I don’t know if there’s an outcome yet. And I’m not sure about the tumor sizing but I know my bone met was 1.3x1 cm.
-
Olma, thanks for sharing the link. I believe 5 cm is correct for organs, I heard this number in one of the events held by an expensive-private clinic near where I live. And also there is another category for oligo metastatic, when there are 2 or 3 locations in total 4-5 lesions, don't remember limitation of size of tumor. As the two doctors emphasized really depends on the studies' objectives the oligo metastatic term has different definitions. I really hope that they invest/ do more research on this topic.
-
Olma, Great research and discussion!
And thanks, Santa Barbarian, I had heard about that and will try the hyperbaric oxygen therapy.
Blessings
Esther
-
Glad you ladies have found value in this discussion. Thanks to Alabama Dee also for starting it off.
Snow-drop, thanks for that input! And yes, it is interesting how all the different oligotrials have different design.
I am really, really thankful to my MO for thinking outside the box and referring me for rads on my spine, seeing how these researchers think there is not really evidence for it o someone like me
As she said, it's practicing the art of medicine, rather than being too strict about the science.
-
olma- I found that video very VERY interesting. Thanks for posting it. Both DRs said systemic first to see if it was truly oligo.This validates my treatment. Even though they seem to have de novo as the focus, I heard some reoccurrence discussion too. Mine came back 5 years after original treatment.
My MDACC surgeon said no until I had a systemic working at least stable disease and preferably some shrinkage. if I had the whole right liver lobe removed, the regenerative and healing process without any systemic could cause the probable micromets to explode and the surgery would have been more harmful than good. The video talked about risk/benefit like this.
HOWEVER, MDACC offered me an in-house random clinical trial on SBRT vs systemic. That did not track with their talk on the video. I declined because I wanted to still go for surgery at that time and I did not want to take the risk of micromets growing with no systemic.ALSO, I also had 2 blood biopsies while on treatment at MDACC with 0 result and the tumors were growing/ multiplying. That science needs some more time to improve like they said in the video.
They only hinted at using local therapy to slow down progression and give longer lifespan and better quality of life. No one mentioned local therapy on oligo to reduce tumor burden (that’s what I did with y-90)
I hope this area of treating oligo aggressively for curative intent and what that really means, gets more traction.
Both DRs insisted that more research is needed (ie clinical trials) to gather statistics. Meanwhile I’m glad some of our docs agreed to think outside the box and get us some local therapy that seems to be helping us. Anecdotal data here on this site is how I have educated myself and pushed for local treatments
Dee
-
gals, gals, FINALLY something about polymetastatic disease!!!
This was a pre-phase 1 trial of what I think is mapping out essentially SABR dose escalation for polymetastatic disease
www.advancesradonc.org/article/S2452-1094(21)00092-0/fulltext
(trying url again. if I make it clickable it doesn't work so you're going to have to cut/paste)
-
(xposted to mTNBC thread(
Keynote 355 Phase 3 clinical trial reports: IMPROVED OS with pembrolizumab (Keytruda) for mTNBC w. PD-L1 >10
details re OS to come at a medical meeting so we don't know how big an effect it has but it reached statistical significance & was clinically meaningful.
-
Good one, moth! Thank
-
one for early stage high risk TNBC
FDA approves pembrolizumab for pts with high-risk early stage TNBC based on DFS improvement seen in KN-522
https://www.merck.com/news/fda-approves-keytruda-p...
-
Duration of Adjuvant Aromatase-Inhibitor Therapy in Postmenopausal Breast Cancer https://www.nejm.org/doi/full/10.1056/NEJMoa2104162
CONCLUSIONS: In postmenopausal women with hormone-receptor–positive breast cancer who had received 5 years of adjuvant endocrine therapy, extending hormone therapy by 5 years provided no benefit over a 2-year extension but was associated with a greater risk of bone fracture.
-
Lilyishere- I saw that one and thought it was quite interesting. I lasted 4 1/2 years on the AI’s just couldn’t take the SEs anymore. Became metastatic a year later
Here is another summary report of er targeting trials
Dee
-
Researchers Identify Biomarker to Predict Immunotherapy Response in Patients With Breast Cancer
The Major Histocompatibility Complex Class II protein has potential to predict immunotherapy benefit in two types of breast cancer.
Needs large Phase 3 trial to confirm
https://www.curetoday.com/view/researchers-identif...
-
Has anyone here with ER PR + stopped taking the drug Arimidex after 7 years? If so what was your node involvement? Two years ago my MO told me about thise study https://www.breastcancer.org/research-news/5-more-years-of-ais-no-better-than-2-more so we agreed to go two more years making it 7 years of medication. December will be 7 years. The conversation we had on Monday at my 6 month appt was that she wanted me to get a bone density scan and that would determine if we kept going on the arimidex. If I had issues, we would stop it was my guess since it eats at your bones.
I get a call today that I have Osteopenia. I talked to the PA and she said my doctor wants me to go another 3 years on the arimidex and take the Prolia shot every 6 months! I've always been told that with grade 1 I had a cancer that was not aggressive and chemo was an "insurance policy". Now the PA is telling me I am at more high risk because I had node involvement and the 7 years is for people who have no node involvement. My MO has never told me this in the conversations we had about stopping the medication. I'm not sure what I want to do to be honest. I'm disappointed because I was ready to stop with the meds that have my hair thinning, the fat is harder to lose and my vajay jayay is a desert!
-
HomeMome, I think it's reasonable to ask to see the MO and find out from them what numbers they're looking at and how they're assessing your risk.
The study that looked at stopping at 5 years showed that risk for HR+ continues into the 20 year event horizon and the number of lymph nodes is relevant. The blue line is 1-3 positive nodes. But you've already done two extra years ... I suspect this is an area where there's a lot of uncertainty still. https://www.nejm.org/doi/full/10.1056/NEJMoa170183...

-
AlabamaDee, I hope you are not feeling guilty about stopping AI at 4.5 months. AI can reduce the recurrence up to 50% and from this forum, so many women had recurrences while using tamoxifen or AI. These medications are keeping the cancer cells without their fuel to multiply but obviously, in more than 50% of cases are not killing them. In the best case senario, when the time comes to stop AI, cancer cells can be still "sleeping" or can start multiplying. It is a gamble we are all playing with our lives.
-
Moth - thank you for that. So those numbers are if you stop at 5 years, not if you continue to 7-10 years? I read everything and it was a little confusing. The PA just mentioned my node involvement. She said 7 years was for early stage only. Hello? I was early stage.
I read it over again. If I read it correctly, those numbers are only if you stop after 5 years. Correct me if I'm wrong. I'm starting to lean towards taking it another 3 years!
-
Homemom- the latest report is being repeated on cancer social media. Lillyishere listed it above.
“In postmenopausal women with hormone-receptor–positive breast cancer who had received 5 years of adjuvant endocrine therapy, extending hormone therapy by 5 years provided no benefit over a 2-year extension but was associated with a greater risk of bone fracture.“
You and your MO should talk about this article when making the decision. BTW I am osteopenic but cannot take bisphosphonates like prolia. My MO is happy to keep my vitamin D above 60 and increase weight bearing exercise. Bone density again in 2 years.
Lilyishere - quitting my AI at 4.5 years was probably not the issue since my MBC has the esr1 mutation the AI probably quit working.
Dee
-
AlabamaDee - Thank you, I didn't see that since it was before my post. Looks like extending to 10 years still doesn't help more than 7 years, but that study doesn't go into detail like Moth's link does. I wish one would show both. I will have questions when they call back next week
-
just to go further on AlabamaDee's post, Prolia is not a bisphosphonate, it is a monoclonal antibody. Zometa however is a bisphosphonate & it too is often used to boost bone density.
-
HomeMom, the new study is here https://www.nejm.org/doi/full/10.1056/NEJMoa210416...
I think this is the one you should discuss with your MO and see if it applies to you. The preview doesn't give important details about the node status and how it affected the results. I can't even see if they considered only node neg pts in their study population
-
Moth - so no study anywhere shows benefit for extending 5 years rather than 2. As a matter of fact, we have studies that show it increased possibility of bone fractures. I'm guessing that is why she wants me back on prolia. So three more years of Arimidex and Prolia, she thinks it will significantly decrease my chances of recurrence and protect my bones at the same time. I wonder if there is anything dertimental to doing that? I mean none of the studies suggest that anyone took a bone density drug along with the additional AI
Love this message board by the way!
-
moth- thanks for the clarification on prolia. It has the same SE of potentialosteonecrosis of the jaw as the bisphosphonates so I lumped them together. I have had 5 root canals and 2 apico surgeries. I can’t risk jawbone issues. Hopefully my bone density won’t drop too fast on my trial drug.
Dee
-
Important info for LOW ER+
from tweet by Dr Paolo Tarantino
"comparable outcomes b/w early TNBC and "ER-low" BC
Coherent with the recent EJC paper by Villegas et al. - showing that nearly 90% of "ER-low" cancers are basal-like tumors, behaving as TNBC"
Paper he's referring to:
"Impact of estrogen receptor levels on outcome in nonmetastatic triple negative breast cancer patients treated with neoadjuvant/adjuvant chemotherapy" https://www.nature.com/articles/s41523-021-00308-7...
"In conclusion, primary BC with ER1–9% shows similar clinical behavior to ER 1% BC. Our results suggest the use of a 10% cut-off, rather than <1%, to define triple-negative BC."
and
"the St. Gallen Consensus 2015 reported that ER expression values between 1 and 9% should be considered equivocal and that endocrine treatment alone, in the absence of chemotherapy, should not be considered a reliable adjuvant treatment for these patients."
I think the Villegas et al article he's referring to might be this one or one based on same research. I can't find an EJC version... https://cancerres.aacrjournals.org/content/79/4_Su...
bottom line seems to be that low ER might act really be much more like TN than we thought
-
Here's a blog post about ErSO that I think gives some context:
https://blogs.sciencemag.org/pipeline/archives/202...
-
ASCO treatment update for HER2- metastatic breast cancer
"Chemotherapy and Targeted Therapy for Patients With Human Epidermal Growth Factor Receptor 2–Negative Metastatic Breast Cancer That is Either Endocrine-Pretreated or Hormone Receptor–Negative: ASCO Guideline Update"
https://ascopubs.org/doi/full/10.1200/JCO.21.01374...
-
hi everybody. I need your help: my daughter, dx triple positive in 2015, has been taking tam for four years altogether with an interruption bc of having a baby...
She has tremendous problems with tam and would like to know how long yet.
I remember reading a study here on this thread that found out there was no further benefit after 5 years IF ER positive PLUS Her2 positive. I've been searching the net for hours now but cannot find it.
Does anyone of you ladies have an idea? Would be so grateful and thx in advance.
-
Apologies if this is old news. I was asked to participate in a research study, and I agreed and all it took was a blood sample. Apparently, researchers believe they have identified the genetic marker which would indicate breast cancer and could be detected in a blood sample. This would negate the need for a biopsy. I signed up without hesitation - I'm tired of the "death by a thousand cuts" process. It's called the Toray 3D-Gene Protocol: Study Sample Collection Protocol for "Analysis by EarlyGuard" of Serum miRNA from women referred for additional testing due to abnormal breast imaging classified as BI-RADS 3, 4, or 5." Fingers crossed it is successful - it'd be huge to avoid unnecessary biopsies and get to positives more widely/quickly/cheaply.
-
PinkTonic It should be on the page previous to this one (92? or 91?) I was in that discussion, but you should read the posts, I don't remember what was said about HER+ patients
My doctor thinks I need to stay on them another three years (I've been on 7) because I had node involvement. They sent me this study from New England Journal Of Medicine from a Canadian study https://www.nejm.org/doi/full/10.1056/NEJMoa1604700
I'm in the middle of reading it, but if anyone else wants to take a look and interpet what it says, be my guest!
-
-
I tried to look up that clinical trial you mentioned above. I could only come up with two clincial trials and one has been completed and the other suspended. Here are the two ClinicalTrials.gov Identifiers: NCT02127073 & NCT01231386. One was run out of Columbia University in NYC, and the other City of Hope on California. Do you know if it is one of these?
Thanks.
-
ARV471 Trial scan and plan on Monday. If all is good we move scan to every 12 weeks. Still going every other week for bloodwork. I am hopeful for a good report on the cancer, but dealing with UTI, migraines, vertigo and random pains. My step mom moved to a hospice house for pancreatic cancer. It was hard to deal with my emotions for her and my thoughts of an eminent future for me. Needless to say I am dealing with the usual scanxiety. Will let you all know the results. 🙏🏻🦋
Dee
Edited-Oops I meant to put this on clinical trials thread. Cross posting there.
-
Dee,
Thinking of you and hoping that all goes well on Monday. Thoughts for your step mom as well.
-
Alabama - thoughts are with you and that things go well next week for you, family, and friends
-
AlabamaDee - here I've been bellyaching about taking a pill another three years, and you have a very important date on Monday! I'll be thinking of you Monday, hoping you get the best results for less scans in your future!
-
Can Statins Extend Survival in Women With TNBC?
— Link with improved outcomes could have important public health implications, authors say
For women with triple-negative breast cancer (TNBC), using statins was associated with improved oncologic outcomes, according to results from a retrospective study.
Women who initiated statin use in the 12 months after a TNBC diagnosis had a 58% relative improvement in breast cancer-specific survival (BCSS; standardized HR 0.42, 95% CI 0.20-0.88, P=0.022) and a 30% relative improvement in overall survival (OS; standardized HR 0.70, 95% CI 0.50-0.99, P=0.046), reported Kevin Nead, MD, MPhil, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues in the journal Cancer.
When we looked at women without triple-negative disease, "there is absolutely no benefit, or even a hint of a benefit," in regards to BCSS (standardized HR 0.99, 95% CI 0.71-1.39, P=0.97) or OS (standardized HR 1.04, 95% CI 0.92-1.17, P=0.55), Nead told MedPage Today.
"It is important to acknowledge that this study is retrospective," he noted. "But I think this paper makes a strong case that the opportunity to help women with breast cancer by using statins is in those with triple-negative breast cancer, and I think it makes sense, as the next step, to work toward conducting a prospective trial."
There have been numerous studies looking at the association between statin use and breast cancer, with inconsistent results, the authors noted.
There is good biologic evidence that statins decrease breast cancer cell proliferation and increase apoptosis, and they can target key TNBC-associated pathways and can act synergistically with some existing therapies, they observed.
"Given the limited toxicity profile, low cost, and ease of use, an association between statin therapy and improved breast cancer outcomes, particularly in aggressive breast cancer subtypes, could have important public health implications,"...
Read the full new coverage article here:
https://www.medpagetoday.com/hematologyoncology/br...
Journal DOI: https://doi.org/10.1002/cncr.33797
{No charge but registration may be required. Journal article abstract available w/o charge, full article require a subscription or fee. }
-
Can someone explain the mumbo jumbo like this? (BCSS; standardized HR 0.42, 95% CI 0.20-0.88, P=0.022)
-
I don't know wht the BCSS is - I would need more context for that.
The other terms are from stats.
HR is hazard ratio
CI is confidence interval
P value is a complex thing but it's getting at how likely the result is to be random chance. Generally speaking, the smaller the P value, the better.
There are some good youtube videos just introducing medical stats. Here's one if you want to get the basics- it doesn't go over how to calculate anything, just what the results might mean.
-
I believe BCSS is “breast cancer-specific survival" i.e. percentage of people who don't die of breast cancer
-
ah that makes sense! thanks Pi-Xi!
-
Thanks moth, that is helpful
-
AlabamaDee: I'll pop in for an update. I hope it will all be good for you!!
-
Elderberry thanks for checking!
Continued stable disease🎉🎉🎉 Breathing a sigh of relief! I started this trial in Dec 2020 so this is the longest I have been on any MBC drug. The shrinkage went from 11% to 9% from start of study, but they considerate that still stable. And for my history that really is great.
Hope this trial drug has great success and becomes a new alternative to faslodex. Pills are better than shots.
(Cross posting )Dee
-
AlabamaDee - Great news!

-
HomeMom,
Magic decoder ring!
HR is hazard ratio: a measure of an effect of an intervention on an outcome of interest over time.
CI is confidence interval: expresses the degree of uncertainty associated with a sample statistic.
P is probability: the level of marginal significance within a statistical hypothesis test, representing the probability of the occurrence of a given event.
This stuff is fairly technical. Readers can certainly delve into it if they want, but sometimes I actually edit that out... mentally or editorially.... on the theory that it is in the linked doc if someone wants more detail and to make the material more readable. If you are trying to get the *general concept,* and read this:
"Women who initiated statin use in the 12 months after a TNBC diagnosis had a 58% relative improvement in breast cancer-specific survival and a 30% relative improvement in overall survival."
you probably get the general idea which is that this is a pretty significant improvement.
Hope that is of some help.
-
AlabamaDee - That is wonderful news! So happy to hear it! and Cheers! to new drugs!
-
Oops! I had already started the statistics reply before I saw Moth's. Video link is handy. Thx.
-
Lumpie, thanks! I did just what you do, skip over the abbreviations in the parentheses. Moth's video was very good too. I had heard that statins help cancer patients, but I didn't recall that it was for bc patients with TNBC. That IS great news
-
Fauci: Booster Shots for Immunocompromised People in the Works
August 09, 2021The US government is working to make booster shots available for immunocompromised people "as quickly as possible," Anthony Fauci, the White House medical adviser, said Thursday.
Government health officials have said booster shots for the general population are not needed now, but the rise of the highly transmissible Delta variant has created new dangers for people with compromised immune systems, **such as those undergoing chemotherapy,** with HIV, or taking certain medications.
"It is extremely important for us to move to get those individuals their boosters, and we are now working on that and will make that be implemented as quickly as possible, because for us and for the individuals involved it is a very high priority," Fauci said in a news briefing at the White House.
CDC data shows that immunocompromised people make up 2.7% of the US population.
The Wall Street Journal reported Thursday that the FDA expects to have a strategy by early September on COVID-19 vaccine boosters, including decisions on which people should be prioritized.
The Biden administration is worried that certain groups could need a booster as soon as this month, such as people who are immunocompromised, over 65, or who got their vaccine during the early rollout in December and January, the Journal reported, citing unnamed people familiar with discussions within the agency.
Vaccine makers Moderna and Pfizer have said they think booster shots would be a good idea.
Moderna said this week that neutralizing antibodies generated by its vaccine against three variants of the virus that causes the disease waned substantially 6 months after the second dose. Because of this, the company expects an increase in breakthrough infections with a need for boosters before winter.
Pfizer said in July that data from a booster study showed that antibody levels jumped by 5 to 10 times after a third dose, as compared with the second dose months before. That finding indicated a need for booster shots, Pfizer said.
After meeting with Pfizer officials in July, the CDC and the FDA issued a joint statement that said those who have been fully vaccinated "do not need a booster shot at this time."
https://www.medscape.com/viewarticle/956246?src=mk...
{Free access.}
-
Share's recorded webinar, "Patient-Centered Dosing for Individuals with MBC" is now available for viewing.
Patient-Centered Dosing for Individuals with MBC
Join the Patient-Centered Dosing Initiative (PCDI)'s Dr. Aditya Bardia, medical oncologist at Massachusetts General Hospital (MGH) Cancer Center and Assistant Professor of Medicine at Harvard Medical School, and Anne Loeser, patient advocate, author of The Insider's Guide to Metastatic Breast Cancer, to discuss their work with patients and doctors to help select optimal treatment dosage for those living with MBC.
https://www.sharecancersupport.org/patient-centere...
@{Great topic and I so admire the work Anne Loeser has done. No charge to watch! @ 1 hour but platform allows pace control (slower/faster).}
More on the same topic here: https://www.cancertodaymag.org/Pages/cancer-talk/M...
{Free to access. May require registration.... but I don't think so.}
-
Survival Outcomes Among Patients with Metastatic Breast Cancer
Annals of Surgical Oncology March 2021 https://link.springer.com/epdf/10.1245/s10434-021-...
It's a review of SEER database (so de novo dx only) from 1988-2016. Shows improvement in survival during that time but still median OS 25mos, CSS 27 mos, with results varying widely based on tumor markers and number/location of metastatic sites.
results very similar results to Wang et al 2019
https://bmccancer.biomedcentral.com/articles/10.11...
-
Durability of Response to SARS-CoV-2 BNT162b2 Vaccination in Patients on Active Anticancer Treatment
August 11, 2021
"We recently reported initial findings from a prospective cohort study which evaluated the antispike (anti-S) IgG antibody response to the SARS-CoV-2 BNT162b2 messenger RNA (mRNA) vaccine (BioNTech-Pfizer) in patients with solid tumors on active anticancer treatment vs healthy controls.1 After a median of approximately 5.5 weeks from the second vaccine dose, 90% of the patients with cancer (90/102) and 100% of the healthy controls (78/78) were seropositive, and the median IgG titer in the patients was significantly lower than that in the controls..."
AMA Oncol. Published online August 11, 2021. doi:10.1001/jamaoncol.2021.4390
https://jamanetwork.com/journals/jamaoncology/full...
{No charge for abstract. I was able to down load the full article at no charge.}
-
moth - It just distresses me to the max that they can't do better for MBC. The funding, from what I hear, is just 10-20% of funds raised for breast cancer research. I give 2% of my commissions as a Realtor to Metavivor. It isn't going to make a huge difference, but holy crap, that study was depressing
-
Lumpie
Thanks for posting about durability of response. Since I am in active treatment and low immunities due to hypogammaglubulinemia I will qualify for the booster. The FDA vote is tomorrow.
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-07/07-COVID-Oliver-508.pdfI plan to get it, even though I had Covid, monoclonal antibody for it and the Pfizer vaccine- we can't be sure how much response my body produced. I would love to get tested tofind out.
Dee -
Another study showing survival benefit for lumpectomy over mastectomy in eligible stage 1-3 pts
https://www.mdpi.com/2072-6694/13/16/4044
-
Cancer Patients See Sustained Response to COVID Vaccine
— Most patients on active treatment remained seropositive at 4 months
Cancer patients on active treatment achieved sustained responses to the Pfizer/BioNTech COVID-19 vaccine, though at reduced antibody levels versus healthy controls, according to Israeli investigators.
