Refusing Axillary Dissection: what is proper legal paperwork?
Comments
-
I don't really understand why they need the nodes? If they are planning to 'throw the kitchen sink' at you anyway, why not leave the nodes alone?
-
there's been quite a lot of discussion about this of late.
here's a repost that you might find useful...
my surgeon had said that i would have full alnd if the snb came back positive... but another friend of mine is wondering about these questions because she is a musician and very nervous about range of motion / lymphedema issues.....
Here's one paper that is relevant:
jco.ascopubs.org/content/29/34...
In conclusion, on the basis of the results of Z0011, a significant proportion of patients with one to two positive SLNs and BCS can safely forego ALND. The majority of these patients do not need to be subjected to the short-term and long-term morbidity of ALND. The multidisciplinary approach of adjuvant systemic therapy and WBRT is important in reducing the risk of locoregional recurrences. Until additional data are available, including analysis of the Z0011 radiation fields, it remains our policy to assess the risk of microscopic involvement in the regional nodes and to target nodes that are at significant risk in the radiation treatment plan. Table 1 summarizes a suggested approach for radiation field design. Using this approach, we will provide patients with excellent locoregional control and, in combination with surgery and adjuvant systemic therapy, optimize the patient's probability of cure. The data from Z0011 also give additional justification for the use of BCS for patients with positive SLNs. The potential for avoiding ALND, coupled with the high rates of locoregional control that are associated with BCS and WBRT, should make this approach more appealing than mastectomy for most patients.
Later in that same paper:
The radiation oncologist, however, has historically relied on ALND findings in the design of the radiation treatment fields7; the number of positive nodes provides information concerning the risk of involvement of the level III/supraclavicular (SCV) nodes. When this risk is clinically relevant, radiation oncologists commonly treat the level III/SCV region with an SCV field.8 Typically this is used for patients with four or more positive nodes and selected patients with one to three positive nodes. With computed tomography–based planning, this involves contouring level I through III nodes, which ensures adequate radiation to the target nodes that are at risk. Although the combination of ALND and axillary radiation increases the risk of lymphedema,8,9 minimal morbidity is associated with radiation to the undissected level III/SCV region or to the undissected axilla.3,7
anyway, from this paper, it appears that the radiation treatment of the auxiliary nodes does not result in as high a risk of lymphadema, like radiation plus ALND does....and perhaps radiation can do the job....definitely food for thought.
i feel so lucky that i did not have to face alnd... if i had to make a decision about it, and radiation could do the job, i would choose radiation over alnd, but only if radiation could indeed do the job.
best wishes... i'm so sorry you two are dealing with this awful disease.
-
I think the forest is being lost for the trees here.
****Find out for 100 percent dead sure if your wife is stage IV first.****
LE concerns are a distant second. Don't let your emotions and views of the medical profession get in the way of being methodical about this.
Besides, as has been pointed out, LE can be caused by cancer itself. Some people also get it due to chemo and rads. Honestly, LE is the least of your inquiries. Don't go by stories others tell you - that is not a scientifically reliable way to appraise your wife's medical situation. It is also not sensible to pre-judge an individual's intentions based on his or her profession (view of doctors).
Again: see the forest, not the trees. You are concerned about the possibility of one illness (LE) without getting a full confirmation on the existence of a far more serious one (metastatic BC). Your decision on how far to let the surgeon go would likely be different depending on her stage.
I can't believe I am being so strong, but I beg of you and your wife to organize your thoughts and feelings on this better! Either you believe in medical treatment or you don't. But you are in a no man's land where you are believing and disbelieving selectively. Find out the FACTS only. Discard the opinions, emotions or surmises.
-
If you don't trust your surgeon, then find someone else...ask for references of other patients from your surgeon if need be. A good Doctor will keep their word regardless of what is or is not on a piece of paper. You have to have some comfort level that they will make the best choices available at the time. If there is visible cancer, it needs to be removed. Good Luck. And, 1Athena1 is right. Find out abt cancer first. It's much more serious. God Bless
-
I agree that treating the bc should trump concerns over lymphedema. Please read back on all of the op's posting regarding limited choices on doctors due to insurance. This really puts some people between a rock and a hard place. If insurance limits you and you can't afford to pay out of pocket, it can be rough.