After about 4 months from the second dose of Pfizer's mRNA vaccine (BNT162b2), 87% of solid tumor patients who had been on active treatment remained seropositive for SARS-CoV-2 antispike IgG antibodies, reported Salomon M. Stemmer, MD, of Rabin Medical Center of Beilinson Hospital in Israel, and colleagues, in a research letter in JAMA Oncology.
"Given the prevalence of breakthrough infections with the Delta variant, these declines may provide justification enough for some patients to pursue a third vaccine booster dose to boost protection," Parikh suggested. "It remains to be seen whether the booster dose could actually improve clinical outcomes, however, and thus clinical trials of the booster dose -- which are ongoing -- are eagerly anticipated."
Read medical news coverage of article at: https://www.medpagetoday.com/hematologyoncology/ot...
{This news seems mostly reassuring. News reporting, abstract and JAMA article all appear to allow free access.}
-
Just chipping in to say research from Edin Uni concurs as to efficacy of vaccine. Also it is very likely we will be offered a booster in the autumn.
-
Karen,
Supposedly the U.S. Food and Drug Administration will announce in a day or two that we can get a third booster shot. Can't wait to get in line, with this crazy virus.
-
Has anybody heard whether the booster has to be from the same company as the first two shots? In other words, if I had Moderna, can I get a booster from Pfizer when the time comes?
-
I wondered that too SP. I had the J&J shot.
-
Shetland I was told they are still figuring that part out.
-
FDA authorizes extra vaccine doses for immunocompromised patients to bolster protection against the coronavirus
The Food and Drug Administration action means additional shots might be available as soon as this weekend
The action by the Food and Drug Administration means that additional shots could be available as soon as this weekend for patients who have received organ transplants or have certain types of cancer or other illnesses.
The FDA decision updated the emergency use authorizations for the Pfizer-BioNTech and Moderna coronavirus vaccines to say an additional dose could be given to some immunocompromised individuals, specifically organ transplant recipients and others with similar levels of immune-system impairment. The agency did not give further details. The Johnson & Johnson vaccine was not included because there was not sufficient data on the issue, according to the agency.
https://www.washingtonpost.com/health/2021/08/12/b...
"The Washington Post is providing this important information about the coronavirus for free. For more free coverage of the coronavirus pandemic, sign up for our Coronavirus Updates newsletter where all stories are free to read."
{Article say that they don't yet have enough evidence on "mixing"/changing brands. There is a short film available, too. It is my understanding that clinical trials on "mixing"/changing brands are under-way.}
-
@moth, to me, that sounds like another study showing survival benefit for radiation over no radiation for early stage patients
-
"@moth, to me, that sounds like another study showing survival benefit for radiation over no radiation for early stage patients"
When they found micromets in my sentinel lymph node after my BMX they were like you don't need radiation but, we'll present it to the tumor board; they recommended Radiation. When I went in for a consult I was armed with all the studies that showed there's no benefit to Rads after Mastectomy with less than 4 lymph nodes involved. The RO was like no there are new studies showing great benefits to radiation after Mastectomy with any node involvement!
Long story short, I hope that Rads + Mastectomy is the winning ticket. 😀
-
In my case, the tumor board decided no radiation even though I had 2 positive nodes. I had two opinions from two large cancer centers and they all agreed on this. I really don't like it when science keep changing their recomendations.
-
Are micromets when it is just a "spec" in there? I had two fully involved and two with "a spec".
-
I read online that in a biopsy-
“Micrometastases are defined as clusters of cancer cells that are between 0.2 mm and 2.0 mm in diameter. Any smaller clusters are called isolated tumor cells.“
I had 1 micro metastasis in my sentinel lymph node confirmed by pathology after surgery. The surgeon took out 22 nodes because he “saw” cancer. I have suffered from chronic Lymphadema for 8 years now. Tumor board said no radiation.
Dee
-
https://jitc.bmj.com/content/jitc/9/8/e002597.full.pdf
Recommendations Summarized here-
---All pts with MBC should undergo comprehensive genomic profiling, including TMB+MSI
---To test for PDL1, prioritize extrahepatic sites or primary tumor
---PDL1 should not be performed on decalcified bone
my PDL1 was from the liver and negative. 🤔
Dee
-
good article makes tremendous sense! My current onc had my almost four yr old bone sample tested - PDL1 negative. Not sure what “decalcified bone” means, though.
Since I’ve never had breast surgery, I wonder if anything is left of the primary that could be tested
-
https://www.nytimes.com/2021/08/17/health/breast-c...
This Breast Cancer Gene Is Less Well Known, but Nearly as Dangerous
PALB2 is not as well known as BRCA, but mutations of the gene can raise a woman's risk for breast cancer almost as much.
-
This piece is full of info and, well, nearly overwhelming. Wow.
I read it earlier this am and then went back to look for it. And read it again.
Coincidentally, my search brought up this piece on the same topic from 2014! In the same paper!
Wonder how much info/data remains the same between then and now?
The 2014 piece reports: "Women with the PALB2 mutations were slightly more likely to have "triple negative" breast cancer — a form resistant to hormone treatment, more aggressive, and more likely to recur than other subtypes."
And "Over all, the researchers found, a PALB2 mutation carrier had a 35 percent chance of developing cancer by age 70. By comparison, women with BRCA1 mutations have a 50 percent to 70 percent chance of developing breast cancer by that age, and those with BRCA2 have a 40 percent to 60 percent chance. The lifetime risk for breast cancer in the general population is about 12 percent."
Still all the same?
-
Education Department Announces Automatic Debt Cancellation for Over 323,000 Disabled Borrowers
... the Department of Education has finally committed to providing automatic federal loan discharges to the hundreds of thousands of disabled borrowers who have been entitled to this relief for years, totaling more than $5.8 billion in discharges. This action is long overdue and will make a huge difference in the lives of these borrowers who have been trapped in unnecessary student debt.
We're also very encouraged to see that the Department of Education plans to pursue broader changes through its upcoming rulemaking, and we look forward to working with the Department through that process to eliminate the many barriers that keep borrowers with disabilities from receiving the relief they are entitled to under law.
In the upcoming rulemaking, we're hoping that the Department will commit to eliminating the three-year monitoring period that has prevented so many borrowers from getting much needed relief under the disability discharge program. In addition, we want to see the Department take this opportunity to expand the eligibility criteria for the program to better match the intent of the law, and to find other ways to identify borrowers who miss out on relief due to our Kafkaesque student loan system.
We look forward to the Department's implementation of these changes for disabled borrowers early this fall....
Source: email dated Aug 20, 2021 by Persis Yu, Director, Student Loan Borrower Assistance Project, National Consumer Law Center
Organization web site: www.nclc.org Relevant posts: https://www.nclc.org/?option=com_content&print=pri... and https://www.nclc.org/media-center/statement-in-res...
{Web site access is free of charge. This information will be relevant to those with metastatic breast cancer. An additional source of excellent information on financial, legal and practical issues related to breast cancer is https://triagecancer.org/ }
-
piqray data-
https://theoncologist.onlinelibrary.wiley.com/doi/10.1002/onco.13804
“Postadjustment, median PFS for patients treated with alpelisib in BYLieve was 7.3 versus 3.7 months in the real-world cohort, and 6-month PFS was 54.6% versus 40.1%, respectively.“
I hope this helps someone interested in recent data. I'm not eligible since Idon't have the mutation, but up to 40% of MBC patients have PIK3CA-mutated tumors.
Dee
-
High tumor mutation burden fails to predict immune checkpoint blockade response across all cancer types
"In cancer types that showed no relationship between CD8 T-cell levels and neoantigen load, such as breast cancer, prostate cancer, and glioma, TMB-H tumors failed to achieve a 20% ORR (ORR = 15.3%, 95% CI 9.2-23.4, P = 0.95), and exhibited a significantly lower ORR relative to TMB-L tumors (OR = 0.46, 95% CI 0.24-0.88, P = 0.02)"
https://doi.org/10.1016/j.annonc.2021.02.006
(edited to fix link, hopefully!)
-
'How Deeply Ignorant We Are' About Healthcare Pricing
The New York Times has built a database to make pricing information released under new U.S. transparency rules easier to use, and along the way revealed how hospitals charge vastly different prices for the same services.
Not all hospitals are complying with the new rule to publish the rates they negotiated with insurers, but the reporters compiled information from more than 60 hospitals that did publish, partnering with researchers from the University of Maryland-Baltimore County to turn the pricing files into a database.
They found that hospitals charge patients "wildly different amounts for the same basic services" like an x-ray or a pregnancy test.
They also found that insurers aren't always negotiating favorable rates for their customers: "In many cases, insured patients were getting prices that are higher than they would if they pretended to have no coverage at all," they wrote.
More patients have a reason to care when their insurance makes a bad deal, as high-deductible plans become increasingly popular, the Times reported. With these plans, patients could have to pay thousands of dollars before their coverage kicks in.
The reporters used patient bills involving rabies vaccine as examples. At Intermountain Medical Center in Utah, a child's dose of the two drugs to prevent rabies -- along with administration fees and ED usage charges -- cost $4,198 with Cigna; $3,704 for patients paying cash; $3,457 with Regence BlueCross BlueShield; and $1,284 for SelectHealth, which is owned by Intermountain.
In Florida, an adult dose of a rabies shot at AdventHealth Orlando ranged from $17,000 to $37,000, not including ED usage fees.
"It's not just individual patients who are in the dark," Martin Gaynor, PhD, a healthcare economist from Carnegie Mellon, told the Times. "Employers are in the dark. Governments are in the dark. It's just astonishing how deeply ignorant we are about these prices."
Source: MedPage Today https://www.medpagetoday.com/special-reports/exclu...
Link to database: https://www.nytimes.com/interactive/2021/08/22/ups...
{MedPage is free of charge but may require registration. NYT may require a subscription - not sure. This is disillusioning - but no surprise at all. We all need to be talking with our legislators IMO about a health care system that is more affordable and accessible when we need it!}
-
Big development re TECENTRIQ/atezolizumab
Roche has WITHDRAWN the US accelerated approval for atezolizumab in combination with chemotherapy for the treatment of patients with advanced TNBC whose tumours express PDL1
"Roche will work with the FDA over the coming weeks to complete the withdrawal process. Roche is notifying healthcare professionals in the US about this withdrawal. Patients in the US being treated with Tecentriq for PD-L1-positive mTNBC should discuss their care with their healthcare provider."
https://www.roche.com/media/releases/med-cor-2021-...
-
All I can say is thank goodness for our nhs - even if it’s not perfect by a long way!
-
EANO–ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours
https://www.annalsofoncology.org/action/showPdf?pi...
- •This Clinical Practice Guideline provides management recommendations for patients with brain metastases from solid tumours.
- •The guideline covers clinical and pathological diagnosis, staging and risk assessment, treatment and follow-up.
- •Treatment and management algorithms are provided.
- •The author panel encompasses a multidisciplinary group of experts from different institutions and countries in Europe.
- •Recommendations are based on available scientific data and the authors' collective expert opinion.
-
https://www.thedenverchannel.com/news/national/res...
Another article about ErSO for metastatic breast cancer, hormone positive. I found it encouraging that the researcher from Univ of Illinois said that clinical testing could be done in the next few years. What I don't understand is why were they able to push the covid vaccines (3 or 4 different ones!) to the public in a matter of months but we have to wait years for this phenomenal medicine. And WHY do they need to test it on other cancers as the next step?
-
GoKale, I think it's money honestly. The population affected and who will benefit from it is much larger for covid, and govt's were going to be buying the vaccine for their citizens. The more cancers this vaccine can target, the easier for the manufacturer to bring it to market. If it only helps a small handful of people, it's cost prohibitive....
-
You're right, Moth. If the new drug can help other cancers then Bayer will gain a tremendous market share.
-
GoKale - thank you for posting this article! It is frustrating that the path from mouse trials to human is so much time
-
Article from today’s Times newspaper on emerging trials based on Covid vaccine platform.
-
Concerning ErSO, in the United States, would people that are at the end of the road as far as treatment options be able to try it under President Trump's "Right to Try"?
-
Karenfizedbo - the article you posted sounds very interesting. I had read a while ago that one of the people who helped develop the Covid vaccine had been working on a cancer drug that used the same mechanism. She had to stop working on the cancer therapy to start working on the covid vaccine. So this therapy sounds further along than the ErSO drug which is encouraging.
Cowgal - I forgot about the "Right to Try", thanks! That's encouraging!
-
Karenfizebo - thank you for the post. I have been hoping that the research/technology/money/science behind the Covid Vaccines will lead to better treatment/options for diseases/conditions such as cancer.
-
-
Posted this in clinical trial thread but want to repost it here too:
Dear all, it is so cool Covid-19 helped to advance mRNA technology that is coming into cancer world. What a great idea to make your body produce leukocytes with vaccine-induced cancer antigens. I think it will become another great tool in combination with existing drugs: https://www.fiercebiotech.com/research/biontech-re.... There's also a recruiting clinical trial there for solid tumors. In my list! Hooray!
Saulius -
https://www.mdanderson.org/cancerwise/what-is-tumo...
This article is about TILs therapy. Judy Perkins benefited from this therapy but she also had a gene mutation. I don't know if a patient has to have a gene mutation for this to work. It also says that TILs works on solid tumors. Do you think that includes bone mets? I will ask my MO about this later this month.
-
GoKale,
I'd be interested in hearing what your doc says. To my knowledge, this is still being tested. However, I had had the NIH trials bookmarked and recently pulled up that bookmark and it looks like they are not currently taking patients. I don't know if this is related to the actual testing or related to Covid stuff -- because the TIL therapy requires, to my knowledge, going in and out of the hospital for different periods of time.
-
Interesting video- SBRT is becoming more of an option! But has a way to go.
Dee
-
Did anyone see this - very relevant to Stage4 ER pos —https://www.sciencedirect.com/science/article/pii/S2059702921001927
-
Whatayear,
Very interesting article. When I started on palbo, I read through all of the paperwork and raised with the NP assigned to my oncologist that I was taking a PPI. She passed it off and just said -- don't take them at the same time. Make sure you have a 2 hour window between the two drugs. I got about a year and a half on palbo -- sounds like her advice may not have been exactly on point.
-
Wow, great article. I also sporadically took a PPI, maybe three or four times in the two years on Ibrance. I am switching to Xeloda. She did tell me that Pantoprazole could interfere so try Tums or something else. Pantoprazole never made any difference to me. It didn’t really help. Thank you for sharing.
-
Whatayear - that is an interesting article. I had to look up PPI to see what it was. I also read that people taking a PPI for a year or longer (not cancer patients) have an increased risk of breaking a hip. Yikes! I don't take PPI, and had to confirm that Rolaids are not a PPI. This is great information to know because a nurse had casually mentioned Protonix, and that I should discuss it with the MO. I just looked it up and it is a PPI. So I am glad to know this information, Whatayear. Thanks!
-
In an interview with Targeted Oncology for Metastatic Breast Cancer Awareness Day, O'Regan discussed how the metastatic breast cancer landscape has changed and suggested potential regimens that could further that change.
-
Tinkerbell, very interesting.
Have you seen Lumpie?
-
Tinkerbell - thank you for posting that article. It was quite honest, but also hopeful. No mention of the ErSO med, though.
-
interstitial lung disease is a problem with ADCs used for her2+ tx
Pls share with her2+ peeps so they're aware & vigilant to report symptoms such as shortness of breath.
https://jamanetwork.com/journals/jamaoncology/arti...
Twitter thread by lead author https://twitter.com/PTarantinoMD/status/1448679136...

-
LillyisHere: I hope Lumpie is taking a break from these boards. I looked forward to her sharing the latest research information. Until she returns I hope anyone sees anything research worthy please post. Thanks
-
I've been reading more about Erso too. Sounds very hopeful except for how slowly things move to trial. I hope we can all keep the conversation going on this and possibly bombard the researchers with questions about it to hopefully get things moving. It really sounds like this could be different than these meds that just string us along for a few more months. Wouldnt it be great if these drugs that just extend life by a few more months than the last one could be put out of business by something that finally looks like more of a cure for this type of breast cancer.
-
Elenas401 - Yes, I completely agree about ErSO. I am going to ask my husband to hunt down several people and their email addresses to try to get some answers about clinical trials. He's retired and I am not so he has more time to hunt for information; though I am positive, I am more motivated! haha!
-
cross posting from clinical trials thread
https://www.annalsofoncology.org/article/S0923-7534(21)04498-7/fulltext#fig1
Not sure if I agree with everything the article says, but, this very detailed ESMO article gives recommendations for lines of therapyIn ER+ notice that targeted therapies are preferred to chemo for the first 2 lines in most cases. This should help more patients who don't respond and are interested in clinical trials be eligible due to the rigid restrictions of lines of chemo.
ER positive Second-line treatment after CDK 4/6 +ET
- o Selection of second-line therapy (ChT versus further ET-based therapy) should be based on disease aggressiveness, extent and organ function, and consider the associated toxicity profile.
- o Alpelisib/fulvestrant is a treatment option for patients with PIK3CA-mutant tumours (in exons 7, 9 or 20), prior exposure to an AI (± CDK4/6 inhibitors) and appropriate HbA1c levels [I, B; ESMO-MCBS v1.1 score: 2; ESCAT score: I-A].
- o Everolimus/exemestane is an option since it significantly prolongs PFS [I, B; ESMO-MCBS v1.1 score: 2]. Tamoxifen or fulvestrant can also be combined with everolimus [II, B]. If everolimus is used, stomatitis prophylaxis must be used.
- o PARP inhibitor monotherapy (olaparib or talazoparib) should be considered for patients with germline pathogenic BRCA1/2 mutations [I, A; ESMO-MCBS v1.1 score: 4; ESCAT score: I-A] and as an option for those with somatic pathogenic or likely pathogenic BRCA1/2 or germline PALB2 mutations.
- o At least two lines of endocrine-based therapy are preferred before moving to ChT
Dee
-
Apparently there is still a dearth of great mouse models that support extensive breast cancer metastasis. Scientists have now created a better model by engineering mice to express the human version of the hormone prolactin, and it supports more extensive metastases- in addition, they showed two different prolactin blocking drugs inhibited lung mets in the new mouse model,
https://www.sciencedaily.com/releases/2021/10/2110...
-
Cure-ious Reading that was very enlightening, thank you for sharing. It's interesting that I had a tough time producing milk when I tried to breastfeed any of my three children, yet I ended up with ER+ (97%) BC. I also took birth control pills from 19 to 33 y/o, but it was 21 years later that I was diagnosed.
The other takeaway I had was that I keep seeing each type of BC, take turns as the deadliest. Seven years ago I was diagnosed and told I had "good guy" cancer (oxymoron) because I can take a pill after treatment. Triple negative? We throw chemo at it and see if it works. HER+? Very aggressive, they will try to save your life! Fast forward to today --- Now the women who most die from BC are ER+?
The fact they now have this and at least one possible treatment if it spreads to the lungs, is exciting.
-
Curious: Thanks for a sharing that info. I'm wondering why though we just don't hear more everyday about the research into Erso which seems to be the most promising thing on the Horizon for MBC. Whatever it takes to move it along quickly would be good, like the demand grew for HIV drugs years ago.
-
I keep googling ErSO to see if there is any news, and I find only articles from July 2021. Here is Bayer's website https://www.bayer.com/en/contact-us I used their "contact us" form to send them an email just now asking about clinical trials.
This page on the Bayer site https://www.bayer.com/en/pharma/access-investigati... show information on how to try a new drug that hasn't gotten FDA approval yet.
-
https://clinicaltrials.gov/ct2/show/NCT04708860 This trial is looking at the effects on progression in MBC patients with Hr+ breast cancer when they do nightly prolonged fasting (greater than 13 hours) and moderate exercise 120 minutes per week with 2 weight lifting sessions per week for 12 weeks. Study participants taking either Ibrance or Piqray along with endocrine therapy. Study concludes 9/30/2021 with results July 2022. I will be curious to see the results. I have been doing prolonged nightly fasting most days since 2017 plus more exercise than this study suggests (and it didn't prevent metastasis). Even though it didn't work for me, it's easy to do so I will keep at it.
-
Thanks for posting the link, I've just messaged too. Here's hoping
Jools xx
-
business wire MBC pipeline report.
Interesting summary
Dee
-
I found this post about erso. It has the email address of the CEO.
-
Simone,
Thanks for posting. I just emailed him. I would urge everyone else to do so as well. Hopefully, the guy has a heart.
-
As have I, Simone and Bev. Thanks for posting!!
-
Metavivor.org has some useful information about how to contact your members of Congress. Look at the Stage IV stampede section.
-
Thank you, Simone, for posting Werner Baumann's email address. I have emailed him just now and plan to send a new email every day.
-
Hopefully it works and he will get things moving.
-
Simone, Thanks for posting the ErSO thread. There was a link to a change.org petition further down in the thread:
https://www.change.org/p/bayer-possible-breast-can...
-
Here is a recent Nature paper analyzing different types of fasting (namely the nighttime calorie-restricting diet vs the fasting-mimicking diet) in terms of effects on primary and metastatic breast cancer (lung in this case) in mice- they find the nighttime fasting (13+ hours of a water-only fast every evening, as GoKale mentioned) to be the best way to fight cancer cells and improve immune response
https://www.nature.com/articles/s41467-021-26431-4
-
Re ERSO, I think it was just an unfortunate press release, in that their enthusiasm they made it sound like a potential cure, but what was reported looked like just a regular "dang good in mice" kind of finding
-
Another Nature paper identifies a gene KDM5B as a problem for immunotherapy- this gene is already a target drug companies are working on- inhibition of KDM5B enzyme activity strongly up-regulates immune system attack on solid tumors and helps immunotherapy work
https://www.nature.com/articles/s41586-021-03994-2
Related to that, Cell has an open-access review of all things Immunotherapy-related; if immunology is your thing you will appreciate the scope:
https://www.cell.com/cell/fulltext/S0092-8674(21)01101-6
-
Cure-ious - you don't think ErSO will work in humans? I'm willing to try it, and I am going to email the CEO of Bayer every day. I'm asking my family members to email him, too. Plus I signed and shared the change.org petition on facebook.