-
Yes, I see that. But with or without insurance, their goals and energy have to be properly focused. There is a lot of strangeness about this situation. He said they had insurance but it wasn't accepted in some places. If it is accepted anywhere (which it is) then there must be a way by which his wife can get an exact status of cancer diagnosis. If it really is thought that his wife might have stage IV, then new avenues of assistance may well open up for them (including expedited SSDI and Medicare, importantly).
I almost wish this were in a different forum - like the "not diagned...but concerned", or even lymphedema (so that the sisters there can also tell them not to confuse the forest for the trees). Might get more responses of knowledgeable people (ie: not me) on both topics.
It doesn't really belong here and I am concerned that time is going by and these folks are going round in circles. Whatever they do decide to do is their own business - but they have to see the clear medical picture first and distinguish it from their feelings or surmises.
-
I somehow get the feeling that their minds were set on doing it their way, which is their business. Don't know if they are still reading this forum. Insurance can be very limiting. I belong to a large, all inclusive HMO, which I am very happy with. However, if I were not , all opinions or tx outside my HMO would be at my own expense. I have gone outside for second opinions but was only able to do so with financial assistance from a family member.
-
You may be right in that they are no longer reading. Insurance limitations place even more burdens on the patient to be judicious about what to focus on. No insurance status in the world would cause me to be concerned about the possibility of one illness while not knowling for certain about the existence of another, far more serious one.
(If they are still reading): she could try catholic charities and see if they will help re: tests to confirm staging. The American Cancer Society and others help people with insurance with copays and other things.
For more information on paying for care, this web site is as good as any other:
http://www.breastcancer.org/tips/paying/
Hope they do see that.
There is also an "insurance and financial issues" forum here.
-
I will say that if your insurance limits you, but you have insurance, it is not likely that you will receive financial assistance. I looked into it, just in case I wasn't happy with my HMO, and it was no dice. I am extremely pleased with my care and within my HMO's system I can get as many opinions as I want. I am also grateful to family who financed my second opinion outside my HMO. Boy, are we getting off topic
")
-
2 hours ago J9W wrote:
"I don't really understand why they need the nodes? If they are planning to 'throw the kitchen sink' at you anyway, why not leave the nodes alone?"
J9W it is a matter of degree of known involvement. As the recent medical literature indicates (See BikerLee's post above) patients with 1-2 nodes involved do not neccessarily benefit from ALND. With my first dx in 2000 I had micromets to 2 sentinel nodes and refused ALND since I was going to have chemo anyway. My new primary in 2005 was a different situation with very locally advanced disease and total nodal involvement. Each one of those 23 nodes removed were malignant tumor sites. I did not worry about LE at that point since my first goal was to reduce as much cancer load from my body as possible and hope to survive the disease itself. While radiation and chemo can be very effective, surgically removing known tumor sites also increases the odds of a successful outcome. The combination of multiple treatment modalities gives the best results when you are dealing with a heavy cancer load.
As I have stated before, Lymphedema is certainly manageable and in no way do I regret making the decisions I did to treat my cancer aggressively. I too hope that the OP and his wife can make fighting the cancer their first priority.
-
Until her stage is known for sure, things like "it will make a difference if you do this or that" can not be said with any amount of accuracy.
-
She may not be properly staged now since that area near trachea can not be biopsied or operated on. Only biopsy can confirm or deny cancer, according to standard approach. Drs are assuming that it's stage IV because of size of tumors, multiple lymph nodes involvements, trachea thing lit up on PET scan, that it's not in situ, and that it's recurring...