-
GoKale: I think many share your enthusiasm. Dr. Shapiro from U of I said they couldnt believe what they saw, unlike anything they had seen before. More than just "dang good in mice" I saw an article that brought out that they're also testing it in larger animals. I'm glad so many are doing whatever they can to get this moved along faster. Bayer has already invested so much in this it must look promising to them. So many things don't turn out but just think about what it would mean even if it worked almost as good in people. Let's keep hopeful. HIV patients had to to get meds that are keeping them alive today.
-
GoKale, I absolutely agree with you - if there's a promising drug, we must push for it to be tried out on humans. I know several drugs that were amazing with mice, and yet they do not reach humans in over 5 years because of many reasons (mostly inaction of institutions, lost interests as ,,it might cost too much", etc.). I am not naive and do not say that what worked in mice might work in humans as well 100% but man, at least we have to try, as mechanism of action is known, toxicities are known (mice!), and probably the only problem that remains is delivery in larger bodies. HIV patients were pushing for their drugs very hard and what they have today is amazing (sure, you cannot compare HIV with C). You never know until you try. Saulius
-
my two cents - not that I’m a expert but — some drugs look very promising in animal studies but the researchers can’t get a drug company or other funding entity interested and the project goes nowhere
In the case of ERSO, Bayer has put lots of money behind it doesn’t that mean something? At the very least, human trials will go forward, even if the result is not positive, there will be an answer one way or another
-
GoKale, Of course it could be terrific in humans but there have been many treatments that work fabulously in mice and end up disappointing in humans (indeed we can cure cancer in mice). Mouse models of human disease are being improved but have problems recreating the mechanism of metastatic spread to various organs, and also do not recapitulate the tumor-immune system interactions that protect tumors in humans, so anyway my sense was ERSO data looked good but its in early days, and there are hella lot of drugs that fall into that category. For example, I was excited about the discovery of a universal cancer neoantigen, which should allow CAR-T to work for any cancer, but there's still no news for any clinical trials and its been two years now. Similarly, very excited about the IL19 decoy drug that in mice makes immunotherapy work amazingly on all kinds of cold tumors, they promised trials were coming but there's been no news for a couple years.
I hope you learn some insider information, and I'd be thrilled if it works- sometimes it seems these companies need people pushing them from the outside
-
The FDA strengthened safety standards for breast implants
The agency will require manufacturers and plastic surgeons to warn prospective patients of possible complications, The {Washington} Post's Katie Shepherd reports.
Key context: The requirements come after years of complaints from tens of thousands of women who received breast implants and later had brain fog, fatigue and other health issues, known as "breast implant illness."
Providers will now be required to walk patients through a checklist of risks. It will warn of cancer linked to the implants and patients will be required to affirm that they understand that breast implants don't last a lifetime.
https://www.washingtonpost.com/health/2021/10/27/f...
{Complete article may be behind a pay wall... not sure...}
-
Lumpie, so good to see you back. Thank you for the link. So helpful for me since I am considering the next step to remove the implants.
-
Thank you, LilyIsHere! very glad I could pop in. Schedule has been hectic lately but I am trying to ad a bit here and there. I get notifications of posts and enjoy following the postings/discussion.
-
NIH Director Francis Collins On Covid, Faith, And The Future Of Medical Research In The U.S.
Doctor Francis Collins is stepping down as director of the National Institutes of Health after 12 years. He reflects on his legacy and his agency's efforts in the fight against COVID-19.
https://dianerehm.org/audio/#/shows/2021-10-22/nih-director-francis-collins-on-covid-faith-and-the-future-of-medical-research-in-the-u-s/116534
@{@45 minute interview by Diane Rehm. Not exclusively, or even primarily, about cancer research, but may be of interest to those interested in NIH, medical research and some of the humans behind this work. No charge for access. You'll have to copy and paste the *full* web address to get to the right episode.}
-
TNBC Vaccine to prevent recurrences: trial
-
Lumpie, you were missed! Glad to see you posting again. I love this thread as I learn so much - I keep my MO on his toes…LOL
Santabarbarian, that is an interesting trial. I hope it proves to be a success!
-
I join the chorus celebrating Lumpie. I missed her posts. Thank you Lumpie. Glad to see you back and I hope all is well with you.
-
Study: Eating nuts improves survival rate in breast cancer
A study in the International Journal of Cancer found that breast cancer survivors who consumed more than one-half ounce of nuts a week had 94% five-year survival and disease-free survival rates, while those who didn't consume nuts regularly only had an 89% five-year survival rate and an 86% disease-free survival rate. The findings also revealed that 94% of the participants who ate nuts regularly did not report return of their breast cancer within half a decade of recovery.
Full Story: United Press Internationalhttps://www.upi.com/Health_News/2021/10/20/breast-cancer-nuts-survival-study/1631634735622/
https://onlinelibrary.wiley.com/doi/10.1002/ijc.33824
{Golly. That's a plus. The study only evaluated 5 years and notes that long term study is needed. Free access to both reporting and to the journal article. (I don't know why it's still underlining....) }
-
You are all too kind and generous with the very nice comments! It is good to be missed. Thank you!
-
I love nuts but they are expensive and not very filling despite being highly caloric. They're basically dessert for health-concscious fancy people.
My first impulse was that nuts are standing here as a proxy for socio-economic status and it was interesting to me that when they adjusted by income, nuts actually made no impact on overall survival.
-
Only a 1/2 oz of nuts a week isn't much. I've been eating 2 tblsp a week for some time & it has helped lower my cholesterol. Of course almonds & pistachios are better for you than cashew nuts. And naturally un-salted are better too. Sometimes they are dessert, but just as often I throw them in a salad.
-
I remember hearing that walnuts, specifically, may be good for breast cancer patients. Here’s a mouse study -
https://pubmed.ncbi.nlm.nih.gov/30979659/
And I think there are other studies with walnuts
-
I have been eating nuts every day for many years and I keep them at work, car, home even though my kids are allergic to tree nuts. I even mix nuts with honey and eat them as dessert. Since starting letrozole I am finding them difficult to digest and I don't eat as much anymore.
Salamandra, you can find them cheap at Costco.
-
Agree about the Costco prices. Yes walnuts are high on all the 'good' lists. Unfortunately I am allergic to walnuts & macadamia nuts - but I eat all the rest.
-
Walnuts are good for your brain as well. Here in Ky you can find walnuts for free if you want to go to the trouble to crack them open yourself.
-
Ooohh yes good to see you Lumpie and a real pic of Cure-ious!
-
I'm wondering, in these instances where funding a human trial is an issue, does Metavivor come in to help fund? I give 2% of my net commissions to a handful of charities and of course Metavivor is one and the next one up for a check.
-
I received a response from Bayer about the emails I have been sending with requests for ErSO clinical trials:
Thank you for your inquiry regarding one of our drugs in development, ErSO. As you may have read, it has shown promising results in pre-clinical models of breast cancer. However, before it can be tried in humans, additional safety tests (such as in primates) must be undertaken, and that is where the compound currently is in development. We try to move our compounds through development as quickly as possible, but at the same time we have to take the prudent steps to ensure that the compounds are safe and provide the potential benefits we are striving to achieve (and thus the tests in other species such as primates). Because of these necessary steps the drug is not currently available for trials in humans. However, we hope to be able to provide an update on the status of the program before the end of the year.
If you would like to contact me in a 6-8 weeks, I may be able to give you a more definitive schedule.
You should know that Bayer posts its human clinical trials for all of its drugs on clinicaltrials.gov and that is another source for ongoing (or soon to start) clinical trials.
I hope that your doctors find ways to control your cancer in the meantime.
Sincerely,
Joseph Germino, MD, PhD
Vice President USMA
Bayer Healthcare
-
WOW, Kale!! Great job, and thanks so much!
-
Go Kale!
-
GoKale,
Wow, it's wonderful he responded to you. Thanks for sharing.
-
GoKale, thank you so much for taking the initiative on this. Wonderful that you received what appears to be a personalized response. Can you share the email address you used to contact Mr. Germino?
Praying that ErSO reaches human trial phase soon and that it actually works! I'm very cautiously optimistic.
-
MoCoGram - here is the email address for Dr. Germino
joseph_f.germino@bayer.com
-
Someone asked about METAvivor funding for research. METAvivor has a research funding application process. It takes place once or twice a year. Petitioners must complete a grant application. This is typical in the grant application/research "space." Applicants are scored and ranked by a scientific team and by patient advocates team. Scoring relates to chance of success and potential impact. A board makes final decisions about awards. Those interested in applying can find more info on the METAvivor website.
-
Sharing this update from the American Cancer Society's Cancer Action Network:
Exciting news! We have recently released some initial findings of our last Survivor Views survey, which focuses on patient experiences with telehealth and issues around clinical trial participation. As noted by ACS CAN president Lisa Lacasse in today's press release, "These data suggest we have a real opportunity to make clinical trial participation easier for all patients by removing barriers to participation, including through the use of telehealth technologies and reducing out-of-pocket costs."
To all those who responded to our Summer 2021 survey, THANK YOU! You've contributed your voice to our mission of improving the lives of cancer patients and survivors. With the Survivor Views project, we do this by making sure you are heard by the decision makers shaping health policy.
If you haven't yet responded to our current survey, which covers topics like paid medical leave for patients and caregivers, please click the following link to respond by November 15th:
https://survey.us.confirmit.com/wix/p925353504545.aspx
{If you are interested in signing up for the ACS Cancer Action Network, you can do so here:
The group does both advocacy and fundraising. You can pick and choose your level of participation.}
-
A very interesting episode (there are more - please check): https://www.ourmbclife.org/episodes/rtac-lin-parso...
Also lot's of useful information and articles.
Saulius
-
Thanks for that link Saulius! Great conversation.
-
https://investor.lilly.com/news-releases/news-rele...
FDA has approved Verzenio for HR+ HER2 -, node positive high-risk early breast cancer
"This subgroup analysis (N=2,003) included patients with ≥4 positive axillary lymph nodes (ALN), or 1-3 positive ALN with either Grade 3 disease and/or tumor size ≥5 cm, and whose tumors had a Ki-67 score of ≥20%. There was also a statistically significant improvement in IDFS for this pre-specified subgroup of patients receiving Verzenio plus ET compared to those who received ET alone."
"The number of IDFS events at the time of this analysis was 104 with Verzenio plus ET compared to 158 with ET alone."
-
Jenny - man that stuff has some bad side affects.
-
HomeMom,
Thankfully, I don't meet their definition of "high-risk", so I won't be adding this to my treatment regimen. But if I did, I would be happy to know that this was an additional option to help prevent metastatic recurrence.
-
FDA is Moving Away from the Maximum Tolerated Dose!
The decades-long paradigm of leveraging the highest and most toxic dose of a cancer drug, called the Maximum Tolerated Dose (MTD), will be coming to an end.
Shortly after the PCDI's presentation about MBC patients' treatment-related side effects at ASCO's 2021 worldwide conference, Richard Pazdur, Director of the FDA's Oncology Center of Excellence, stated that the FDA will start requiring drug companies to test the efficacy of multiple drug doses during clinical trials instead of identifying and moving forward with the MTD.
This is a game-changer because the MTD, which is identified in Phase 1 clinical trials that focus solely on toxicity, is the dose that generally causes the most severe side effects. In today's world, whenever patients with MBC begin a new treatment, they are generally prescribed the MTD unless there's a medical contraindication. But in tomorrow's world, at least two doses will be identified in Phase 1 clinical trials for further study so that ultimately the optimal dose - based upon a balance of efficacy and toxicity - will be given to patients.
If this subject interests you, please consider joining a webinar hosted by Friends of Cancer Research on Wednesday, Nov. 10th at 12PM ET. Panelists including the FDA, pharmaceutical companies, Friends of Cancer Research, and the PCDI, will be discussing the transformation of MTD-based oncology studies.
You may register here for the free conference!
Thank you,
Anne Loeser, Author,Founder PCDI
{The above is from an email dated 11/6/2021 from Anne Loesser. Some of you may have received it. This is great news IMO. Less toxicity while maintaining efficacy is what we all want. I believe that the Friends of Cancer Research session on Patient Centered Dosing is only one hour long.}
-
Hi Lumpie, re MTD can I just jump in and say that I have NEVER tolerated the Max Dose of pretty much any cancer drug. I’ve had a few now and they have always required reductions because the side effects are just awful. So far we’ve managed to get to a reasonable level albeit with plenty of side effects. I agree that we should not be accepting the max dose just because that’s where the clinical trials are pitched. Much more research required!
-
the discussion about max dose jogged a memory. I was told that it is known that a lot of people won’t be able to tolerate the max dose and it is expected that there will be dose reductions. I can’t remember the exact reason, but studies are done at max dose because it’s easier to dose reduce than to get approval for a dose increase. Meaning, you can always prescribe it for a lower dose than it’s approved for use for, but you can’t prescribe it at a dose it wasn’t tested and approved for ( higher). Therefore the starting dose is often higher than what some people can tolerate.
This is from my memory of when I was on Xeloda and had to do a dose reduction and from discussions I had. When I was in a clinical trial.
-
I saw a very interesting presentation on the steps in a clinical trial and exactly how they determine the maximum tolerated dose and it had discussion about determinations around what dose reductions are "officially" permitted. It was a really good presentation. If I can find a link, I will post it, but ... I don't know... it's been a while....
-
If you missed the Friends of Cancer Research presentation on....
Maximizing Benefit and Improving Tolerability for Patients Through Dose Optimization
Here are the links:
Click HERE to Watch
Click HERE to access the Pre-Conference White Paper.It is about 1 hour long.
-
Treatment landscape of triple-negative breast cancer — expanded options, evolving needs
Nature Reviews: Clinical Oncology Nov 2021
covers early stage as well as metastatic setting. Link is publishers complimentary access - might expire at some point. main link: https://www.nature.com/articles/s41571-021-00565-2 & doi https://doi.org/10.1038/s41571-021-00565-2
-
Atlas of Lobular Breast Cancer Models: Challenges and Strategic Direction
https://www.mdpi.com/2072-6694/13/21/5396/htm -
Dear All, a very interesting summary on ongoing/future research in ADCs with tables of main clinical trials: https://acsjournals.onlinelibrary.wiley.com/doi/10.3322/caac.21705#caac21705-bib-0119
-
News > Medscape Medical News > Conference News
Survival Doubled in 2 Types of Met Breast Cancer, Says Expert:
Unfortunately I can't seem to send a link. However you can join medscape for free to read the article. Recent update on survival trends.
-
Tinkerbell, thanks for posting that.
https://www.medscape.com/viewarticle/962953#vp_1
For those who can't access it, the positive trends are ER+ and HER2+ - not a real surprise is it?
"Patients with two of the three major types of advanced breast cancer now have a median overall survival of at least 5 years, which is roughly a doubling of survival time over the past decade, says an expert."
The only positive thing said about TNBC was that trodelvy improved our survival by 5 months. Not much of yippeee for mTNBC
Honestly, I feel like throwing up - I'm so tired of triple neg. I'm so tired to of mbc support groups being dominated by people with more favourable diagnosis. If I hear thriver one more time I'm going to scream. Oh dear, maybe this should be in the steam room.... But yay, I'm glad for the ER+ and HER2+ peeps!
-
Moth, aren't you ER+ now? I am sorry if I am mistaken but from your signature, it seems that you moved to ER+, and hopefully, letrozole will keep it under control for a very, very long time.
-
Lilly, no, I have one met which tested faintly er+ but so faint that they consider me triple neg still. We added the letrozole just in case but honestly nobody thinks it's doing anything and it was debatable whether I should have started it.
My original biopsy also had a very faint trace of er+ which they struggled to categorize. Oncotype has me as triple neg and we've been treating as triple neg.
-
Moth: Thanks for adding to my failed attempt with sending a link. I attended a virtual conference on Sunday for MBC. There was positive chatter for mTNBC, especially w PARPi and Pik3 mutation (utilizing PIqray if + positive for the mutation.) besides or in combo with immunotherapy.
-
I'm sorry Moth. I had this hope of having ER+ in order for letrozole to work. Hugs.
-
alas,I've been tested & have no somatic or germline brca or pik3ca mutations. I have had a good run on immunotherapy + chemo. By mTNBC standards I've done well so I shouldn't complain but you know how it is...5 years is the stuff dreams are made of for me.
-
I am sorry, moth. The article about the doubling of the survival time arrived to my Inbox a couple of days ago, and my first thought was of compassion towards every patient out there reading this who has triple negative mbc. I specifically thought of you, because although I don't know you, I always read your insightful advice and comments in this forum. I send you a big, big hug, sister. You are not alone. Very very sorry. You had such bad luck. Here is for your dream becoming true, for you making it to the five years, and then for some breakthrough drug that tames that cancer freaking beast that we hate so much. And yes, you absolutely can complain.
-
Moth, LaughingGull said everything I wanted to say (except SO much better than I could have written.) I always read your posts because they are so insightful and filled with useful information. You make a difference - probably to a lot more people than you can imagine. Thank you for that. Sending you a virtual hug, to be used any time you need it and for as many times as you need it.
-
Dear All, ESMO Immuno-oncology has amazing seminars on 08-11/12/2021. I find day 2 (9th) very intriguing, especially TIL, TCR, CAR-T, and multi-specific engagers in solid tumors. Please, whoever has time, follow: https://cslide.ctimeetingtech.com/immuno2021v/attendee/confcal/session/calendar/2021-12-09
Cell therapies and bispecific agents in the pipeline
Date: Thu, 09.12.2021, Time: 14:30 - 16:00 Room Room A, Chairs: Marco Donia (Herlev, Denmark) -
Saulius,
Thanks for posting. Odd that ESMO overlaps with SABCS? I thought they generally ran at different times.
-
awww, LaughingGull & Tess, thank you so much. You made me cry - but in a good way, kwim...
BevJen, I did a double take at that too because I was sure I'd followed some ESMO sessions this year...then I thought maybe that was last year & I'm really out of it? But no, main ESMO is over already. They have an immunology mini congress. I'm signed up for SABCS so not sure how I'll organize my time. (and fit in all my hallmark xmas movies!!! priorities!... lol)
-
regarding the Bayer ErSO, just saw a screenshot of someone else's correspondence & it's bad news - they're NOT proceeding to Phase 1 trials at this time https://twitter.com/LibbyMbc/status/14606547735022...
-
Thanks, Moth, for passing on this information about ErSO. What a lucky turn of events. Looks like only mice have a cure.
I have an appointment at Dana Farber to see what further treatment I should pursue and to see if I might qualify for the ErSO clinical trial. I probably should cancel it since I can now clearly see the path of maybe 3 different CDK4/6 inhibitors and then nothing.
-
That's disappointing news about ErSO. Makes you wonder sometimes.
-
https://link.springer.com/chapter/10.1007/978-3-03...
Systematic Review of Exercise for Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy
"The 10 randomized studies collectively suggest that exercise is beneficial for the treatment and prevention of CIPN with little to no side effects. However, these studies tend to be either rigorous yet small or large yet simple and exploratory, with no Phase III randomized studies published or pre-registered"
-
Dear BevJen, SABCS does not overlap with ESMO - this is just small four day routine event for immuno-oncology... Europe does a lot in this field, so that is why.
Also... very disappointing for ErSO. This is so typical... I know a few drugs (classical example is oral Taxane - Tesetaxel) that "drowned" in the pool of financial turmoils:/ Hopefully there will be another investor but they have wasted so much time with Bayer. Crap!
Saulius
-
I would travel to Europe, if I could figure out where to go to get the drugs that the FDA won't approve. I wonder if the problem with ErSO is that it would put a big dent in the profits of the other pharmaceuticals as well as doctors so a backroom deal was made to squash the study. Do you think Europe is different when considering the actual welfare of common people?
-
The issue isn't that the FDA isn't approving the drug. It's that Bayer won't invest in it. I really think if they thought they could make money off it, they'd do it. I think pharmacorp thinking is 1. is this drug good 2. how much do we need to invest to get it through trials 3. how much profit will we make.
If the drug is good but not spectacularly better than a different drug already on market or in pipeline, then dependng in financial positions, a company might decide to not proceed. I'm guessing that's what happened with atezolizumab/tecentriq in the US. It's not that it isn't a good drug - it is, but trodelvy is probably better so the market share would have been smaller.
The obvious way around it would be for governments to bring drugs to market, rather than relying on pharmacorps whose responsiblity is to their shareholders. or at least for governments to subsidize certain drug development --- that's an issue especially with rare diseases because the market there is so small, companies won't invest in the drugs.
-
genentech almost didn't fund herceptin and in fact, Dr Dennis Slamons was lucky enough to catch the attention of someone who knew the wife of the head of Revlon Cosmetics and that's how he raised money to continue some of his early research!
So, yeah, just because pharmacos are being dick heads doesn't mean the drug is ineffective.
Wonder if Systems Oncology will continue pursuing this...hope so.
-
Dear Moth, there's another possibility you did not mention: ErSO might be good but is extremely cheap to sell, i.e. everyone knows it is easy to make, market and you cannot sell it wit 2000% margin, meaning that you have to invest quickly into clinical trials now and pay-off comes slowly and begins to pay off in 10 years = not very interesting for a big company (who knows what will happen in 10 years?:)... this also has already happened. Saulius
-
Just saw an article that said that Systems Oncoligy will be going ahead with Erso and that it may go into clinical trials for Ovarian cancer too.
-
Elanas401 - Wow! Fantastic news, thanks for posting. This is something to ponder; the "failed" trial with Bayer could very well be simply not a large enough profit margin as mentioned above by Saulius. Maybe Systems Oncology is more humanitarian.
Great news, thanks!