She has HealthPlus which is part of Medicaid. It's much worse than Medicaid itself. We're in NYC. Neither MSK nor NYU not any major cancer centers takes it. Literally 2-3 centers do. All surgeons within one center will agree with one another... In spite of that, we saw 2 other surgeons for opinions, I paid cash for 1 of those visits, and the other one was covered. I mentioned about what they said earlier... That's correct about no financial support - the idea is "lucky you have insurance, many people don't". My mother receives SSI, barely making it, but even she shared her slender savings.No, we do not fully trust medical profession. Because within medical profession there are opposite polarities as far as cancer treatment approaches and choices and responsibility lies on us, as much as we hate it. Plus, medical profession cannot be proud of high cure rates of cancer, of you know what I'm talking about...
We appreciate support here. Yeah.... this is such messy and confusing with lymph nodes... Arguments on both sides are strong. I think we'll probably flip a coin. Seems like a loose-loose situation anyway. Maybe we should flow with the flow... Should we see if our surgeon will follow his promise and not cut all nodes and then see if that was right decision after all? I guess so...
-
SccS,
Glad to see that you're still here. I feel your conflict about treatment choices and frustration with limitations of insurance. Ultimately, you will do what's right for your wife. I think what many are trying to say is put the tx of the cancer before the fear of lymphedema. I know the chances go up with more nodes taken but having any nodes taken will put your wife in a situation where she will always need to be on guard. Just put the cancer tx first and deal with the rest later.
Caryn
PS:I was born and raised in the Bronx and graduated from Queens College -
Note please, that the paper BikerLee posted and the other new information only applies to positive nodes found through SLN testing and not to positive nodes (usually larger) clinically evident beforehand. Big difference.
-
I had 14 nodes removed and have MILD lymphedema since a mastectomy November, 2011. It flares up and goes away. In the scope of the whole cancer picture, it is really the least of my worries. Other than wrapping it when I fly and trying to remember not to be so crazy in the garden or at least put my lymphedema sleeve on then, I have just gotten used to it. My flare ups have been a 1 inch increase - not even noticeable.
I see a Lymphedema Physical Therapist who has helped me tremendously. She has taught me many "tricks" to keep the lymphatic system flowing. My personal opinion knowing what I know now after having Mastectomy, Chemo and Radiation - I will say it again - Lymphedema is the least of my worries because it is controllable.
I am sorry your experience with doctors has been so negative. I travel quite a distance to get a medical team I trust at the Univ of Michigan. They have been amazing to me.
-
Why not do chemo first? It's called neoadjuvant chemotherapy, and is quite common.
If you do that, you and your wife will see how her tumor responded to chemo. If the chemo works on her specific pathology, then great - a SNB may be all you need to confirm that. There may not even be any lump left to remove. If it doesn't respond, then the only safe thing is to allow the surgeon to use his best professional judgement in how to proceed.
Let's be real here...lymphedema is inconvenient. Cancer left behind in the lymph nodes can be fatal... is that really a gamble you and your wife are willing to take?
-
Read the op. He states that neo adjuvant chemo is currently being done.
Caryn -
I didn't see that when I skimmed - thanks. THen to me it's a no-brainer - either it worked or it didn't, and if it didn't, how could anyone consider leaving cancerous nodes to spread more?
-
sccs:
I am going to say this plainly and forgive my directness:
CONFIRM YOUR WIFE'S STAGE.
Focus on nothing else. No ifs or buts. Everything else is secondary.
Again CONFIRM YOUR WIFE'S STAGE. Do what you have to do to make that happen.
-
I was Stage IV from the onset also. I did the neo-chemo and got great response. I also had tracheal involvement as well as lung and liver mets. I was insistent from the start there would be no axilla removal. I did have a BMX last Aug but no nodes were taken. I did have extensive talks with both the surgeon and onc and they agreed to my wishes. I had encounters with two people with bad LE in the chemo room and I said I would rather risk the cancer than be disabled from doing my job and the hobbies I love. It had already passed thru there so what was the point? They were not going to take out the lung and liver mets either-so again what was the point of risking it.
They have never lit up on any subsequent PET-and I am contenet with my decision. As a Stage IV I think it is all about quality of life and without being able to do my job and garden and be active---that is NO quality to me. I also did Rads but didn;t allow them to do the axilla there either. Rads was totally an extra step-they tried to get me to say if I didn;t remove them I would allow them to radiate them but I stood my ground.