-
TriNeta Becomes an FDA Breakthrough Device for Early-Stage Breast Cancer Detection
The FDA has granted breakthrough device designation to TriNeta, a blood test designed to detect early-stage breast cancer, according to a press release by the developer Datar Cancer Genetic, Inc.1
The test works by detecting circulating tumor cells that are specific to breast cancer. In recent studies, TriNeta detected cancer as early as stage 0 and stage 1 with a high level of accuracy. To detect cancer, only 5 ml of blood is needed. Patients that can be tested with the device are asymptomatic women who are older than 40 years of age with a prescription from their physician.
-
wow, that's great news
-
Wow that is amazing. Wonder if there is application after diagnosis/treatment with stage 1 to determine if further years of hormonal therapy needed?
-
elenas401 - that is great news for ErSO. I wonder if Bayer did that press release in July just to create a buzz to increase the value of their stock. They probably thought investors would jump on it, but didn't think they would be bombarded by a large gang of menopausal breast cancer patients! I hope Systems Oncolgy succeeds without them. It would be wonderful if this drug becomes a game changer for us. Even if not a cure, perhaps better quality of life and long term remission could be achieved.
Were you able to try the Alpha Dart treatment you mentioned?
-
Study compares spiral breast CT, digital mammography
Researchers found that patients who underwent spiral breast CT experienced a significant reduction in discomfort and pain, especially among premenopausal women, compared with digital mammography. The findings, published in the European Journal of Radiology, also showed that using SBCT led to a "favorable" interrater agreement among radiologists and was able to consistently detect microcalcifications at a radiation dose that is comparable to digital mammography.
Full Story: Health Imaginghttps://www.healthimaging.com/topics/diagnostic-screening/patients-prefer-spiral-breast-ct-over-dm
{No charge for access to reporting.}
-
Age Distributions of Breast Cancer Diagnosis and Mortality by Race and Ethnicity
- The authors used data from the SEER database to identify trends in breast cancer diagnosis and mortality by race and ethnicity. Minority women were 72% more likely to be diagnosed with invasive breast cancer and 58% more likely to be diagnosed with advanced breast cancer at young ages compared with white women. Minority women were also 127% more likely to die of breast cancer at a young age.
- Minority women are disproportionately impacted by advanced breast cancer at a young age, and this should be considered when developing screening guidelines for breast cancer.
DOI: 10.1002/cncr.33846{Free access to reporting/summary and to journal article.} -
elenas401, can you send the link to that article? cant find anything
-
Anyone interested in enrolling in the op-1250 trail, don’t hesitate! Its amazing what it can do according to the clinical coordinator who shared this info with me
Link: https://drive.google.com/file/d/1FklxhTXj4N3odFI2lJscdQIUMmQ5u_ZS/view?usp=drivesdk -
Thanks, DeeBama, for the information on the OP-1250 trial. Sounds very encouraging.
-
Early research in mice...
New therapeutic approach prevents growth of metastatic tumors by putting cancer cells to sleep
...In a previous study, Maria Soledad Sosa from the Icahn School of Medicine at Mount Sinai and Julio A. Aguirre-Ghiso, now at Albert Einstein College of Medicine, discovered that the ability of cancer cells to remain dormant is controlled by a protein called NR2F1. This receptor protein can enter the cell nucleus and turn numerous genes on or off to activate a program that prevents the cancer cells from proliferating.
...In the new JEM study, Sosa and Aguirre-Ghiso's teams used a computer-based screening approach to identify a drug, named C26, that activates NR2F1. The researchers found that treating patient-derived HNSCC cells with C26 boosted the levels of NR2F1 and arrested cell proliferation.
..."Drugs that activate NR2F1 might be particularly useful in breast cancer," says Sosa. "NR2F1 is highly enriched in ER-positive tumors when compared to ER-negative tumors, and activating NR2F1 might be able to suppress reawakening of dormant cancer cells kept in that state by anti-estrogen therapies." However, because C26 treatment elevates the levels of NR2F1, the approach may also be useful for other cancers with inherently low levels of the receptor protein.
-
I hope so, Deee, and now I don't remember either...but it was helpful! That expains my not being able to go back and review what you said before I sent my reply!!
-
And the very best of luck with the trial! Keep us all posted!
-
AlabamaDee's account continues to be compromised. The poster above, AlabamaDeee, which started out as BamaD is NOT the real AlabamaDee. We are in contact with the real AlabamaDee and she has NOT re-registered. Please do not respond to anyone claiming to be AlabamaDee until we notify you.
Please be cautious about sharing your email addresses, or any personal information over PM.
We are working on this issue. Please contact us via PM, or to community@breastcancer.org if you have any concerns.
Warmly,
The Mods
-
New cancer therapy from Yibin Kang's [Princeton] lab holds potential to switch off major cancer types without side effects
Cancer biologist Yibin Kang has spent more than 15 years investigating a little-known but deadly gene called MTDH, or metadherin, which enables cancer in two important ways — and which he can now disable, in mice and in human tissue, with a targeted experimental treatment that will be ready for human trials in a few years. His work appears in two papers in today's issue of Nature Cancer...
"You can't find a drug target better than this: MTDH is important for most major human cancers, not important for normal cells, and it can be eliminated with no obvious side effects," said Kang, Princeton's Warner-Lambert/Parke-Davis Professor of Molecular Biology and one of the principal investigators of the Princeton Branch of the Ludwig Institute for Cancer Research.
"In the two papers we are publishing back-to-back today, we identify a compound, show it is effective against cancer, and show that it is very, very effective when combined with chemotherapy and immunotherapy," said Kang...
-
21-Gene Assay to Inform Chemotherapy Benefit in Node-Positive Breast Cancer:
Among premenopausal women with one to three positive lymph nodes and a recurrence score of 25 or lower, those who received chemoendocrine therapy had longer invasive disease–free survival and distant relapse–free survival than those who received endocrine-only therapy, whereas postmenopausal women with similar characteristics did not benefit from adjuvant chemotherapy.
-
Definitive Local Therapy in Select Patients With HER2+ de Novo Metastatic Breast Cancer Treated With Dual Anti-HER2 Blockade
- The authors of this retrospective study evaluated the role of local therapy in addition to systemic chemotherapy plus dual anti-HER2 agents in selected HER2-positive de novo metastatic breast cancer. There was a superior 3-year overall survival for patients who received both surgery and radiation compared with those who received surgery alone, radiation alone, or no local therapy.
- Further prospective studies are warranted to confirm the findings for select patients with HER2-positive de novo metastatic breast cancer.
Breast Cancer Res Treat 2021 Nov 17;[EPub Ahead of Print], L Rosier, Y Wang, JH Lee, K Daily{Free access to full article.} -
SNO 2021: Neratinib Is Promising for Leptomeningeal Metastases of Heavily Pretreated HER2+ Breast Cancer
Dr. Pellerino concluded that neratinib may be a safe and effective treatment for leptomeningeal metastases of heavily pretreated HER2-positive breast cancer. She remarked, "The study is ongoing with the aim of increasing the sample size to validate preliminary results."
Patients underwent a median of three adjuvant treatments before the onset of leptomeningeal metastases. Three patients developed leptomeningeal metastases alone. The other six harbored leptomeningeal metastases associated with multiple bone metastases. Six-month overall survival was 66.7%. One-year overall survival was 22.3%. Median overall survival was 8 (95% confidence interval 3 - 13) months. Median progression-free survival was 3.5 (95% confidence interval 2 - 6) months from the start of treatment.
Neurological improvement was observed in two of nine patients (22.2%). The remaining four of nine patients (44.5%) achieved neurological stabilization that lasted for a median of 5 (95% confidence interval 2 - 19) months. The best radiological response was stable disease in five of nine patients (55.6%). No complete or partial responses were achieved according to criteria of the Response Assessment in Neuro-Oncology.
This preliminary outcome of an extended-access program was reported at the 2021 Society for Neuro-Oncology's 26th Annual Scientific Meeting and Education Day, from November 18 – 21.
https://www.practiceupdate.com/C/127819/56?elsca1=...
{Free access to this reporting.}
-
Breast Cancer Outcomes Following Immediate Breast Reconstruction With Implants Versus Autologous Flaps
- In this retrospective study, there were no significant differences in recurrence rates, distant metastases rates, or survival rates in patients with primary breast cancer who underwent immediate breast reconstruction after nipple-/ skin-sparing mastectomy with either implant-based reconstruction (IBR) or autologous flap reconstruction (AFR).
- Oncologic outcomes were similar in this population following IBR or AFR.
{No charge to access abstract. Charge or subscription to access full article. On my computer, the journal page blocked half the screen if I did not accept ALL cookies. Very annoying. The Practice Update page which offers reporting did NOT do this.}
-
A massive 8-year effort finds that much cancer research can't be replicated
"like research in the social sciences, cancer research has a replication problem.
Researchers with the Reproducibility Project: Cancer Biology aimed to replicate 193 experiments from 53 top cancer papers published from 2010 to 2012. But only a quarter of those experiments were able to be reproduced, the team reports in two papers published December 7 in eLife."
https://www.sciencenews.org/article/cancer-biology...
-
That's pretty scary!!!
-
Duration of Endocrine Therapy in Breast Cancer: How Much of a Good Thing Is Too Much?
Tailored Approach Based on Anatomic and Biologic Risks
We think these recent data are important for clinicians and women with breast cancer and offer a tailored approach based on anatomic and biologic risks. For postmenopausal women with stage I breast cancer, who have lower-risk histologic features or genomic risk scores, 5 years of adjuvant endocrine treatment is likely sufficient, particularly if that includes an aromatase inhibitor at some point. For patients with stage II cancers or limited nodal involvement, they suggest that a treatment course of around 7 years is likely to offer an advantage over 5 years. And, finally, for women with higher-risk tumors by virtue of stage or adverse biology, longer durations of around 10 years remain the standard recommendation. As always, it is important to weigh the benefits of longer treatment against the well-known side effects of therapy, such as arthralgias, osteoporosis, hair thinning, and genitourinary health. Hopefully, patients and clinicians can use these data to make well-informed, data-driven, shared decisions about the best course of therapy.
Dr. Trapani and Dr. Burstein are employed at the Dana-Farber Cancer Institute, Harvard Medical School, Boston.
-
Users of AI, we are not crazy, SE exist:
Aromatase inhibitors have been associated with new onset autoimmune diseases.
Our cases suggest a link between aromatase inhibitors and inflammatory myopathies.
Cessation of the aromatase inhibitor should be considered if a myopathy develops.
https://www.sciencedirect.com/science/article/pii/S1297319X21001810?dgcid=rss_sd_all
-
Novel Endocrine Drug Slows Previously Treated HR-Positive Breast Cancer
-
Anyone know how to get information on SABCS?
There was something related to the trial I'm in but, I have no idea how to find whatever they did.
It should have been Wednesday Night 12/8 at SABCS 5-6:30 PM CT.
"OT1-16-01 A multicenter phase II study of vaccines to prevent recurrence in patients with HER-2 positive breast cancer
Han HS, Disis M, Wesolowski R, Fisher C, Gandhi S, Chan N, Gwin W, Gogineni K, Mick R, Sierra Rodriguez C, Hogue D, Liu H, Costa R, Czerniecki B. Moffitt Cancer Center and Research Institute, Tampa, FL; University of Washington, Seattle, WA; Ohio State University, Columbus, OH; Indiana University School of Medicine, Indianapolis, IN; Roswell Park Comprehensive Cancer Center, Buffalo, NY; Rutgers Cancer Institute of New Jersey, New Brunswick, NY; Emory Winship Cancer Institute, Atlanta, GA; University of Pennsylvania School of Medicine, Philadelphia, PA."
-
morrigan, you have to be registered as a delegate. I am one. I will try to get that info for you - I can access talks and presentations but the posters section is not working well for me (& others are having the same problem...)
-
Morrigan - the MODs usually post all sorts of information & data after the conference is over.
-
Thanks Moth and MinusTwo I'll keep my eye out. I'm also going in for Booster #2 next week so I'll ask them if they have any information as well.
The study is still on going so they were only supposed to present interim findings and, maybe some stuff on Phase 1.
-
Healthcare cost of HER2-positive and negative breast tumors in the United States (2012–2035)
The approach to advanced breast cancer has been revolutionized by targeted agents.
•The total cost of HER2-positive patients was estimated for $2,719,542,347 in 2012.•The total estimated cost for HER2-negative patients in 2012 was $8,376,028,459.•In 2035, we estimated a cost of $3.6 and $11.2 bilions for HER2+ and HER2− tumors.•The cost of HER2-negative tumors should be carefully evaluated in the coming years."...our data strongly suggest that cost-analyses should be carefully evaluated in the coming years, aimed to improve the cost-effectiveness of targeted approaches for advanced BC, in particular in patients with HER2-negative tumors. This will be crucial to guarantee the access to cure for all cancer patients and the future economic sustainability of health system."
https://www-sciencedirect-com.ezproxy.liberty.edu/...
https://doi.org/10.1016/j.ctrv.2017.08.005
{This article was evidently published in 2017, but I only recently located a link. It is a bit cringeworthy because the implication seems to me to be that we are not worth the high cost. Of course, it is mostly the drugs.... which, thankfully, are often effective, but which we know to be astronomically unaffordable. The costs/prices they cite are dramatically higher than my shocking EOB's. I can't quite make sense of that. Access to full article seems to be free.}
-
Found this interesting from Loma Linda.
Blood Test Finds 50 Types of Cancer
We reported in our August BOB Tales about this test that was invented by Grail, a biotechnology company in Menlo Park, CA. Mayo Clinic has partnered with Grail in the development of the test, which is known as "Galleri." This new test looks for signals in the blood stream that are associated with specific cancers. Cancer-specific information is carried in bloodstream DNA. According to a recent article in Health Care, "The Galleri test uses next generation sequencing and machine-learning algorithms to analyze methylation patterns of cell-free DNA," which helps identify specific cancers. Cells regulate gene expression using DNA methylation. The Galleri test can also pinpoint the location of the disease allowing doctors to select appropriate treatments to target and destroy the cancer.
Having access to a single blood test that can detect 50 types of cancer is significant. The Health Care report states, "Currently recommended cancer screenings in the U.S. cover only five types of cancer and can screen for only one type at a time." Yet, 71 percent of cancer deaths are caused by cancers that are not commonly screened for, according to Grail. False positives with the Galleri test are low, according to researchers, at about one in 200 people tested.
The test is recommended for adults, typically over 50 with an elevated risk for cancer. It should not be a substitute for currently approved tests, such as colonoscopies or mammograms.
Galleri and Mayo Clinic have not received FDA approval for this new test, and insurers do not cover the $949 cost. This blood test is, however, available to the general public and must be administered by a licensed health care provider.
FDA approval for this breakthrough blood test is expected soon and we will report here when that happens.
-
The FDA has granted emergency use authorization to an antibody combination called Evusheld that is highly effective at preventing COVID-19 infection in immune compromised patients. Press release here.
https://www.astrazeneca.com/media-centre/press-rel...
-
Perhaps some readers of this forum listen to NPR and their Morning Edition newscast. If so, you have probably heard reporting by journalist Ina Jaffe. She disclosed over the summer that she has been diagnosed with MBC. Below are links to a couple of articles she has published on the topic. While this news is very sad and disappointing to hear, perhaps it will lead to more meaningful coverage of MBC in the media. It amazes me how many people think that breast cancer has been "cured."
https://www.npr.org/2021/06/22/1009065462/breast-c...
https://www.npr.org/sections/health-shots/2021/12/...
-
Most Oncologists Discuss Drug Side Effects, Open to Reduce Doses
Roxanne Nelson, RN, BSN
December 15, 2021
Many patients with metastatic breast cancer (MBC) experience distressing toxicity related to treatment.
According to a new survey, all oncologists reported talking to their patients about side effects at every visit and nearly all (97%) were open to lowering medication doses.
The findings, presented during a poster session at the 2021 San Antonio Breast Cancer Symposium (SABCS), were encouraging to Charles Shapiro, MD, of the Icahn School of Medicine at Mount Sinai in New York City.
"I think this survey confirms that a lot of oncologists are willing to reduce the dose if patients have side effects, and a high percentage discuss side effects with their patients," said Shapiro, who was not involved in the study.
Anne L. Loeser, who has MBC and is co-author of the survey alongside a team of oncologists, agreed that it is vitally important for doctors to discuss toxicity and take patients' quality of life into consideration.
"Patients with MBC are incurable — albeit treatable — and the majority will remain on therapy for the rest of their lives," Loeser, founder of the Patient-Centered Dosing Initiative (PCDI), told Medscape Medical News. "Understandably, we want to make the most of the time we have left."
When patients begin treatment, oncologists often prescribe the recommended starting dose, which is based on the clinical trial results used to approve the drug. However, patient tolerance for this dose in the real-world setting often differs from that of clinical trial participants, the survey authors note.
In fact, Loeser said, "this dose generally precipitates the most, and worst, side effects."
In a previous survey, the team of researchers found that, among 1221 patients with MBC, 86% experienced at least one significant treatment-related side effect and almost all were willing to discuss individualized dosing with their physicians. The current study expands on that research, highlighting responses about treatment side effects and dosing options from medical oncologists.
In the new study, a confidential, 28-question online survey was sent to US medical oncologists identified via professional organizations, social media, and email lists. The objective of the survey was to gain a better understanding of oncologists' perspectives regarding the prevalence and severity of treatment-related toxicity, increase recognition of the impact of dosage-related mitigation strategies on clinical outcomes, and determine their willingness to discuss flexible dosing options.
A total of 119 medical oncologists participated in the survey. Of this group, 85% specialized in breast cancer, 66% worked in an academic setting, and 82% had been in practice for more than 5 years.
Overall, respondents estimated that nearly half of their patients had reported a distressing treatment-related side effect, 15% visited the emergency department or hospital for this reason, and 37% required a break from treatment. The most common mitigation strategies included prescribing supportive medication, offering suggestions for palliation, and lowering the medication dose.
All respondents reported reducing medication doses as a means of alleviating side effects; 74% reported that dose reduction helped relieve side effects; and 71% indicated that efficacy of the reduced dose was similar to that of the standard dose.
Notably, 60% of oncologists indicated that patients felt better when therapy began with a lower starting dose rather than the standard dose, and 59% indicated that treatment efficacy was similar to the standard dose. The drugs, or drug classes, most commonly prescribed at lower initial doses were capecitabine (91%), taxanes (60%), and palbociclib (50%).
The authors concluded that "these patient-centered dosing discussions should be part of routine care and may consequently improve [quality of life] for patients with MBC."
In the past, quality of life and quantity of life were perceived as an "either/or" proposition, but that mentality is changing, Loeser said. "In fact, the [US Food and Drug Administration] is moving away from the concept of maximum tolerated dose in favor of identifying the optimal dose with regard to safety and efficacy."
Loeser also noted that toxicity-related side effects not only affect quality of life, they also affect treatment options. These side effects "may force some patients to stop a working treatment prematurely," she said. In addition, "cumulative side effects that build up over successive treatments may preclude patients from [using] the full list of therapies available to them because they can no longer withstand the toxicities from further drugs."
Some survey participants also posted comments in the survey, elaborating on how they communicate with patients and manage treatment-related toxicities.
One oncologist emphasized the need for an individualized approach to dose adjustments: "Like other decisions, this requires good communication and an effort to understand patients' preferences and expectations, so that an informed decision can be made."
Another participant noted that "it is critical to be able to vary dose based on the individual, as well as the biology of their cancer. It is quite likely that lower doses are less effective in some cases, but this can be sorted out as treatment is ongoing."
For certain patients, dose reduction may not be the best option, one respondent said. "In some cases, it may be prudent to go a step further and move to best supportive care rather than reduce dose, particularly for late line therapy or indolent disease."
For Shapiro, establishing a strong partnership between physician and patient is critical to ensuring patients get the best care possible.
"You rely on patients to tell you what's working and what isn't with the drug, and we can make adjustments," he said. "It can be the greatest drug in the world, but if your patient can't tolerate it, then it isn't going to do much good."
The survey was conducted by PCDI. Loeser is the founder of the PCDI.
SABCS 2021. Abstract P4-10-09. Presented December 9, 2021
https://www.medscape.com/viewarticle/964899?uac=21...
{Free access.}
-
Oncolytic Virus Clinical Trial Opens for Patients With Advanced [TN] Breast Cancer
City of Hope recently announced the opening of a phase 1 clinical trial for an investigational therapy in patients with metastatic triple-negative breast cancer. The trial is a first-in-human analysis of using an oncolytic virus, which is a cancer-killing virus, to treat patients.
The researchers at City of Hope created a genetically engineered therapy, CF33-hNIS-antiPDL1, from the naturally occurring oncolytic virus. The therapy is intended to infect, replicate and kill cancer cells while leaving healthy cells untouched...
"It is an exciting time in immuno-oncology. Preclinical research has shown that this oncolytic virus can direct the killing of cancers and stimulate the immune system to enable further killing of cancers," said Dr. Yuman Fong, the Sangiacomo Family Chair in Surgical Oncology at City of Hope who developed CF33, in a news release. "This trial is an important step forward."
https://www.curetoday.com/view/oncolytic-virus-cli...
-
Great article Lumpie, as one who has required dosage reductions on every treatment so far and had to tolerate significant side effects to get to that point.
-
ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer
October 2021
https://www.annalsofoncology.org/article/S0923-7534(21)04498-7/fulltext
-
Moth,
Thanks so much for posting the ESMO link. Great information.
-
Agreed, moth. That was wonderful information. I am reading and re-reading and highlighting. Thanks!
-
https://www.cancer.gov/news-events/cancer-currents...
on the relationship between stress and the return of cancer
-
This trial is for triple negative advanced breast cancer.
-
BevJen,
Thanks for the link to the reporting on the link between stress and cancer. Ugh! Just what we don't need. We mostly focus on our own cancers and those of family and friends, but that could have all kinds of crazy implications for public health.
-
Lumpie,
It just caught my eye. After many years (8-9 years) when my cancer was quiet, I ran into a few years where my life was extremely stressful in an uncontrollable way -- illness and death of a sibling, illness and death of a parent, several other issues -- and boom, major recurrence. Perhaps stress is not the cause of all recurrence, but to me, the article just makes sense.