Always a difficult decision but I don;t look back and regret any step i have taken.
-
A couple of things: Can the area near the trachea really not be biopsied? I have a coworker whose BC is back, metastasized, and she also had a spot light up deep in her chest by the trachea. They biopsied it by cutting a small hole at the base of her neck, and inserting a probe guided by fluoroscopy. She had 2 stitches. It was positive and she also has spinal mets just treated with radiation. They did say it was a little risky, as it could cause bleeding, but she and her onc really wanted to know what she was dealing with. Fortunately, she had no complications.
I went outside network for my care. I was initially referred to a local Catholic-affiliated hospial with an excellent reputation for BC care. My insurance dictated I go to the same system that I feel mistreated my father when he was dying from lung cancer back in 2003. I really did not want to let them touch me. Going out of network doubled both my out-of-pocket deductible and yearly maximum (currently $6,000). I'm not rich, either, but I called the hospital's billing department and explained that I wanted to be treated there, but had an insurance issue and wouldn't be able to pay as I went. They set me up on a monthly payment schedule of $100.01, I think so they can say I'm paying more than $100/month. There is no interest and new bills are added without increasing my monthly payment. I'm very pleased I went this direction. It might be worth looking into.
-
SccS~ The surgical consent form will likely have a line that states the procedure that is being done. Don't sign it until it reads the way you want it to. Good Luck!
-
A question for those with more medical expertise than I have. If it is truly impossible to biopsy a certain area, how are mets then confirmed? Assuming there are mets, many, many stage IV women have neither an mx nor lymph node removal. As a matter of fact, for those dx with mets from the get go, some never have mx/node removal and some do after chemo and confirmation of no progression. I have had a bmx and node removal only to be dx with a bone met 2 months later. Of course, that bone met was probably there all along and had it been found initially, I might not have had any surgery. This is very common for stage IV. Caryn
-
In Canada you are always given a consent form before surgery and on that form you can write whatever you feel is appropriate and THAT is legally binding. Don't know about U.S.
-
Just another comment regarding lymph nodes and lymphedema. The body is literally covered from head to toe by the lymphatic system which includes both the vessels that transport lymph fluid and clusters of nodes which filter that fluid. ANY trauma done to the lymphatic system has the potential to result in lymphedema. Yes, the risk is statistically higher the more invasive the procedure and the more nodes removed or damaged. Here is a map from the Academy of Lymphatic Studies (ACOLS) showing the lymph system just in the breast area:
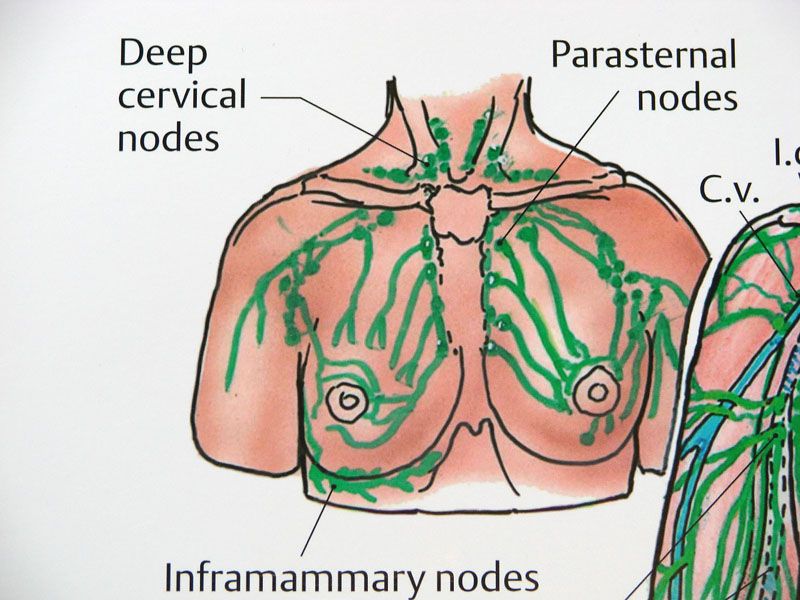
Typically, when we talk about node removal as it relates to breast cancer we are referring to the removal of Sentinel or Axillary nodes. Just be aware that having "only a mastectomy" without axillary node removal still involves the removal of lymph nodes and damage to the lymphatic system, so it is not a free pass from developing future lymphedema. We have women on the LE forums now with active lymphedema and no "axillary node" removal.