-
BevJen, Yes, my life was very stressful in the years leading up to my becoming sick and eventually being diagnosed. I have often wondered to what extent this contributed to the cancer's development and progression. Thx again.
-
In the midst of covid, are you tired of wandering around in a fog trying to figure out what activities are risky and which are less so? Aren't we all! I thought I would share this risk calculator from the Canadian National Institute on Aging. It seems pretty good. to use it, you need to answer several questions about anticpated circumstances. The information/assessment is available in both English and French.
https://covidvisitrisk.com/riskscore-english.html
If you want a more abbreviated descriptive tool, the Virginia Department of Health has an info graphic that is useful here:
-
'First Reliable Estimate' of Breast Cancer Metastasis
For the first time, there are now 'reliable' data to show what proportion of women with breast cancer go on to develop metastatic disease.
The data come from a massive meta-analysis of more than 400 studies conducted around the world, involving tens of thousands of women.
It found that the overall risk of metastasis is between 6% and 22%, with younger women having a higher risk.
While women aged 50 years or older when they were diagnosed with breast cancer have a risk of developing metastasis that ranged from 3.7% to 28.6%, women diagnosed with breast cancer before age 35 had a higher risk — 12.7% to 38%. The investigators speculate that this may be because younger women have a more aggressive form of breast cancer or because they are diagnosed at a later stage.
The risk of metastasis also varies by tumor type, with luminal B cancers having a 4.2% to 35.5% risk of metastasis vs a 2.3% to 11.8% risk with luminal A tumors.
"The quantification of recurrence and disease progression is important to assess the effectiveness of treatment, evaluate prognosis, and allocate resources," commented lead investigator Eileen Morgan, PhD, of the International Agency for Research on Cancer.
Morgan and colleagues presented the new meta-analysis at the virtual Advanced Breast Cancer Sixth International Consensus Conference.
She added that this information has not been available until now "because cancer registries have not been routinely collecting this data."
In fact, the US National Cancer Institute began a project earlier this year to track this information, after 48 years of not doing so.
Reacting to the findings, Shani Paluch-Shimon, MBBS, director of the Breast Unit at Hadassah University Hospital, Jerusalem, Israel, commented that this work "provides the first reliable estimate of how many breast cancer patients go on to develop advanced disease in contemporary cohorts."
"This information is, of course, important for patients who want to understand their prognosis," she continued.
"But it's also vital at a public health level for those of us working to treat and prevent advanced breast cancer to help us understand the scale of the disease around the world," she said. "It will help us identify at-risk groups across different populations and demonstrate how disease course is changing with contemporary treatments.
"It will also help us understand what resources are needed and where, to ensure we can collect and analyze quality data in real-time as this is key for resource allocation and planning future studies."
The work was funded by a grant from the Susan G. Komen Foundation.
Advanced Breast Cancer Sixth International Consensus Conference: Abstract Abstract OR91. Presented October 15, 2021.
Source: https://www.medscape.com/viewarticle/962289?uac=21...
-
Which Fully Vaccinated Adults Are Most at Risk of Severe COVID?
— Study examines which factors did, and didn't, play a role in risk
A significant proportion of all fully vaccinated adults who died of COVID-19 had at least four risk factors associated with severe outcomes, researchers found.
In addition to older age (65 and up) and being immunosuppressed, having chronic kidney, cardiac, pulmonary, neurologic, or liver diseases, as well as diabetes, were all associated with higher odds of severe COVID outcomes, and 77.8% of fully vaccinated adults who died had at least four of these risk factors, reported Sameer Kadri, MD, of the NIH Clinical Center in Bethesda, Maryland, and colleagues in the Morbidity and Mortality Weekly Report.
However, there were no increased odds of severe outcomes associated with sex, race/ethnicity, time since primary vaccination, or whether the infection occurred during the Delta variant wave.
Kadri and team examined data from 465 U.S. healthcare facilities in the Premier Healthcare Database Special COVID-19 Release from December 2020 to October 2021, which included adults who were either fully vaccinated, received a third dose as part of their primary series, or received a booster dose after their primary series. Severe outcomes were defined as hospitalization with acute respiratory failure, non-invasive ventilation, ICU admission, and death.
Overall, 1,228,664 adults completed a primary vaccination series, and of those, 2,246 contracted COVID-19. Of these, 327 were hospitalized, 189 had a severe outcome, and 36 had a COVID-related death.
Not surprisingly, older age was associated with a higher risk of death (adjusted OR [aOR] 3.22, 95% CI 1.81-5.74), as was immunosuppression (aOR 1.91, 95% CI 1.37-2.66).
Of the six conditions, chronic pulmonary disease (aOR 1.69, 95% CI 1.31-2.18), liver disease (aOR 1.68, 95% CI 1.12-2.52), and kidney disease (aOR 1.61, 95% CI 1.19-2.19) were associated with the highest odds of severe outcomes.
Interestingly, Pfizer vaccine recipients had comparable risks of severe outcomes to those who received the Johnson & Johnson vaccine (aOR 0.70, 95% CI 0.39-1.26), while these risks were lower for those who received Moderna (aOR 0.56, 95% CI 0.32-0.98).
Kadri and colleagues noted that all adults with severe COVID outcomes had at least one of the eight risk factors. Only 19% of all adults with four or more risk factors had non-severe outcomes, while 57% had respiratory failure or were admitted to an ICU.
Among 36 adults who died, 15 had do-not-resuscitate orders at the time of hospital admission, and nine were discharged to hospice.
The authors noted that these results may not be applicable to time periods when other variants were predominant in the U.S.
Source: https://www.medpagetoday.com/infectiousdisease/cov...
Primary Source
Morbidity and Mortality Weekly Report
{Strangely, this article actually made me feel a little better. Of the over 1.2 million people diagnosed with covid, few actually died. Those who did tended to have multiple co-morbidities.}
-
Risk for Breast Cancer Recurrence Persists Past 30 Years
For the first time, new data show that risk for breast cancer recurrence extends past 30 years.
The data come from a Danish study involving 20,315 women who were treated for early operable breast cancer between 1987 and 2004, and all of whom were disease-free at 10 years.
Further follow-up showed that 2595 women had a breast cancer recurrence more than 10 years after their primary diagnosis.
The cumulative incidence of recurrence was 8.5% at 15 years; 12.5% at 20 years; 15.2% at 25 years, and 16.6% at 32 years.
Recurrence risk was greatest early in the study period.
Women who had primary tumors larger than 20 mm, lymph node-positive disease, and estrogen receptor-positive tumors were at higher risk for late recurrence.
"Such patients may warrant extended surveillance, more aggressive treatment, or new therapy approaches," said the investigators, led by Rikke Pedersen, MD, a PhD candidate in epidemiology at Aarhus University Hospital in Denmark.
"Our observed high cumulative incidence of late breast cancer recurrence is a concern given the increasing prevalence of long-term survivors." Among other things, a new model to better select women for prolonged surveillance is needed, they said.
The new findings were published online November 8 in the Journal of the National Cancer Institute (NCI).
This study confirms previous investigations, but it is the first to report that breast cancer can recur more than 30 years after diagnosis, note the authors of an accompanying editorial, Serban Negoita, MD, DrPH, and Esmeralda Ramirez-Peña, PhD, MPH, both from the National Cancer Institute.
The caveat is that treatment has evolved considerably since the women in the study were diagnosed, so the prognostic value of the findings with current treatment regimens is uncertain, they note. Some studies haven't found a recurrence benefit for aggressive upfront treatment, but those studies had shorter follow-ups.
Research into the issue is "increasingly important" to guide clinical management and counsel women who are living longer after their primary diagnosis, they comment.
Further Details from the Study
Data for the study came from the Danish Breast Cancer Group clinical database and other national databases. The researchers focussed on women who were disease-free at 10 years after their primary diagnosis, which was stage I or II disease. Median age was 55 years.
Cumulative incidence for breast cancer recurrence was highest for grade 1 tumors with four or more positive lymph nodes (37.9% 10-25 years after the primary diagnosis) and was lowest for patients with grade 3 disease and no involved lymph nodes (7.5%).
The finding of higher recurrence incidence with lower grade tumors goes against some previous reports, the researchers commented. It may be that some tumors considered lower risk decades ago, and treated accordingly, would be considered higher risk in more recent times.
The cumulative incidence of late recurrence was also higher in younger patients and those treated with breast-conserving surgery instead of mastectomy, the team reported.
Adjusted hazard ratios followed the incidence trends, with higher hazards of recurrence for women diagnosed before age 40 as well as those who had breast-conserving surgery, four or more positive lymph nodes, and primary tumors 20 mm or more across.
The work was funded by the Danish Cancer Society and Aarhus University. Lead author Pedersen reports no disclosures, but co-authors report ties to Amgen, Novo Nordisk, Roche, and other companies. The editorialists have disclosed no relevant financial relationships.
J Natl Cancer Inst. Published online November 8, 2021. Abstract, Editorial
-
GnRHa Therapy Protects the Ovaries of Young Women With Breast Cancer Having Chemo
NEW YORK (Reuters Health) - Treatment with a gonadotropin-releasing hormone analog (GnRHa) during chemotherapy in premenopausal women with breast cancer reduces ovarian impairment, according to a randomized controlled trial conducted in China.
Studies on the use of GnRHa therapy to protect ovarian function have shown "mixed results" for a variety of reasons, Dr. Xiangyun Zong of Shanghai Jiao Tong University Affiliated Shanghai Sixth People's Hospital and colleagues note in JAMA Oncology.
To investigate, they did an open-label trial involving 330 women aged 18 to 49 years with operable breast cancer for which treatment with adjuvant or neoadjuvant cyclophosphamide-containing chemotherapy was planned.
Half underwent chemotherapy without and half with GnRHa therapy, which consisted of 3.6 mg of goserelin or 3.75 mg of leuprorelin by subcutaneous injection once every 28 days from one to two weeks before the first cycle of chemotherapy to four weeks after the last cycle of chemotherapy.
At 12 months after the completion of chemotherapy, the rate of premature ovarian insufficiency was significantly lower in the GnRHa group than the control group (10.3% vs. 44.5%; odds ratio, 0.23; P<0.001). Premature ovarian insufficiency was defined as anti-Muellerian hormone levels of less than 0.5 ng/mL.
Anti-Muellerian hormone resumption at 12 months was significantly more common in the GnRHa group than in the control group (15 of 25 vs. six of 44; odds ratio, 4.40; P<0.001).
After a median follow-up of 49 months, there were no between-group differences in four-year overall survival and tumor-free survival (secondary endpoints). However, a post hoc analysis indicated that GnRHa was associated with improved tumor-free survival in patients younger than 35 years.
Based on their findings, the researchers say GnRHa therapy "should be used to protect ovarian function in premenopausal women who are receiving chemotherapy for breast cancer."
This study had no commercial funding, and the authors report no conflicts of interest.
SOURCE: https://bit.ly/32K0yEf JAMA Oncology, online December 30, 2021.
Reporting at: https://www.medscape.com/viewarticle/965865?uac=21...
-
Wow, what a clinical trial and results for mTNBC with trilaciclib!!!
https://clincancerres.aacrjournals.org/content/ear...
Saulius
-
Early (but interesting-- a new approach) research...
Researchers reduce breast cancer metastasis in animal models by modifying tumor electrical properties [using drugs]
Amiodarone, an ion channel blocker approved for other diseases, significantly inhibits tumor cell invasion
In normal cells, electrical voltage patterns provide a blueprint for orderly growth. But with cancer, the opposite happens. Marked by a breakdown in the normal electrical patterns generated by the cells, they lose their specialized functions, start expanding into a tumor and spreading into and disrupting the function of other tissues -- metastasis. As of yet, there are no clinically available treatments that specifically target the process of metastasis, which remains the leading cause of death in cancer patients.
Now researchers at Tufts University have found that manipulating voltage patterns in tumor cells using ion channel blockers already FDA-approved as treatments for other diseases can in fact significantly reduce tumor cell invasion in a dish and metastasis in an animal model of breast cancer...
-
RE the trilaciclib!!! trial,
does that mean that TNMBC people got a year or more out of this drug and then they went to to chemo?
-
2019whatayear - one arm just got chemo, the other arms were getting chemo and the trilaciclib either on same day or the trilo a day ahead.
" 34 to group 1 (GCb on days 1 and 8), 33 to group 2 (trilaciclib and GCb on days 1 and 8), and 35 to group 3 (trilaciclib days 1 and 8, and trilaciclib and GCb on days 2 and 9). "
GCb = gemcitabine plus carboplatin
full text is here https://clincancerres.aacrjournals.org/content/cli...
-
thanks moth. Damn
-
Yes 2019whatayear, chemo, but still... another promising combo/line for mTNBC, and we always want more of them! The plots (group 2: OS not reached!!!) are simply "music to my ears". Saulius
-
Oh Saulius so not reached in this case means participants in group 2 are still out there living life?
-
Gene expression profiles of breast cancer metastasis according to organ site
https://febs.onlinelibrary.wiley.com/doi/10.1002/1...
this study looked at the genes in various metastatic sites to determine if expression was same or different. Lots of interesting tidbits but also pretty familiar results regarding OS
"Median OS was 63.8 months in patients with HR+/HER2-negative disease, 35.5 months in patients with HER2+ disease, and 22.1 months in patients with TNBC"
"Median OS was 99.7 months for luminal A, 63.6 for luminal B, 34.7 months for HER2-enriched, and 22.4 months for basal-like."
-
Thought I would post this here in case anyone is interested:
The eReach Study: A Randomized Study of an eHealth Delivery Alternative for Cancer Genetic Testing for Hereditary Predisposition in Metastatic Breast, Ovarian, Prostate and Pancreatic Cancer Patients.
The University of Pennsylvania is conducting the eReach Study to look at how to best help cancer patients understand and get genetic testing.
If you live in the United States and have metastatic breast cancer, metastatic prostate cancer, advanced pancreatic cancer, or advanced ovarian cancer, and you haven't had genetic testing for a hereditary cancer syndrome, you may be eligible to receive free genetic counseling by participating in the eReach Study.
Read more here:
https://redcap.med.upenn.edu/surveys/?s=MY7H37TM7W...
-
Cancer treatment may inhibit immune response to COVID-19 vaccination
January 20, 2022
JACKSONVILLE, Fla. — A study by researchers at Mayo Clinic Cancer Center has found that patients with cancer who receive chemotherapy ― and some targeted therapies, such as CDK4/6 inhibitors and therapies targeted at B cells ― may mount an inadequate immune response to COVID-19 vaccination. The findings are published in Mayo Clinic Proceedings: Innovation, Quality & Outcomes.
"It is important for patients with cancer who are receiving chemotherapy to receive a COVID-19 vaccine," says Saranya Chumsri, M.D., a Mayo Clinic hematologist and oncologist, and author of the paper. Dr. Chumsri says this advice also applies to patients with cancer who are taking a CDK 4/6 inhibitors. These inhibitors are a newer class of medicines used to treat hormone-receptor-positive and HER2-negative breast cancers.
Dr. Chumsri says that while CDK 4/6 inhibitors are not conventionally considered to be as immunosuppressive as chemotherapy, her research on patients with breast cancer who take these drugs found that they exhibited less optimal neutralizing antibody activity. Dr. Chumsri recommends that antibody levels be tested in these patients after vaccination, and they should consider receiving booster vaccinations for COVID-19.
Dr. Chumsri anticipates having additional data later this year regarding broader immune responses to COVID-19 vaccinations, including cellular and antibody responses in patients receiving chemotherapy and targeted therapies with booster vaccinations.
Read it here: https://newsnetwork.mayoclinic.org/discussion/canc...
Research published here: https://www.mcpiqojournal.org/article/S2542-4548(21)00173-9/fulltext (pre-publication proof)
DOI: https://doi.org/10.1016/j.mayocpiqo.2021.12.004
{I note that this says "Chumsri recommends that antibody levels be tested in these patients after vaccination..." I have not found docs willing to order this test, chiefly because they state that the information is not actionable/they don't know what to do with it. Perhaps as evidence accumulates, this approach will change. There is a self-pay/self-help test available through LabCorp. It seems semi-actionable to me: I realized it is no guarantee, but if antibodies are low, one would know to be especially careful about risk and exposure. Access to all sources free of charge as of posting.}
-
yes, I went and got the LabCorp antibody test on my own, just to make sure I had developed antibodies. My count was in the 300s
-
I got the LabCorp test, too. Mine were >2500. No guarantee, but I was pleased and relieved.
-
Did your doctor give you the antibody test or is this an at home test kit?
-
I registered on the lab Corp website. Their doctor writes the order and you go to a Lab Corp location for the blood draw.
Covered by myinsurance except for the small website fee $15 I think it was.
Link - https://www.labcorp.com/coronavirus-disease-covid-19/individuals/antibody-test
Lumpie wow >2500 that's great. My sister did hers at the same time and her result was over 700. My infusion nurse said hers was only in the 200s -
Ditto. My doc would not prescribe, that is why I did the "no order in hand" option through LabCorp. As Olma61 says, register, if you have not already done so, on LabCorp's site. Then you have to find the correct test. It can be a little tricky. You can find it in the test menu (one of the tabs near the top of the main page). Their doc will write the Rx for the test if your doc has not provided one. They charged me a $6 fee for that service. It is not an at home test. You must go to LabCorp for a blood draw. Results are delivered through the LabCorp website. Interestingly, my insurance did pay for the test. I wa surprised.
Test name is "SARS-CoV-2 Semi-Quant Total Ab" (if seacrching by name, I had to shorten the name to "SARS-CoV-2 Semi-Quant" to get anything to come up.)
Test # is 164090
There is another very similarly named test for IgG rather than "total" antibodies. The descriptions do not make it entirely clear why you'd want total rather than IgG. I had the impression that back before the vaccines, the IgG test was an indicator of prior but cleared infection. I suppose the "total" test might count IgM, too. But I am not entirely sure about this reasoning/analysis. I ordered the above because it made sense to me and was the one that was recommended through my local MBC cancer buddies network.
Note: I have been advised that you should wait at least 30 after getting a vaccine or booster to have this test. I waited >90 days.
I was very pleased with the >2500, especially since I am on active chemo. An MBC buddy said hers were around 900. She is not on active chemo but gets a targeted therapy and is otherwise in good health. I think that some of the hard-to-account for discrepancies in results are one reason clinicians have some concerns about relying too heavily on this test. I think it is fair to say it just gives us a sense of where we are on a given day.... and it is a snapshot since the studies seem to be indicating that our immunity may wane over time... hense all the boosters....
Good luck and stay healthy out there!
-
Thanks for the information Lumpie and Olma61
-
How do you know if you are Luminal A or Luminal B or other ?
thanks
-
this article helps explain those subtypes
https://www.breastcancer.org/symptoms/types/molecular-subtypes
-
olma61-thanks. Very clear article, a k67 was never done on my original cancer biopsy, so I guess I am never going to know whether mine is A or B.
-
Nkb me either, but it did say that A is typically lower grade, which mine was, so I'm assuming I'm A. Not much difference between A & B anyway
-
Nkb, I always understood that if you are hormone positive and HER2 negative, you are Luminal A; hormone positive and HER2 positive, you are Luminal B. You probably know that from your patho report. I suppose that if you are HER2 negative with high levels of Ki-67, but they did not comment on Ki-67 in your patho report, that could present a twist (uncertainty), but in most cases, I think your patho report will give you this info. Things change over time, especially with the emergence of genomic analysis, so maybe this is over- simplified. Hope you find some certainty/reassurance.
-
Lumpie- thanks. At the appt to discuss the path report (10 years ago) I asked about k67 and the surgeon said it wasn’t done. That they weren’t doing them as much. I heard that many MOs don’t find them as consistent so don’t do them. I was Her2 negative but recently looked again and was 2+ so basically Her 2 low.
I’m not stressed, just curious. The only mutation I have that Iknow of (CCND1) wasn’t listed in the article- but, overall super interesting article.
-
Nkb, did they ever test your HER2 by FISH? Mine was also 2+ by IHC so they sent it for further analysis by a more sophisticated test “FISH”. I was still in the grey zone and had several pathologists weigh in on whether I’d benefit from HER2 targeted therapy, ultimately it was decided that I should be treated as negative. If they never tested your HER2 status beyond the equivocal 2+, that might be something to ask your MO about. The HER2 targeted therapies have experienced great advancements and so it seems more important than ever to take a closer look at cases that might be positive by FISH
-
There is some overlap between the luminals & hormone markers but it's not a 100%. for ex this study below found that some triple negs were not basal.
& in metastatic cancer, there is a difference in survival curves for luminal a, luminal b and basal
"Median OS was 99.7 months for luminal A, 63.6 for luminal B, 34.7 months for HER2-enriched, and 22.4 months for basal-like."
https://community.breastcancer.org/forum/73/topics...
-
Triple Neg has other subtypes too... 4-6 depending who is grouping them. If you go a genetic assay scattergram you can see the clusters of the different types but multiple genes control it.
basal-like 1 (BL1), basal-like 2 (BL2), mesenchymal (M), mesenchymal stem–like (MSL), immunomodulatory (IM), and luminal androgen receptor (LAR)
-
JennyJo20- yes, they FISH tested it and it was negative.
I’ve heard that Herceptin is very weak compared to for example Enhertu- and doesn’t work on Her 2 low- but Enhertu works on about 35% of Her2 low.
My UCSF second option MO says in biopsying again for an Enhertu study no one who was 2+ at primary turned negative although some 1+ people did.
Interesting about all the triple negative subtypes.
-
Probiotic Supplement Attenuates Chemotherapy-Related Cognitive Impairment in Patients With Breast Cancer
- This randomized, double-blind, placebo-controlled trial showed that a probiotic supplement attenuated the incidence of chemotherapy-related cognitive impairment (CRCI) in patients with stage I–III breast cancer who underwent chemotherapy. No measurable side effects were found during the treatment. Disease-free survival and death rates in the probiotic group were slightly better numerically but not significantly than those in the placebo group.
- Probiotic supplementation during chemotherapy is a simple, inexpensive, safe, and effective intervention for the prevention of CRCI. Impact on long-term outcomes or survival warrants further trial study with a large sample size.