This is not intended to scare anyone, but just a statement of fact regarding our human anatomy. Damage is damage, however it may occur to the lymphatic system. Each person's lymphatic system is unique, some being more robust than others. Often people may have an underlying genetic predisposition towards developing lymphedema, unknown to them. We all know cases where women with 20+ nodes removed never have a problem with lymphedema and then there are women with 1-2 nodes or less removed that still develop the condition.
So again, when faced with a cancer dx I believe the priority is to fight the cancer. Lymphedema is a condition that is very manageable when you have a good working knowledge about it and get proper treatment. It is certainly not the case that every patient with lymphedema becomes disabled or unable to enjoy the work and hobbies they love. Check out the Lymphedema forum and see how many women with lymphedema are active athletes or teachers or health care workers or other persons actively engaged in Life. So yes, it is still advisable to discuss ways to reduce cancer related treatment side effects whenever possible. But finding the most effective ways to kill the cancer should still be the primary goal.
-
How exactly do we confirm stage??? With PET scan only, correct?
They said the trachea area can't be biopsied. Another second-opinion-surgeon (who also takes our insurance) said same thing. Maybe it can be biopsied, but they are afraid, or don't have the skills or something... Remember, this is not top notch center....
Chemo had shrunk tumors in about 30-40%, some lumps are not palpable, but lymph nodes lumps are still there, although are smaller.
She will do another PET scan in few days. Looks like PET scan is the only tool of staging her at this point, if I got it right. If the scan shows same or better results than last one, which was done before chemo started, then we'll try to write not more that 50% of level 2 on the consent form and see if surgeon will follow that... I think this is all we can do now. And if the scan shows worse then... I don't know at this point what we'd do....
-
Glad you're touching base. Not being able to biopsy an area is not uncommon. There are more than a few stage IV women who have received their dx based on imaging alone. I was able to have a bone biopsy but others did not. Will be thinking positive thoughts for your wife and you. Caryn
-
Unfortunately, scans and tests are not as accurate as you would like. There are MANY of us here that had significantly more cancer than any of our pre surgery tests indicated. I went into surgery dx by scans as a stage I. Woke up being a stage II. Pathology put me at stage III. Lymphedema, as problematic as it is, is not the main concern here.
-
Pip,
SccS's wife is going to have surgery. His feels like a complete AND is unnecessary because imaging indicates mets to the trachea in an area that cannot be biopsied. Many women who are dx at stage IV have neither mastectomies nor node dissection. Check out our stage IV and you will see that this is a common scenario. -
Cancer in the nodes of your chest and neck do not make stage IV. Otherwise, I too would be stage IV.
From my understanding, they have nothing to go on to say that she is stage IV and should therefore have a different tx plan. These chest nodes are difficult to get to which is why they don't normally do surgery for them. That is what the chemo and rads is for. Unfortunately, the axillary nodes are a question until they get to the pathologist. Niether should they eliminate tx decisions because they "think" she may be stage IV. A lot us stage IIIs live on that edge.
















Categories
- All Categories
- 679 Advocacy and Fund-Raising
- 289 Advocacy
- 68 I've Donated to Breastcancer.org in honor of....