Article: European Journal of CancerProbiotic supplement attenuates chemotherapy-related cognitive impairment in patients with breast cancer: a randomised, double-blind, and placebo-controlled trial
Eur. J. Cancer 2022 Jan 01;161(xx)10-22, Z Juan, J Chen, B Ding, L Yongping, K Liu, L Wang, Y Le, Q Liao, J Shi, J Huang, Y Wu, D Ma, W Ouyang, J TongDOI:https://doi.org/10.1016/j.ejca.2021.11.006Abstract: https://www.ejcancer.com/article/S0959-8049(21)01216-8/fulltext{Reporting and abstract: free access; full journal article requires fee or subscription. IDK about you, but any news about improving on chemo brian is welcome to me! I have been taking a probiotic to help with intestinal distress for almost a year now. It has helped my intestinal situation dramatically. My chemo brain has also improved. I thouht it was time/coincidence, but maybe the probiotic is improving things.} -
A new paper has been published about ErSO. From the abstract...
"While ErSO has promise as a new drug, it has effects on ERα-negative (ERα−) cells in certain contexts. Herein, we construct modified versions of ErSO and identify variants with enhanced differential activity between ERα+ and ERα– cells. We report ErSO-DFP, a compound that maintains antitumor efficacy, has enhanced selectivity for ERα+ cancer cells, and is well tolerated in rodents."
Unfortunately, still no signs it will make it into clinical trials in the near term.
https://pubs.acs.org/doi/10.1021/acs.jmedchem.1c01...
-
New mammogram measures of breast cancer risk could revolutionise screening
Abstract/What's new? dtd 16 November 2020
Mammographic density, or the area of the mammogram which appears white or bright, has well-established associations with breast cancer risk. The authors call this Cumulus due to the computer-assisted technique for measuring that density. Here, the authors introduce two novel measurement techniques, Cirrus and Cirrocumulus, for extracting risk information from mammograms. Cirrocumulus is based on image brightness and Cirrus is based on texture. When combined, these measures substantially improve risk prediction beyond that of Cumulus. In addition, the new risk measures outperformed the recently published polygenic risk score. By obtaining more information from mammograms, these tools could improve personalized risk recommendations for screening.
Reporting: dtd 23 Dec 2020
World-first techniques for predicting breast cancer risk from mammograms that were developed in Melbourne could revolutionise breast screening by allowing it to be tailored to women at minimal extra cost.
Published in the International Journal of Cancer, the University of Melbourne-led study found two new mammogram-based measures of risk. When these measures are combined, they are more effective in stratifying women in terms of their risk of breast cancer than breast density and all the known genetic risk factors.
Researchers say if successfully adopted, their new measures could substantially improve screening, make it more effective in reducing mortality and less stressful for women, and therefore encourage more to be screened. They could also help address the problem of dense breasts.
Since the late 1970s, scientists have known that women with denser breasts, which shows up on a mammogram as having more white or bright regions, are more likely to be diagnosed with breast cancer and to have it missed at screening.
Collaborating with Cancer Council Victoria and BreastScreen Victoria, University of Melbourne researchers were the first to study other ways of investigating breast cancer risk using mammograms.
Using computer programs to analyse mammogram images of large numbers of women with and without breast cancer, they found two new measures for extracting risk information. Cirrocumulus is based on the image's brightest areas and Cirrus on its texture.
First, they used a semi-automated computer method to measure density at the usual, and successively higher levels of brightness to create Cirrocumulus. They then used artificial intelligence (AI) and high-speed computing to learn about new aspects of the texture (not brightness) of a mammogram that predict breast cancer risk and created Cirrus.
When their new Cirrocumulus and Cirrus measures were combined, they substantially improved risk prediction beyond that of all other known risk factors.
Lead researcher and University of Melbourne Professor John Hopper said that in terms of understanding how much women differ in their risks of breast cancer, these developments could be the most significant since the breast cancer genes BRCA1 and BRCA2 were discovered 25 years ago.
"These measures could revolutionise mammographic screening at little extra cost, as they simply use computer programs," Professor Hopper said.
"The new measures could also be combined with other risk factors collected at screening, such as family history and lifestyle factors, to provide an even stronger and holistic picture of a woman's risk.
"Tailored screening – not 'one size fits all' – could then be based on accurately identifying women at high, as well as low, risk so that their screening can be personalised.
"Given mammography is now digital, and our measures are now computerised, women could be assessed for their risk at the time of screening – automatically – and given recommendations for their future screening based on their personal risk, not just their age."
Professor Hopper said this information could be used to ease pressure on BreastScreen, which had to close for a period during the COVID-19 pandemic and is looking for ways to best handle the backlog while continuing to provide a valuable service with limited resources.
He said the current breakthrough could not have occurred without the extraordinary support his mammogram research had received from the National Breast Cancer Foundation, starting with its first funding round more than 20 years ago.
"Only around 55 per cent of Australian women aged 50-74 currently present for screening aimed at detecting breast cancers early," he said.
"Knowing that screening could also give an accurate risk prediction could encourage more women to take up the offer of free screening. Women with high risk based on their mammogram would also benefit greatly from also knowing their genetic risk."
Adjunct Associate Professor Helen Frazer, Clinical Director of St Vincent's BreastScreen Melbourne, said that improvements in assessing a woman's risk of breast cancer would be transformative for screening programs.
"Using AI developments to assess risk and personalise screening could deliver significant gains in the fight against breast cancer," Adjunct Associate Professor Frazer said.
The study involved participants in the Melbourne Collaborative Cohort Study run by Cancer Council Victoria, and the Australian Breast Cancer Family Study and Twins Research Australia run from the University of Melbourne.
Participating women filled out a questionnaire and allowed researchers to access their mammograms from BreastScreen, with other providers or their own copies.
This work was conducted by Dr Kevin Nguyen at the University of Melbourne, whose ground-breaking PhD uncovered the Cirrocumulus measure, and is a continuing collaboration with researchers from Seoul National University in South Korea.
Researchers from Monash University, University of Hawaii Cancer Center, University of Pisa and University of Western Australia also contributed to the study.
Reporting: https://about.unimelb.edu.au/newsroom/news/2020/de...
Abstract: https://onlinelibrary.wiley.com/doi/10.1002/ijc.33...
Journal: https://onlinelibrary.wiley.com/doi/full/10.1002/i...
https://doi.org/10.1002/ijc.33396
{Abstract and reporting are free. Full journal article requires fee or subscription.}
-
Anthracyclines for HER2+ Breast Cancer: Are We Ready to Let Them Go?
"The role of anthracyclines for early HER2-positive BC appears limited in an era of highly effective HER2-directed therapies. De-escalation of (neo)adjuvant regimens is possible and safe, by using paclitaxel and trastuzumab or trastuzumab emtansine for small tumors and by using taxane- and platinum-based neoadjuvant regimens for larger tumors, including those with high-risk features.
Omitting anthracyclines can result in a substantial reduction in potential serious toxicities, while still achieving optimal treatment outcomes. Several additional de-escalation trials are currently ongoing and may allow for even further reduction in toxicity of treatment, ultimately allowing us to maximize the benefit of chemotherapy while minimizing its undesired impact on the quality of life of our patients."
-
That sounds very exciting Laughing Gull, I hope that is the case!
-
A New Solution for Long-COVID Brain Fog?
Noninvasive brain stimulation (NIBS) that uses alternating microcurrents appears to rapidly and effectively improve cognitive and visual deficits related to "long COVID," a small case series shows.
SARS-CoV-2 infections impair blood flow to the eyes and brain, causing visual and cognitive deficits, and the stimulation restores normal blood flow....
"Oxygen and glucose is delivered again to nerve cells, so they can do their job of firing electric signals to the brain, and the patient can think better, their cognition is better, and their vision is improved."
The benefits for those affected with long-term cognitive problems occur within days.... "This Is the fastest solution that I'm aware of ― much faster than with the standard neurological rehabilitation."
The study was published in a recent issue of Restorative Neurology and Neuroscience.
Reporting: https://www.medscape.com/viewarticle/968290#vp_1
Journal article: https://content.iospress.com/articles/restorative-...
DOI: 10.3233/RNN-211249
{This is about covid brain fog, but anybody who says "brain fog" has my attention. Makes me wonder if these therapies could help those of us suffereing from chemo-related brain fog as well. We must hope (and perhaps advocate) for clinical trials. Access to reporting and journal article are both without charge. Reporting may require registration.}
-
That caught my eye too in terms of chemo brain, but it was a study of only two patients. Something to investigate further for sure.
-
"HER2-positive breast cancer progressively turned from the most feared to the most curable subtype. Currently, more than 9 out of 10 patients with HER2-positive breast cancer who are treated with chemotherapy and HER2-blockade are free from recurrence 6 years after surgery."
Woot woot!!! What great advancements!! Let's hope this becomes the norm for all subtypes asap!
More Tolerable Cures for Patients With Early-Stage HER2-Positive Breast Cancer: Halfway to Precision
https://dailynews.ascopubs.org/do/10.1200/ADN.22.2...
-
"overall survival data from MONALEESA-2, breaking the 5-year mOS barrier for patients with metastatic HR+ breast cancer"
-
Accelerated Partial Breast Irradiation using External-Beam or Intraoperative Electron Radiotherapy: 5 year oncological outcomes of a prospective cohort study
this is for rads post lumpectomy for IDC or DCIS
" Ipsilateral breast tumor recurrences and locoregional recurrence rates were unexpectedly high in patients treated with IOERT" 10.6% recurrence in the IORT group v 3.7% in accelerated partial breast rads
https://www.redjournal.org/article/S0360-3016(22)00243-7/fulltext
-
Treatment and Survivorship Interventions to Prevent Poor Body Image Outcomes in Breast Cancer Survivors
https://www.dovepress.com/treatment-and-survivorship-interventions-to-prevent-poor-body-image-ou-peer-reviewed-fulltext-article-BCTT
This might have already been posted, but I read it in detail yesterday. I think it's crucial that the BC medical community really spends time realizing that taking care of the whole person overrides what I still have seen as the knee jerk reaction to just annihilate the cancer with secondary regard to the aftermath of a woman who must live with decisions that can be made without us being prepared with the right questions or coming to an agreement with the best possible treatment.
Here are the major sections:
We Shared Decision-Making
Local Therapy De-Escalation
Axillary Downstaging
Radiation
Systemic Therapy
Lymphedema Risk Mitigation
Preventing and Managing Weight Gain During Treatment
Prehabilitation
Addressing Menopausal and Sexual Sequelae of Treatment
Psychological Interventions During Treatment
I feel strongly that these subjects need to be incorporated into the care of every newly diagnosed BC patient. I've gotten so much of this support and preparation from being here, but not everyone knows about options until they have made permanent decisions with what still seems to be a traditional approach that is a decade behind current best practices. As a person living in a city without a major breast care integrated care system, I still prefer to piece the right solution for me into what we have here. I may still end up traveling. But knowing that treating my cancer has options that require shared decisions is both empowering and unnerving for me. My BCS is in line with my approach, but for now, we may lack oncoplastic expertise that can keep be here.
-
[trial in mice] World first: drug prevents human breast cancer recurrence and metastasis (article headline)
From the actual paper's abstract:
"We previously provided in vitro evidence that these features are collectively enforced by mitochondrial superoxide in a paradigm where mitochondria act as metabolic sensors of the tumor microenvironment and produce subcytotoxic levels of superoxide to prime metastatic progenitor cells. We also showed that these metastatic traits can be collectively countered by MitoQ, a mitochondria-targeted antioxidant that selectively deactivates mitochondrial superoxide. Here, we further establish that MitoQ prevents primary tumor recurrence after surgery, tumor take and metastasis as a whole, notably in a model of human breast cancer in mice. Since MitoQ already successfully passed Phase I clinical trials, our findings support the development of this drug as a preventive treatment against breast cancer metastasis."
This patented substance (MitoQ), which is available OTC as a supplement, was selected for trial based on their theorized mechanism of action (suppressing subcytotoxic mitochondrial superoxide) by researchers with no connection to the company -- in part because MitoQ had already gone through Phase I trials (rather than mitoTEMPO which is public domain but also showed good results with it in melanoma). FWIW, I found the paper clearer than the EurekaAlert article.
-
Research done in Montreal could lead to treatment for [TNBC]
[Using CRISPR to knock out genes systematically, researchers identified two signalling pathways or gene networks of significance in TNBC.]
"One of them was an oncogenic pathway. Those are genes that normally promote cell proliferation on tumours and this one was hyperactivated in those breast cancer patients," Lebrun said.
The second group of genes, which normally act as tumour suppressors by preventing cells to multiply, were found to be inactive or asleep.
This combination, Lebrun believes, could explain why TNBC tumours are so "aggressive and metastatic."
Understanding which genetic mechanisms were involved allowed the team to then uncover existing drugs that targeted those networks.
One of the drugs they tested, Verteporfin, surprisingly had nothing to do with cancer.
"It's actually a drug that is used for disease of the degeneration of the retina. It's an eye disease," Lebrun said... In all, the team evaluated around 10 different drugs, with Verteporfin being one of two standouts... Individually, each [of those two] drug[s] had around a 20 per cent decrease in tumour growth... "But [together] we got something more like 80 per cent," he said. "That's what we call a synergistic effect."
Efforts have been underway since the summer to get Phase 1 clinical trials off the ground... [but] Lebrun said he couldn't give a timeline of when the trial would start and when patients could begin enrolling.
-
Warmer Climate Tied to Favorable Breast Cancer Outcomes
Higher environmental temperatures are associated with better outcomes (significant improvements in pCR as well as OS) among patients with stage I-III breast cancer, according to research presented in a poster at the NCCN 2022 Annual Conference.
-
onmagosh... debbew.... your post made my day. Is this an excuse to spend the winter in a warm climate? (Access to care issues aside)
I am such a wimp about the cold and by this time of year, I am ready to petition for no more winter! Now I have a therapeutic excuse. Love it! -
Lumpie, debbew, & moth:
Thanks for keeping this thread active and informing the community on all the research that's out there. This is such a helpful thread
-
Lumpie, I was quite surprised to see that article, too! I wondered if it had anything to do with vitamin D, but that doesn't seem to be what they are thinking.
Norcals, thanks for the nod! Lumpie has led the way but I'm always interested to see what all the other posters have uncovered.
-
debbew That's great news! I went through all my treatments, surgery during the hottest Florida months May - September
-
timing of chemo - as in morning or afternoon- may affect outcomes
"patients who received most treatments after noon required fewer dose reductions and were less likely to stop treatment.
In addition, recurrence rates were highest among patients who received at least 70% of treatments before noon."
https://www.cancertherapyadvisor.com/home/news/con...
-
test
-
test
-
Cardamonin shows promise for treating aggressive breast cancer
Study shows that compound from cardamom spice can kill triple-negative breast cancer cells
-
Hepatic Resection for Breast Cancer–Related Liver Metastases
Published in Metastatic Breast Cancer
Journal Scan / Research · April 11, 2022
- This retrospective study from a single institution described the outcomes of patients undergoing liver resection for breast cancer–related liver metastases and identified any clinicopathological variables associated with recurrence or survival. The findings showed that among 20 patients with breast cancer–associated liver metastases, hepatic resection was associated with a median disease-free survival of 50 months and a 5-year OS of 65%.
- {A} Few patients may benefit from hepatic resection for breast cancer–related liver metastases and this approach appears to be feasible and safe.
- CONCLUSIONS: This study has demonstrated that liver resection for breast cancer-related liver metastases is feasible, safe and associated with prolonged disease free and overall survival in selected patients. It is likely that this option will be offered to more patients going forward, however, the difficulty lies in selecting out those who will benefit from liver resection particularly given the increasing number of systemic treatments and local ablative methods available that offer good long-term results.
{Summary, abstract and full article all appear to be free of charge.} -
Hi All, been a while since the crash and just catching up.
I've had some progression and my MO is suggesting Vinorelbine as next step. However I can't find ANYTHING positive about this drug…apart from it being effective in a mouse trial ina combo to tackle brain mets. It's old, it doesn't seem to be particularly effective and has been 'relegated' to later stage treatment. Does anyone have anything positive on this drug to share? -
karenfizedbo15, I am so sorry to hear about your progression and concern over drugs. I have taken Vinorelbine. I was on the Aviator trial and got Group B: Trastuzumab + Vinorelbine + Avelumab. It did not help me and I "progressed" off of it really quickly. Sorry that is probably not very encouraging. It looks to me like the trial is still recruiting (https://clinicaltrials.gov/ct2/show/NCT03414658) so it must be working for some people. You might check out the trial. Looks like you are triple + so IDK if that fits with their recruitment. I don't recall it being particularly hard to tolerate. I do think I lost my hair, but that sort of goes with the territory at this point. Next I was on Kadcyla, as part of the DS-8201 clinical trial (control arm), and it did not work for long for me and had some ugly side effects. Then we irradiated my brain and liver (Cyberknife) and I went on DS-8201/Enhertu. The combo has kept things under control thus far. Sure hope you find some thing that is tolerable and works well for you!
-
Thanks Lumpie! I’m ER+ and HER2+. You story seems to be the norm, that I can find. Checked the trial link but it’s showing an error. It is encouraging that you’ve managed to find SOMETHING to keep you stable though!
-
Thanks, karenfizedbo15. In case you or any others readers are searching, the Aviator trial is: ClinicalTrials.gov Identifier: NCT03414658. Yes, anything to keep us stable. Thankfully, lots of people having luck on Enhertu. It has some challenging SE's, but for a lot of people, it works. Good luck!
-
I see this thread is a bit quieter... let's revive it! Some very good news on TDX-D for her2low (IHC +1/+2): https://www.onclive.com/view/fda-grants-breakthrou...
Saulius
-
Interesting in-animal study for cyclophosphamide+CSF1R-inhibitor in mTNBC. Some macrophages inhibition mechanisms... Hope such things come into clinical trials sooner than later: https://scienmag.com/a-promising-combination-thera...
Saulius
-
With some of these articles, I need Cliff Notes For Dummies, if there is such a thing!
-
Dear Homemom, Cliff Notes for Dummies would be useful for me too:)D I also sometimes feel they write these articles only for a few selected people - nothing has changed since times of Socrates:)
Saulius
-
NUS scientists develop painless way to shrink breast cancer using magnetic fields
https://www.straitstimes.com/singapore/health/nus-...
-
The most detailed photograph of a cell inner: https://angstrom3d.com/cst-molecular-landscapes
Man... how complicated life really is:/
Saulius
-
Observing ESMO: extremely interesting results in mTNBC BEGONIA clinical trial: 1st line Durvalumab+Dato_DXd = 74% ORR irrespective of PD-L1 status. Amazing!
-
I’m wondering if anyone has an article or info on the efficacy of full axillary node removal vs radiation of nodes after a positive frozen section of the Sentinal node in surgery, but specifically for those with tumors over 5cm treated with neoadjuvent chemo. I can’t find info on this subset, most articles talk about small tumors and/or don’t mention neoadjuvent chemo.
Thanks in advance
-
Dear xfitmama2, can you highlight your diagnosis/histologies/history as decisions are made depending on them? Standard of care could be easily found in ESMO guidelines but I believe you are familiar with them. The discussion in this sphere (LN removal, Sentinel removal, radiation vs removal, mastectomy/lumpectomy&nod removal) is still going on, you can find come comparison studies but I'd be surprised if you found such a comparison for that exact subset.
Saulius
-
Researchers reveal a possible biological mechanism connecting breast cancer and type 2 diabetes
https://www.news-medical.net/news/20220530/Researc...
-
Ultrasound-guided microbubbles boost immunotherapy efficacy
...In the preclinical study, the MUSIC strategy demonstrated a complete tumor eradication rate of 60% when administered as monotherapy in breast cancer models...
https://www.sciencedaily.com/releases/2022/05/2205...
-
Cancer-killing virus injected into human for the first time in new clinical trial
Previous studies have shown that CF33-hNIS is effective against cell culture and animal models of breast, colorectal, pancreatic, ovarian, and lung cancers. During the Phase 1 clinical trial, researchers will test the safety and tolerability of CF33-hNIS in cancer patients by injecting the virus directly into the blood or the tumor.
-
'Masked' Cancer Drug Kills Tumors While Sparing Healthy Tissue, Early Results Show
In breast cancer models, our masked IL-12 resulted in a 90 percent cure rate, while treatment with a commonly used immunotherapy called a checkpoint inhibitor resulted in only a 10 percent cure rate.
https://www.sciencealert.com/masked-cancer-drug-ki...
-
New Biomarker Classifications May Improve Treatment for High-Risk Breast Cancer Patients
The researchers, whose findings were recently published online in Cancer Cell, show that by combining predictive biomarkers to create response predicting breast cancer subtypes, these subtypes can then be matched to the most effective modern treatments. The best subtyping schemas incorporate Immune, DNA repair, Luminal, and HER2 phenotypes, Treatment assignment using these response predictive subtypes may improve the efficacy of the treatment and patient outcomes.
https://www.ucsf.edu/news/2022/06/423061/new-bioma...
-
ASCO: AstraZeneca, Daiichi's Enhertu could transform breast cancer treatment with landmark HER2-low show
At a median follow-up of 18.4 months, Enhertu extended the median time patients had lived without disease worsening to 9.9 months, versus 5.1 months for patients who got physician's choice of chemotherapy. The drug prolonged patients' lives to a median of 23.4 months, compared with 16.8 months for chemo, according to data presented at a plenary session of the 2022 American Society of Clinical Oncology annual meeting.
https://www.fiercepharma.com/pharma/asco-astrazene...
-
Thanks, Debbrew- interesting articles
-
Updated Guidelines on Biomarkers for Early-Stage Breast Cancer
According to the April 25 press release from Hologic (the parent medical technology company that developed BCI), ASCO "now recognizes BCI as the only genomic test to help guide extended endocrine therapy decisions in early-stage, HR+ (hormone receptor-positive) breast cancer patients with node-negative or node-positive (one-three positive nodes) disease when treated with five years of primary endocrine therapy without evidence of recurrence."
BCI is a microarray-based test that analyzes the expression of 11 genes associated with breast cancer recurrence.
-
Dear all, has anyone had any news from Lumpie? She's the "founder" of this thread and used to post constantly but does not anymore after the site was renewed:/ Hmm...
Saulius
-
It is so depressing the number of good friends who have given up and no longer post. It was bad enough losing friends to cancer - but many members just will no longer deal with the inane revisions & issues & problems on BCO. I too hope Lumpie is OK - along with a ton of other people who have (understandably) disappeared.
-
Hi all! Lumpie here. Thank you so much for your concern. Sorry I have not been present as much as in the past. You know how life just catches up with you some times and is demanding? That's kind of where I am. The side effects of my current treatment are chronic and annoying which slows me down. I have had some personal business and family matters that have consumed a great deal of my available time and energy lately. Some fun stuff, too: I saw a couple of college friends last week that I had not seen in a very long time. And then there is the less fun stuff (semi-flooded basement). You know.... life is messy and it comes at you non-stop. So it has taken away from my time to read and research. Maybe I have missed it due to inattention, but I have not seen the volume of new research with eye-catching results coming out lately. (Sidebar: I confess that, while I think that the new BC.com format is "prettier," I find it more challenging for posting to-be-read research-type material. A minor issue, but a thought.) I hope that in a few more months I will still be doing well and will be on a more even keel. Maybe more promising research will be published then, too. I do watch the discussion and if I see anything really good, I will try to pop over and post. The mutual support and concern in this forum - and others - is so wonderful. It's keeps me believing in humanity. More asap... take care and be well!
-
Lumpie, so glad that all is [essentially ] well!
-
Lumpie- so glad to see you as well.
-
Lumpie - thanks for posting. HOpe all life's hassles settle down soon.
-
Thanks for checking in, Lumpie! Hope you are in a good place to start posting again soon!
-
Dear Lumpie, this is what we wanted to hear - that you are alright:) And living life... is a wonderful thing, glad that you are doing it
Saulius
-
Promising compound kills range of hard-to-treat cancers by targeting a previously undiscovered vulnerability
The researchers soon noticed that a compound called ERX-41 not only killed ER-positive cancers in petri dishes, but also readily killed TNBCs, including more than 20 distinct TNBC cell lines. Further experiments showed that ERX-41 also effectively shrunk human cancers and several of these cancer cell lines when grown as tumors in mice without affecting normal cells or causing any discernible toxicity in these animals.\
-
Lumpie 👏🏻👏🏻
-
Symptom trackers may improve QOL in metastatic cancer
People with metastatic cancer who reported symptoms, lifestyle habits and daily challenges electronically every week had greater improvement in physical function, symptom control and health-related quality of life than those receiving usual care, researchers reported in the Journal of the American Medical Association. Care teams were alerted when patients reported severe or worsening symptoms, potentially enabling interventions that prevented complications, but the researchers also noted that alerts could be difficult for care team members to address in the absence of dedicated time.
Reported here: https://www.mobihealthnews.com/news/study-electron...
Study here: doi:10.1001/jama.2022.9265
Relevant clinical trial: NCT03249090
{Of course, they will charge for access to the full study. Reporting and abstract are free. I have been encouraging my computer science guru nephew to develop a symptom tracking app that is not evil (=sells your private info). We'll see.}
-
Trastuzumab Deruxtecan in Patients With CNS Involvement From HER2+ Breast Cancer
- This primary analysis of the phase II DEBBRAH trial evaluated the efficacy and safety of trastuzumab deruxtecan (T-DXd) in patients with HER2-positive breast cancer with CNS involvement, including those with active brain metastases and even leptomeningeal disease. An impressive objective response rate was noted with T-DXd in all three cohorts. Toxicity was manageable, with 9.5% of the patients having grade 1 pneumonitis.
- These data suggest that T-DXd is a promising treatment option for patients with HER2-positive metastatic breast cancer with stable, untreated, or progressing brain metastases. Larger trials are warranted to validate the findings. {Cohort was 21 patieints.}
The manuscript has been accepted but not yet published. It is currently available in its entirety without charge. That may change once it goes to press. -
Not really news, but interesting...
Getting closer to a vaccine for cancer
https://www.washingtonpost.com/health/2022/06/14/cancer-vaccine-future/
-
Study Compares DBT With Digital Mammography Screening
Digital breast tomosynthesis linked to lower risk of advanced breast cancer for women with extremely dense breasts, high risk for breast cancer
- HealthDay WEDNESDAY, June 15, 2022 (HealthDay News) -- Compared with digital mammography, digital breast tomosynthesis (DBT) is not associated with a significant difference in the risk of interval invasive cancer or advanced cancer among women who are not at high risk, according to a study published in the June 14 issue of the Journal of the American Medical Association.Karla Kerlikowske, M.D., from the University of California in San Francisco, and colleagues conducted a cohort study involving 504,427 women aged 40 to 79 years who underwent 1,003,900 screening digital mammography and 375,189 screening DBT examinations from 2011 through 2018.The researchers observed no significant difference for interval invasive cancer rates per 1,000 examinations for DBT versus digital mammography, or among all 836,250 examinations with Breast Cancer Surveillance Consortium (BCSC) five-year risk <1.67 percent, or among all the 413,061 examinations with BCSC five-year risk of 1.67 percent or higher across breast density categories. Among women at low-to-average risk or at high risk with almost entirely fatty, scattered fibroglandular densities, or heterogeneously dense breasts, advanced cancer rates were not significantly different for DBT versus digital mammography. For the 3.6 percent of women with extremely dense breasts and at high risk of breast cancer, advanced cancer rates were significantly lower per 1,000 examinations for DBT versus digital mammography, but not for women at low-to-average risk."Screening with DBT versus digital mammography was associated with a significantly lower risk of advanced breast cancer (prognostic pathologic stage II or higher) among women with extremely dense breasts and high risk of breast cancer," the authors write.Several authors disclosed financial ties to industry.Reporting: https://www.practiceupdate.com/C/137546/56?elsca1=...Article: doi:10.1001/jama.2022.7672{Access to reporting and abstract are w/o charge but registration may be required. Subscription or payment may be required for full article access.)
-
Getting closer to a vaccine for cancer
Scientists have worked for years to harness the power of the immune system. New approaches make researchers optimistic about success.
June 14, 2022
...scientists studying cancer vaccines believe they now are closer than ever before. While these vaccines are still a long way from approval, researchers think they represent the future of cancer care.
{a few quotes re breast cancer...}
MUC1, is present in several types of cancers, including colon, breast, prostate, lung and pancreatic. An MUC1-based vaccine she and her team developed showed a strong response from the immune system in clinical trials in patients with premalignant colon polyps, leading them to believe the vaccine could help prevent the growth of new polyps and keep existing ones from turning cancerous.
The vaccine reduced polyp recurrence rates by 38 percent in their clinical trial
"We and other groups are paying attention to premalignant lesions and focusing on trying to boost the immune system to stop the progression from premalignant to malignancy," Finn says, adding that her group is about to begin a trial of the same vaccine in patients with ductal carcinoma in situ — an early stage of cancer that is confined to breast milk ducts and not yet invasive — to see whether the vaccine can stop it from spreading.
Many cancers also share common antigens, meaning a personalized vaccine isn't always necessary. HER2, a molecule found in about 25 percent of breast cancers is one example. Berzofsky's lab is testing therapeutic vaccines for several cancers, including one that targets HER2.
"It's a 'driver' antigen, which means the cancer can't do without it," Berzofsky says. "It keeps telling the cell: divide and multiply, so going after it with a vaccine would be very effective." Early clinical trials have been promising, he says. There is a drug, Herceptin, available to treat HER2-positive breast cancer patients, but "the patient has to come back to get an IV drip every few weeks," Berzofsky says. "If we had a vaccine that caused a patient to make her own HER2 antibodies, she wouldn't need to come back for the drug."
Knutson and Amy Degnim, a breast surgeon at the Mayo Clinic in Minnesota, also designed a HER2 vaccine and recently completed a small clinical trial in 22 patients with invasive breast cancer. The vaccine, based on four fragments of the HER2 protein, provoked both antibodies and T cells in all the patients, Degnim says. The vaccine was given in six doses, each one a month apart.
After a little more than two years, only two patients had recurrences: one developed another tumor in the same breast, the second patient experienced a recurrence in the lymph nodes, "but that patient did not complete the full vaccination course," having received only four doses, Degnim says.
They are also developing another vaccine they hope will completely prevent breast cancer in women at high risk for the disease. Initially, however, it will be tested — for safety reasons — only in women who already have breast cancer.
https://www.washingtonpost.com/health/2022/06/14/c...
https://doi.org/10.1073/pnas.2200200119
{The Post generally puts stuff behind a pay wall. PM me if you have questions. The journal will let you see the abstract, but there is a pay wall for full access.}
-
Drug combination could be less invasive treatment for [mbc], study finds
Researchers from the National University Cancer Institute, Singapore (NCIS) at the National University Hospital and the Cancer Science Institute of Singapore (CSI Singapore) at the National University of Singapore found that combining two drugs - letrozole and lenvatinib [pill form] - might help those with advanced stage metastatic breast cancer achieve better control of the disease.
The researchers conducted a study of 43 patients with stage four breast cancer who had failed multiple prior therapies.
Half of those given the combined therapy either saw their tumours shrink or experienced good control of the disease for more than six months, with many able to continue normal daily activities.
https://www.straitstimes.com/singapore/health/drug...
-
An article was just published in the May/June edition of Cancer Journal by Dr Bluming entitled 'HRT After Breast Cancer - It is Time.' Happy to email the pdf to anyone or figure out how to share here. Short version is that oncologists should look at current study results about this topic, 24/25 studies indicate no increase in recurrence after using hormone replacement therapy, as well as the often-severe health effects of estrogen suppression. Yes, even for women who had ER+ breast cancer, although the risk may be slightly higher. Vast majority of symptoms we attribute to treatment (chemo brain, ongoing fatigue, severe depression) are often from the temporary or permanent suppression of our hormones, but doctors still don't really understand what causes cancer or the role of estrogen in breast cancer at all. What they do know is that estrogen greatly increases protection from top three killers of women - heart disease, bone fractures, and dementia.
He also cowrote a book called Estrogen Matters where he disputes the connection that was made from a flawed study in 2002 (Women's Health Initiative) indicating it might increase beast cancer risk and leading to very few women wanting or being prescribed HRT after that time, even for severe quality of life issues brought on by perimenopause and menopause. Really well done and interesting.
-
https://www.fiercebiotech.com/medtech/fda-clears-k...
FDA clears Koios Medical's ultrasound-reading AI that spots breast, thyroid cancer in 2 seconds
-
(early research)
'Masked' cancer drug [IL-12] sneaks through body to deliver anti-tumor treatment with fewer side effects
In models of breast cancer studied in the lab, masked IL-12 was even more effective than anti-PD1 antibody, an immune therapy commonly used in humans.
-
FDA finalizes guidance on including patients with incurable cancers in oncology trials
In their guidance, the agency recommended sponsors include patients with incurable cancer—defined as unresectable, locally advanced, or metastatic disease in solid tumors and/or hematologic malignancies with unfavorable long-term overall survival—in oncology clinical trials even if they met criteria that would otherwise exclude them, such as in situations where a patient had previously received an available therapy in a non-curative setting. The recommendation by FDA emphasizes that sponsors still need to follow regulations around informed consent before enrolling patients with incurable cancer in clinical trials.
https://www.raps.org/news-and-articles/news-articl...
-
Interesting, I was told my cancer is "locally advanced" (3B IDC) but was not told that it is considered "incurable" (although what breast cancer is?). I had a large localized tumor with no nodes and no detectable spread anywhere. I knew it was real bad, but I hadn't realized that that apparently puts me in the same category as metastatic and unresectable? You learn something every day.
Thanks for your post, Debbew.
-
Locally advanced, as in lymph nodes, is not regarded as Stage 4 metastatic bc in everything I’ve ever read. This would be a Stage 3B or Stage 3c diagnosis. Lymph nodes are always resectable, too. And can b radiated. Curious.
-
FDA Approves First Targeted Therapy (Enhertu) for HER2-Low Breast Cancer
https://www.fda.gov/news-events/press-announcement...
Threetree, I agree with TravelText.
-
I was just reading this. I'm curious if the are going to start considering Her2 Equivocals as HER2 low?
-
Dear Bluegirl27 - absolutely, HER2 Equivocals are in HER2Low category.
Saulius
-
Circulating Tumor DNA and Late Recurrence
– Personalized assays identified high-risk patients
by Jeff Minerd , Contributing Writer, MedPage Today August 16, 2022
Personalized circulating tumor DNA (ctDNA) assays identified women with HR-positive, HER2-negative breast cancer who had late recurrences, suggesting that these high-risk patients can be identified for potential interventions, researchers said.
"To our knowledge, these are the first data on plasma ctDNA analysis for MRD [minimal residual disease] detection in late adjuvant HR+ breast cancer, a major and understudied cause of more than 40,000 annual breast cancer-related deaths in the United States," Heather Parsons, MD, MPH, of Dana-Farber Cancer Institute in Boston, and colleagues wrote in a "Rapid Communication" article in the Journal of Clinical Oncology.
Parson's group performed whole-exome sequencing on primary tumor samples from 103 patients with high-risk stage II-III HR+ breast cancer who were diagnosed more than 5 years prior and had no clinical evidence of recurrence. The somatic mutations detected were used to design, for each patient, a personalized ctDNA RaDaR [residual disease and recurrence] assay.
Over the next 2 years, the team collected plasma and performed the personalized ctDNA tests at routine visits every 6-12 months. Eight patients (10%) had positive MRD testing. Of these, six (7.2%) developed distant metastatic recurrence. The median ctDNA lead time was 12.4 months. One patient had a local recurrence not identified by the test.
"Here, 10% of patients were MRD-positive more than 5 years from diagnosis despite no clinical evidence of metastatic recurrence at the time of first plasma sample," Parsons and colleagues said. "Importantly, ctDNA analysis identified MRD in all cases of distant recurrence. ctDNA analysis did not identify MRD in the case of local recurrence in this study, consistent with previous reports. Additionally, ctDNA was detected in two patients who had not experienced clinical recurrence at the time of last follow-up, although imaging had not been obtained in these cases."
In addition, "these data suggest that there may be a period in which MRD is detectable via ctDNA before overt, late breast cancer recurrences. This will inform future studies of liquid biopsy to personalize treatment and prevent or delay late recurrence of early-stage breast cancer," the researchers concluded.
In the following interview, Parsons discussed additional details of the study and other relevant ongoing research.
Can you give us more details on how the individualized RaDaR assay is created for each patient?
Parsons: RaDaR is a tumor-informed, patient-specific assay. First, each patient's archival primary tumor sample underwent whole exome sequencing (WES). Then, from mutations identified in the WES, up to 51 variants were selected for assay design.
Next, each patient-specific assay was applied to cell-free DNA isolated from a patient's plasma, to the leukocyte DNA and to the tumor DNA. Samples underwent high-depth sequencing, variants were confirmed, and ChIP [clonal hematopoiesis of indeterminate potential] was filtered. Each test was then reported as either MRD+ or MRD-. For positive MRD tests, eVAF (estimated variant allele fraction) was reported.
Do you plan to continue this study with longer follow-up or additional patients?
Parsons: Yes, we are continuing to follow these patients clinically and to draw research blood samples. We believe this is an important, understudied group of patients – those with a history of HR+ breast cancer diagnosed more than 5 years prior.
Have the two patients who were MRD positive but without recurrence during the study period experienced recurrence subsequently?
Parsons: We have not yet gone back to assess follow-up for the overall cohort but plan to do this in the coming months.
You mentioned that several clinical trials are underway to investigate the efficacy of interventions based on MRD detection. Are there any results yet from these trials, or any information about when can we expect them?
Parsons: In HR+ breast cancer, there are a few trials underway evaluating intervention based on MRD detection. The DARE and LEADER studies are both enrolling patients with history of HR+ breast cancer with an MRD positive test. Patients are screened and then undergo staging scans if the MRD test is positive. If metastatic disease is not detected, they enter the study.
In both trials, investigators are evaluating the efficacy of a CDK4/6 inhibitor together with hormonal therapy.
You mentioned that researchers at the Dana Farber Cancer Institute are investigating patient understanding of and attitudes toward late recurrence in a survey study. Can you tell us more about this study and what it hopes to find?
Parsons: This is the POWER study, led by Shoshana Rosenberg. In investigating patients with HR+ breast cancer with risk of late recurrence, we found very little data available evaluating patient understanding of and attitudes toward this risk. The POWER study, which is complete and undergoing data analysis currently, enrolled participants at least 5 years from diagnosis with HR+ breast cancer.
We look forward to the results of this study to help us design patient-centered interventions and approaches to the problem of late recurrence in HR+ breast cancer.
Read the study here and expert commentary about the clinical implications here.
The study was funded by AstraZeneca, the National Cancer Institute, and Susan G. Komen.
Parsons reported research funding from Puma Biotechnology (Inst).
Primary Source
Journal of Clinical Oncology
Journal: DOI: 10.1200/JCO.22.00908 Journal of Clinical Oncology 40, no. 22 (August 01, 2022) 2408-2419.
Reporting: https://www.medpagetoday.com/reading-room/asco/bre...
{Both full text and reporting are available w/o charge.}
-
Replying to Mar 18, 2022 10:34AM sarahmaude wrote:
Treatment and Survivorship Interventions to Prevent Poor Body Image Outcomes in Breast Cancer Survivors
Have any of you farther along found a good way to advocate for survivorship care? Either for yourself individually, or to help other women have a better experience?
I was cut loose with major treatment damage, high risk of recurrence, and no plan. My oncologist's office shamed me when I pressed for more information or help. They think it is the primary care doctor's problem. He says he does not have the expertise. Current status: no support for dealing with damage, no screening, no care. And I was treated at a major center that advertises itself as patient-centered. I don't think my situation matters much. (If it metastasized it will kill me no matter when I catch it, and the damage done is done.) But I feel like it might help me to advocate for others.
-
lenaaz,
I am not happy with your oncologist's office for shaming you when you pressed for more information and help! Not acceptable! This was a very reasonable request.
A few thoughts: I think that NCCS (National Coalition for Cancer Survivorship) is a non-profit doing the best advocacy around the survivorship issue. Their web page is http://canceradvocacy.org/ and their unique focus is that *every* cancer patient should leave treatment with a written survivorship plan which clearly explains the treatments they have had and on-going monitoring that is the current standard of care. This way, it can be made a part of their chart and it is easy to share with a Primary Care doc who can help you stay on track with monitoring.
Another resource that may be of help to you: https://www.cancer.net/survivorship This is the ASCO (American Society of Clinical Oncology) website targeted to patients and dealing specifically with questions related to survivorship. The resources here may be helpful.
NCCN (National Cancer Care Network) publishes the definitive standards on cancer care. They have versions for both patients and professionals. Needless to say, the professional version is much more technical and detailed. I quickly looked through the materials to see what it might have to say about survivorship care. Disappointingly, it did not say much. I did not dig into the professional version. You may want to go here and take a look https://www.nccn.org/guidelines/guidelines-detail?...
Clearly, a great deal more advocacy is needed around this issue. Sometimes, the farther you get into the breast cancer world, the more you find there is to do to make care better. Some, of course, is medical or scientific, but *we* are the experts on the patient experience and sometimes, we have to be the voice advocating for improved care. If and/or when you feel up to it, consider being a voice for improvement. We - and our loved ones - will all be healthier if we can improve cancer care. Thanks for raising this important issue.
-
Here is another resource on how to put together your own survivorship (they call it "thrivership") package: https://pinklotus.com/powerup/resources/thrivership-care-plan/
-
New TROPiCS-02 Data in HR+/HER2- Metastatic Breast Cancer Patients Demonstrates Progression-Free Survival Benefit of Trodelvy® Regardless of Their HER2 Status
-
WOW indeed! so exciting! thanks for posting!
-
https://www.nbcnews.com/health/womens-health/breas...
FDA receives reports of cancer linked to breast implants
The agency has received 10 reports about squamous cell carcinoma, a type of skin cancer, and 12 reports about various lymphomas related to breast implants.
-
Antipsychotic use associated with elevated risk of breast cancer
-
cp418 - would love to read the article about skin cancer & implants, but there is a firewall. If it's not too long, could you copy & paste? Or oops, maybe BCO won't work with that.. Urgh
-
Could MS drugs help treat 'chemo brain'?
Seems like this research is still very early stage, but at least the drugs they are considering are already approved.
-
Phase 2 Trial to Study Novel Drug in Pretreated Solid Tumors [including TNBC]
...The other will evaluate navicixizumab alone or in combination with paclitaxel for patients with triple-negative breast cancer who received between two and four standard lines of therapy for metastatic disease, including an immune checkpoint inhibitor or Trodelvy (sacituzumab govitecan)....
Navicixizumab simultaneously targets inhibition of DLL4, a ligand of the Notch pathway, and VEGF, making this a very attractive therapeutic strategy to evaluate," Oberstein said.
https://www.curetoday.com/view/phase-2-trial-to-st...
-
minustwo -- Here's the FDA presser announcing the "communication" (regarding Reports of Squamous Cell Carcinoma and Various Lymphomas in Capsule Around Implants):
https://www.fda.gov/news-events/press-announcement...
and the actual FDA "communication":
https://www.fda.gov/medical-devices/safety-communi...
-
Not research news, but some may be interested in this:
Watch "Hidden Scars" with the directors
Join directors and cancer survivors Kathleen "Casey" Clabby and Noel Storm to view their documentary, "Hidden Scars: Emotional Impact of Mastectomy and Cancer-Related Experiences," on Tuesday, September 20, 2022, at 6 p.m. (ET). The film explores the emotional impact of breast surgery both before and after the procedure. There will be time for discussion and an opportunity to learn about resources for support. This program is brought to you in partnership with Jefferson Health Sidney Kimmel Cancer Center, Unite for HER, and Living Beyond Breast Cancer. There are limited spots available, so please register as soon as possible.