- Test
- 322 Walks, Runs and Fundraising Events for Breastcancer.org
- 5.6K Community Connections
- 282 Middle Age 40-60(ish) Years Old With Breast Cancer
- 53 Australians and New Zealanders Affected by Breast Cancer
- 208 Black Women or Men With Breast Cancer
- 684 Canadians Affected by Breast Cancer
- 1.5K Caring for Someone with Breast cancer
- 455 Caring for Someone with Stage IV or Mets
- 260 High Risk of Recurrence or Second Breast Cancer
- 22 International, Non-English Speakers With Breast Cancer
- 16 Latinas/Hispanics With Breast Cancer
- 189 LGBTQA+ With Breast Cancer
- 152 May Their Memory Live On
- 85 Member Matchup & Virtual Support Meetups
- 375 Members by Location
- 291 Older Than 60 Years Old With Breast Cancer
- 177 Singles With Breast Cancer
- 869 Young With Breast Cancer
- 50.4K Connecting With Others Who Have a Similar Diagnosis
- 204 Breast Cancer with Another Diagnosis or Comorbidity
- 4K DCIS (Ductal Carcinoma In Situ)
- 79 DCIS plus HER2-positive Microinvasion
- 529 Genetic Testing
- 2.2K HER2+ (Positive) Breast Cancer
- 1.5K IBC (Inflammatory Breast Cancer)
- 3.4K IDC (Invasive Ductal Carcinoma)
- 1.5K ILC (Invasive Lobular Carcinoma)
- 999 Just Diagnosed With a Recurrence or Metastasis
- 652 LCIS (Lobular Carcinoma In Situ)
- 193 Less Common Types of Breast Cancer
- 252 Male Breast Cancer
- 86 Mixed Type Breast Cancer
- 3.1K Not Diagnosed With a Recurrence or Metastases but Concerned
- 189 Palliative Therapy/Hospice Care
- 488 Second or Third Breast Cancer
- 1.2K Stage I Breast Cancer
- 313 Stage II Breast Cancer
- 3.8K Stage III Breast Cancer
- 2.5K Triple-Negative Breast Cancer
- 13.1K Day-to-Day Matters
- 132 All things COVID-19 or coronavirus
- 87 BCO Free-Cycle: Give or Trade Items Related to Breast Cancer
- 5.9K Clinical Trials, Research News, Podcasts, and Study Results
- 86 Coping with Holidays, Special Days and Anniversaries
- 828 Employment, Insurance, and Other Financial Issues
- 101 Family and Family Planning Matters
- Family Issues for Those Who Have Breast Cancer
- 26 Furry friends
- 1.8K Humor and Games
- 1.6K Mental Health: Because Cancer Doesn't Just Affect Your Breasts
- 706 Recipe Swap for Healthy Living
- 704 Recommend Your Resources
- 171 Sex & Relationship Matters
- 9 The Political Corner
- 874 Working on Your Fitness
- 4.5K Moving On & Finding Inspiration After Breast Cancer
- 394 Bonded by Breast Cancer
- 3.1K Life After Breast Cancer
- 806 Prayers and Spiritual Support
- 285 Who or What Inspires You?
- 28.7K Not Diagnosed But Concerned
- 1K Benign Breast Conditions
- 2.3K High Risk for Breast Cancer
- 18K Not Diagnosed But Worried
- 7.4K Waiting for Test Results
- 603 Site News and Announcements
- 560 Comments, Suggestions, Feature Requests
- 39 Mod Announcements, Breastcancer.org News, Blog Entries, Podcasts
- 4 Survey, Interview and Participant Requests: Need your Help!
- 61.9K Tests, Treatments & Side Effects
- 586 Alternative Medicine
- 255 Bone Health and Bone Loss
- 11.4K Breast Reconstruction
- 7.9K Chemotherapy - Before, During, and After
- 2.7K Complementary and Holistic Medicine and Treatment
- 775 Diagnosed and Waiting for Test Results
- 7.8K Hormonal Therapy - Before, During, and After
- 50 Immunotherapy - Before, During, and After
- 7.4K Just Diagnosed
- 1.4K Living Without Reconstruction After a Mastectomy
- 5.2K Lymphedema
- 3.6K Managing Side Effects of Breast Cancer and Its Treatment
- 591 Pain
- 3.9K Radiation Therapy - Before, During, and After
- 8.4K Surgery - Before, During, and After
- 109 Welcome to Breastcancer.org
- 98 Acknowledging and honoring our Community
- 11 Info & Resources for New Patients & Members From the Team