Register here:
https://jefferson.zoom.us/meeting/register/tJAsf-i...
{Event appears to be free of charge.}
-
Texas Judge's Ruling Puts Free Preventive Care in Jeopardy
This Wednesday, a federal judge in Texas ruled that parts of the Affordable Care Act (ACA) requiring health insurance companies to cover specific preventive services and drugs at no cost to patients are unconstitutional. Judge Reed O'Connor previously challenged the ACA when he ruled in 2018 that the ACA was unconstitutional; however, the Supreme Court overturned the decision in 2021. In this latest ruling, Judge O'Connor found that ACA provisions relying on recommendations from the Preventive Services Task Force – a panel that decides which preventive care services must be covered under the law – were unconstitutional, as the task force's members are not appointed by the president or confirmed by the Senate. He also targeted the ACA's requirement that health plans cover HIV pre-exposure prophylaxis, known as PrEP, at no cost, ruling that it violates religious freedom law.
One of the plaintiffs, Steven Hotze, who has actively campaigned against the ACA and has referred to same-sex marriage as a "wicked, evil movement," claimed that providing coverage for PrEP burdened his religious freedom as he believed it facilitated and encouraged, "homosexual behavior, intravenous drug use, and sex outside of marriage." The plaintiffs also made a case against covering contraception, the HPV vaccine, and screenings and behavioral counseling for sexually transmitted diseases and drug use.
Why it matters: Under the ACA, health plans must cover a number of preventive services, including cancer screenings and vaccines, at no cost to patients. The mandate has increased the use of preventive services and improved health outcomes through earlier detection and treatment. Despite O'Connor's ruling, requirements that insurers cover certain kids' services, reproductive services, and vaccines stand for now, but free preventive services under the ACA are still at risk. The Department of Health and Human Services (HHS) has not yet said if it would appeal this decision, although it is believed that an appeal is forthcoming.https://www.nytimes.com/2022/09/07/us/politics/aca...
{Write-up courtesy of NCCS. NYT generally allows access to a limited number of articles without charge each month. Further access may require a subscription or access via your library. Depending on local offerings, such access may be available on-line, remotely for library card holders. If you run into barriers, PM me.}
-
Estimation of the numbers of individuals living with metastatic cancer in the United States
According to researchers at the National Cancer Institute (NCI), as of 2018, more than 620,000 people in the US were living with metastatic breast, colorectal, prostate, lung, or bladder cancer or metastatic melanoma. Further, researchers expect that number to increase to nearly 700,000 by 2025.
What they're saying: "Cancer survivorship often focuses on those who have completed treatment," said Emily Tonorezos, MD, MPH, director of NCI's Office of Cancer Survivorship. "But with over 620,000 metastatic cancer survivors in this country alone, these findings highlight the growing importance of identifying and addressing the needs of these survivors, who remain on treatment or who go on and off treatment."https://doi.org/10.1093/jnci/djac158
{Write-up courtesy of NCCS. Free access to journal article.}
-
People with terminal cancer need to know they are dying. Doctors shouldn't withhold that information
Dr. S. Monica Soni, MD, an internist and Associate Chief Medical Officer at New Century Health, reflects on the failings of the health care system in appropriately communicating to cancer patients their diagnosis and prognosis and involving them in decision-making regarding their care. In a study of individuals age 70 and older being treated for incurable cancer, 41% believed they had more than five years to live, while just 10% of their oncologists agreed. Nearly 60% believed their terminal cancer could go away and never return.
What she's saying: "Physicians should be responsible for overcoming health literacy barriers, time constraints, and mistrust to ensure that their patients understand all available options. Anything outside of that is not informed consent. Before patients agree to chemotherapy riddled with unpleasant or harmful side effects, they should have a complete picture of what it will gain them in terms of months of life, quality of life, and symptom burden. For themselves, physicians are overwhelmingly likely to choose non-aggressive care at the end of their lives and up to one-third of oncologists wouldn't accept the chemotherapy they prescribe. This suggests a lot goes unsaid when physicians break bad news to patients about terminal cancer and other fatal diseases and offer next steps."https://jamanetwork.com/journals/jamanetworkopen/f...
doi:10.1001/jamanetworkopen.2022.0018
{Write-up courtesy of NCCS and STAT News. Access to full journal article is without charge but may require registration at the site.}
-
Paid sick leave associated with lower mortality rates among US workers
The US is one of the only developed countries in the world that does not have a national paid sick leave policy. Yet, new research shows the benefits these policies can have for Americans. The study revealed that areas where employers were required to provide paid sick leave had lower mortality rates among working age adults. Mandatory paid sick leave policies are associated with lower rates of suicide and homicide among men and lower homicide and alcohol-related mortality among women. Yet, the recent rise of preemption laws restricting lower governments' ability to enact mandatory paid sick leave policies poses a serious risk. From 2010 to 2017, preemption laws likely contributed to a 6% increase in mortality among working adults.
The bottom line: "Lack of [paid sick leave] increases the odds of economic hardship and involuntary job loss for those who take time off to recover, which in turn can elevate the odds of suicide, drug use, and other risky behaviors. [Paid sick leave] can also produce positive spillover impacts on healthy workers by reducing exposure to sick colleagues," the study's authors wrote.https://www.ajpmonline.org/article/S0749-3797(22)00330-0/fulltext?utm_source=NCCS+Constituent+Database&utm_campaign=d18fc425d3-HCR_MC_Sept_9_22&utm_medium=email&utm_term=0_e96359f924-d18fc425d3-54826649&mc_cid=d18fc425d3&mc_eid=12d673e585
DOI:https://doi.org/10.1016/j.amepre.2022.06.005
{Write-up courtesy of NCCS and The Hill. Access to full journal article is free.}
-
Are No Eyebrows the New Eyebrows?
After a decade ruled by big brows, some celebrities and trend setters are shaving and bleaching their caterpillars. The effect is both avant-garde and alien-like: 'I look like an egg.'
The effects of chemo are now a fashion trend. Who knew? You heard it here first.
https://www.wsj.com/articles/doja-cat-eyebrows-kim...
{Subscription required to access full article. But you don't really need that, do you? }
-
lumpie - Love it! I texted several of my friends to show them what a trendsetter I am!
-
nopink2019: So glad you appreciated that. Not exactly academic, but I hoped people would get a chuckle out of it. (Why would you do that on purpose? No eyebrows, no eyelashes. I look like a fish! Ah, well.... )
-
debbe - thanks for the open link about implants and squamous cell cancer.
Lumpie - GREAT batch of articles. Thanks.
-
Lumpie - Thank you for the info and the articles. As soon as Kylie Jenner did the no eyebrows look for the Met Gala I decided I was not going to worry as much about drawing on my eyebrows. LOL. Who knew we were all ahead of the trend?!
-
Coping With a Deadly Prognosis
It's not a research article and it's not even breast cancer, but this podcast (with a transcript option) may be of interest to those coping with a metastatic diagnosis.
"The Doctor's Art" is a weekly podcast that explores what makes medicine meaningful, featuring profiles and stories from clinicians, patients, educators, leaders, and others working in healthcare.
Hosts are Henry Bair and Tyler Johnson, MD. Guest is Katie Coleman who was diagnosed with metastatic oncocytoma, a rare type of kidney cancer when she was 29 years old. She talks about living with prognostic and therapeutic uncertainty.
It is a rather long (@ 48 minutes) but IMO interesting and insightful interview about the uncertainty of living with a metastatic diagnosis, especially for those diagnosed at a young-ish age - but many aspects of the uncertainty apply to anyone living with a metastatic diagnosis.
Listen at this link or Listen and subscribe on Apple, Spotify, Amazon, Google, Stitcher, and Podchaser.
https://www.medpagetoday.com/podcasts/thedoctorsar...
{No charge to access or listen but medpage and podcast sites may require registration.}
-
Yes, I read this article on medpage and thought it was very interesting, I certainly spent way too much time worrying about prognosis and had to work hard at planning trips etc (I was worried I would screw up someone else's trip if I couldn't make it!) anyone can have an acute event that screws up plans, but, I don't think they worry about it as much.
I really try mention to people to just surge ahead with their plans when they feel well (get travel insurance) but, I am grateful I didn't have to deal with this at her age and got to have children and a career before diagnosis.
also an interesting commentary about how young people who worry about cancer (with symptoms and good reason) get dismissed due to their age alone.
-
A patient with estrogen receptor positive, HER2-negative metastatic breast cancer enrolled in the phase 2 ELAINE 1 trial demonstrated a durable complete response when treated with lasofoxifene.
https://www.targetedonc.com/view/lasofoxifene-elic...
-
Interesting, but looks extremely preliminary. Just one patient. I'd never heard of the ESR1 mutation and have no idea what it's significance is. Looks like this response occurred after 16 weeks? No mention of how many horrible side effects the person might have had to endure for those 16 weeks. No idea if the results would be lasting.
I think it is great that people are posting these research results though, as it can give us all some hope and more to explore. On the other hand, I remember how a drug called ERSO? was all over the news (about the time the Covid vaccines came out) and it was presented as something that showed real promise for ER/PR+, although lengthy clinical trial were yet to happen. Turned out the whole thing went bust and the company (Bayer?) abandoned the whole project. Not sure why. Someone on these boards had commented that they thought Bayer put out all this press about this drug because they'd missed the boat with the Covid vaccines. This is all sketchy from memory and I don't know the particulars of all of this, but it does show how on the one hand we can all get hopeful from these early published results, but also how we can all get tortured and jerked around by them.
I don't know what the answer is and I am in no way trying to discourage publishing (and posting here) early research results, but some of these studies are just so small and preliminary, and then never go anywhere. I'm surprised at all the research results I read that show some initial promise and then never get taken any further. Is it all about the money?
-
Only one patient in the Elaine phase 2 study had the CR. In general, there seemed to be some benefit to lasofoxifene, but it didn't knock it out of the park. They discuss adverse side effects in the 2nd to last paragraph.
ErSO has not yet been tested in humans. The announcement of the drug does seem over-hyped (animal studies can be promising but often don't pan out), but it was based in part on the novel approach. Bayer dropped their rights to the license, putting it back in the hands of Systems Oncology (the SO in ErSO) and the University of Illinois. They have been continuing to develop it, presumably trying to address concerns about toxicity, and they subsequently published a paper on ErSO-DFP which is supposedly less toxic, but apparently work remains to be done before it is ready for FDA approval for human studies.
-
Debbew - You are a wealth of knowledge about all of these studies - good for you. You are a real plus for all of us to have here.
I have to say that I did only "skim" the article you posted, so didn't see the info about side effects. I just so often see news headlines about supposed big breakthroughs, and yet that "breakthrough" only turns out to give people another 2 or 3 months with all sorts of terrible side effects to go with it. I really wish they would present some of these results more "realistically" without the grand headlines. Getting people 2-3 more months, or getting even one CR as in this Elaine study isn't "nothing", and it's worth hearing about and looking at a bit further, but some of these developments are promoted in the headlines like huge things; almost "miracles" and they are far from it.
I'm really glad that you are "on it" about these studies and sharing what you know with all of us. It is really helpful to have someone who understands them fairly well to be giving us some good info. Thanks!
-
Yes, thanks Debbie.
And always thanks to Lumpie, who continues to make this thread such a valuable place to go.

















































 https://youtu.be/hL8VvfVkv18
https://youtu.be/hL8VvfVkv18











 https://www.youtube.com/watch?v=Q-uGRpXmGGM&feature=player_embedded&fbclid=IwAR1xjgMfkH2uCah4p8C6vRZC5VLoyVxtsoEAvJpfv_zh7ncKBXbz9M8oK4I
https://www.youtube.com/watch?v=Q-uGRpXmGGM&feature=player_embedded&fbclid=IwAR1xjgMfkH2uCah4p8C6vRZC5VLoyVxtsoEAvJpfv_zh7ncKBXbz9M8oK4I












































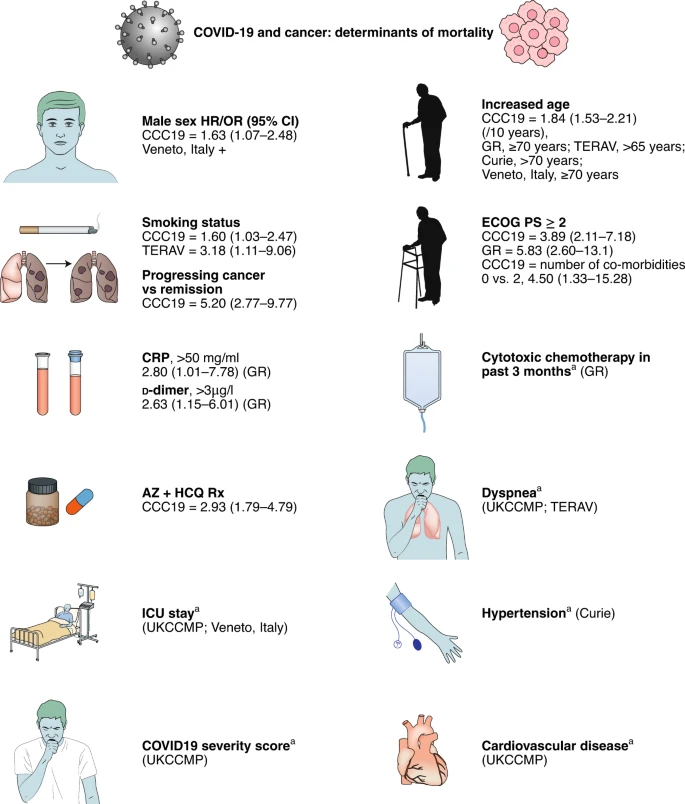
































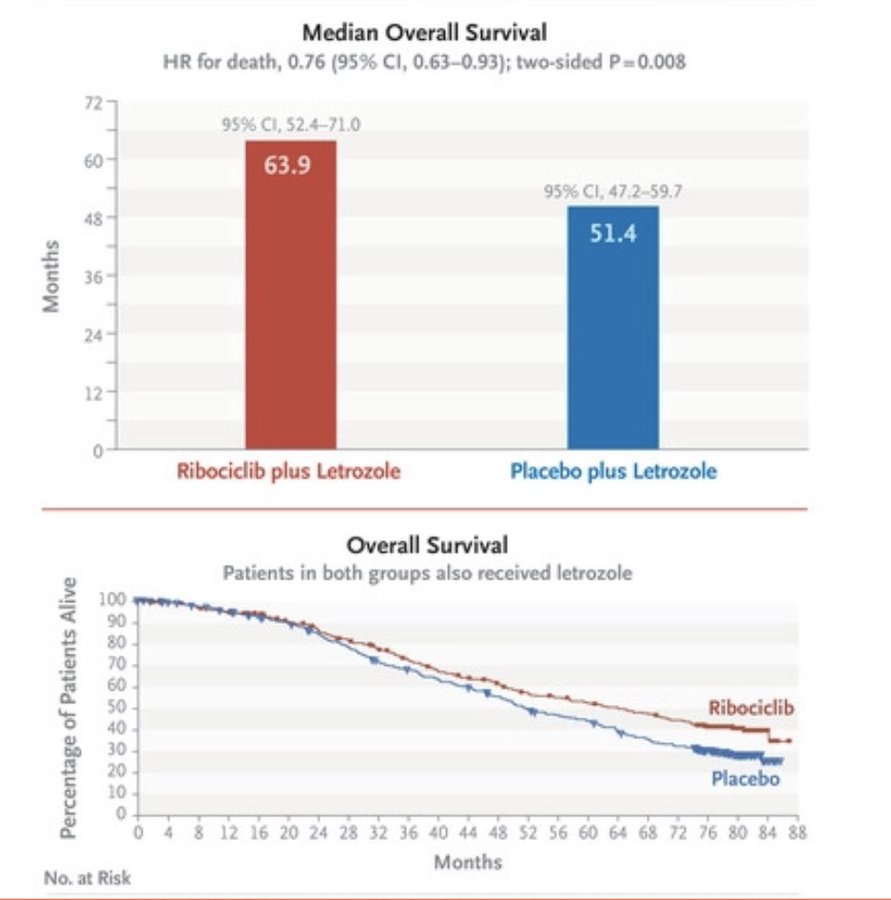


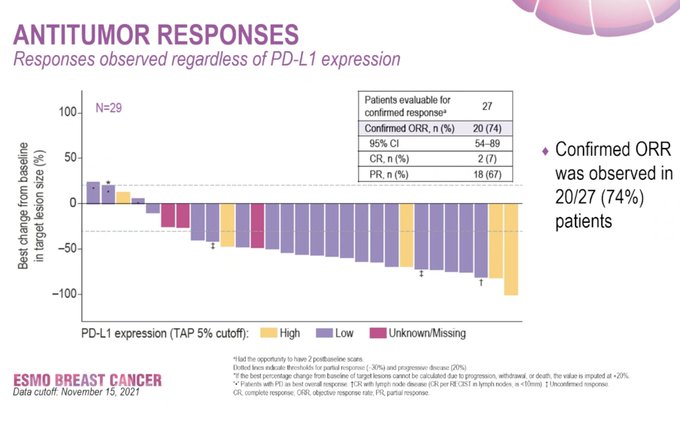







Categories
- All Categories
- 679 Advocacy and Fund-Raising
- 289 Advocacy
- 68 I've Donated to Breastcancer.org in honor of....
- Test
- 322 Walks, Runs and Fundraising Events for Breastcancer.org
- 5.6K Community Connections
- 282 Middle Age 40-60(ish) Years Old With Breast Cancer
- 53 Australians and New Zealanders Affected by Breast Cancer
- 208 Black Women or Men With Breast Cancer
- 684 Canadians Affected by Breast Cancer
- 1.5K Caring for Someone with Breast cancer
- 455 Caring for Someone with Stage IV or Mets
- 260 High Risk of Recurrence or Second Breast Cancer
- 22 International, Non-English Speakers With Breast Cancer
- 16 Latinas/Hispanics With Breast Cancer
- 189 LGBTQA+ With Breast Cancer
- 152 May Their Memory Live On
- 85 Member Matchup & Virtual Support Meetups
- 375 Members by Location
- 291 Older Than 60 Years Old With Breast Cancer
- 177 Singles With Breast Cancer
- 869 Young With Breast Cancer
- 50.4K Connecting With Others Who Have a Similar Diagnosis
- 204 Breast Cancer with Another Diagnosis or Comorbidity
- 4K DCIS (Ductal Carcinoma In Situ)
- 79 DCIS plus HER2-positive Microinvasion
- 529 Genetic Testing
- 2.2K HER2+ (Positive) Breast Cancer
- 1.5K IBC (Inflammatory Breast Cancer)
- 3.4K IDC (Invasive Ductal Carcinoma)
- 1.5K ILC (Invasive Lobular Carcinoma)
- 999 Just Diagnosed With a Recurrence or Metastasis
- 652 LCIS (Lobular Carcinoma In Situ)
- 193 Less Common Types of Breast Cancer
- 252 Male Breast Cancer
- 86 Mixed Type Breast Cancer
- 3.1K Not Diagnosed With a Recurrence or Metastases but Concerned
- 189 Palliative Therapy/Hospice Care
- 488 Second or Third Breast Cancer
- 1.2K Stage I Breast Cancer
- 313 Stage II Breast Cancer
- 3.8K Stage III Breast Cancer
- 2.5K Triple-Negative Breast Cancer
- 13.1K Day-to-Day Matters
- 132 All things COVID-19 or coronavirus
- 87 BCO Free-Cycle: Give or Trade Items Related to Breast Cancer
- 5.9K Clinical Trials, Research News, Podcasts, and Study Results
- 86 Coping with Holidays, Special Days and Anniversaries
- 828 Employment, Insurance, and Other Financial Issues
- 101 Family and Family Planning Matters
- Family Issues for Those Who Have Breast Cancer
- 26 Furry friends
- 1.8K Humor and Games
- 1.6K Mental Health: Because Cancer Doesn't Just Affect Your Breasts
- 706 Recipe Swap for Healthy Living
- 704 Recommend Your Resources
- 171 Sex & Relationship Matters
- 9 The Political Corner
- 874 Working on Your Fitness
- 4.5K Moving On & Finding Inspiration After Breast Cancer
- 394 Bonded by Breast Cancer
- 3.1K Life After Breast Cancer
- 806 Prayers and Spiritual Support
- 285 Who or What Inspires You?
- 28.7K Not Diagnosed But Concerned
- 1K Benign Breast Conditions
- 2.3K High Risk for Breast Cancer
- 18K Not Diagnosed But Worried
- 7.4K Waiting for Test Results
- 603 Site News and Announcements
- 560 Comments, Suggestions, Feature Requests
- 39 Mod Announcements, Breastcancer.org News, Blog Entries, Podcasts
- 4 Survey, Interview and Participant Requests: Need your Help!
- 61.9K Tests, Treatments & Side Effects
- 586 Alternative Medicine
- 255 Bone Health and Bone Loss
- 11.4K Breast Reconstruction
- 7.9K Chemotherapy - Before, During, and After
- 2.7K Complementary and Holistic Medicine and Treatment
- 775 Diagnosed and Waiting for Test Results
- 7.8K Hormonal Therapy - Before, During, and After
- 50 Immunotherapy - Before, During, and After
- 7.4K Just Diagnosed
- 1.4K Living Without Reconstruction After a Mastectomy
- 5.2K Lymphedema
- 3.6K Managing Side Effects of Breast Cancer and Its Treatment
- 591 Pain
- 3.9K Radiation Therapy - Before, During, and After
- 8.4K Surgery - Before, During, and After
- 109 Welcome to Breastcancer.org
- 98 Acknowledging and honoring our Community
- 11 Info & Resources for New Patients & Members From the Team