Oncotype DX Roll Call!
Comments
-
My OncoDX score was 18. Although my onc very much wanted me to do 10 rounds of TC, I said no. When the rad onc said I was too young (44) for Mammosite radiation, I joined a clinical trial, randomized in, and had that. I am now suffering from awful SEs of Tamox and had a trip to the ER just to get some pain meds to get me through until I could see my doc this afternoon. Sigh.
-
Thanks jpann39 I will add this to your score. I know it has helped me, so hopefully others will benefit also.
I hope your holidays were "magical"!!!!
-
Moody--
I posted a reply to mbradford on the "please help!" thread, citing an article I recently found on http://cancerfighter.wordpress.com/2008/8/29/chemotherapy-criticised-by-australian-oncologists
I'm not sure that's the complete URL, but you can find the article by entering the headine, "Chemotherapy criticised by Australian oncologists," in your browser. It emphasizes the same point about the failure to distinguish between absolute and relative benefit.
I was considering posting on it, but thought that might get me suspected of being an anti-chemotherapy mole. As Sgt. Friday used to say,"I'm just interested in the facts, Ma'am."
-
Hi Thanks for all of your hard work. My Onc Type score is 19. I started Tamoxifen in Nov. and am doing fine!! You are doing a great job with this Thread, we are all learning alot!!!! Thanks, Dawn
-
Seabee,
You asked how positive my Her-2 was. It was 3++.
-
dawn and shari, welcome and thanks for sharing your info with us. I have added you to the roll call.

I am glad that we are all gathering so much info, I know it is helping me as I have decided to go back and finish the rest of my Herceptin tx's. I took 2 months off thinking I would just be done, after all I did 9 of the 18. But after all the stories and articles you guys have shared here, I have decided if I can do 9, I can do 18....
christianne, welcome. You may have posted here before, cant rem and too late at night for me to go back and see. Anyway, Id rather say "hi" twice than not at all...LOL
-
Sorry, everybody--I've been on vacation for a couple of weeks and I haven't been doing any homework assignments.
I want to go back to the question of whether we are misinterpreting our Oncotype scores. On page 3 of this thread, mbradford12000 was quoted as having said this:
"If you look on the second page of the report, you will see TWO graphs. It is the second graph, the one on the right that shows absolute benefit, that is the one that shows whether or not chemo will change your chance of recurrence. Although the graph on the left is not clearly labeled this way, according to my oncologist's explanation, that graph only shows relative benefit. Here's the difference.
The graph on the left looks ONLY at the people who have had a recurrence. So, let me use my case as an example. In my case, with a score of 28, I know from page 1 that 18 out of 100 people with breast cancer like mine get a recurrence. According to the left hand graph on the second page, recurrence was decreased by about 6 percent by having chemo plus tamoxifen.
But here is the crucial piece of information. This means 6 percent of the 18 who got a recurrence, not 6 percent of the original 100. ...
That is what the graph on the right on page 2, absolute benefit, clarifies."
Okay, first of all, I'm not absolutely certain which graphs mbradford is referring to. The graphs I'm posting below are from page 2 of the "sample" Oncotype report on the Genomic Health website. BTW, both the graphs are from this article: S. Paik et al. "Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer." Journal of Clinical Oncology Vol. 24 No. 23 Aug. 10, 2006; pp. 1-12.
This is the figure on the left-hand side of page 2 of the report. (Please correct me if this isn't the graph in your report.):
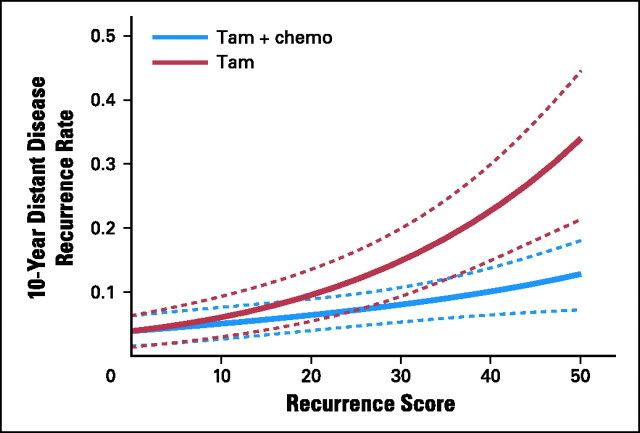
This graph does not show "relative benefit." It is a graph of the 10-year absolute risk of recurrence plotted against the Oncotype recurrence score. The red (dark pink?) solid line is the recurrence risk in women who got Tamoxifen but did not get chemo. The blue solid line is the recurrence risk in women who got both chemo and Tamoxifen. The benefit of chemo is the difference--the vertical gap--between those two lines, for any given Oncotype score.
The dashed lines in the graph are the 95% confidence intervals for the respective pink and blue lines. I'm not very good at explaining statistics. Basically, the confidence intervals tell you that the red and blue lines are probably not correct--there is a 95% likelihood that the actual, true recurrence risks lie somewhere between the dashed lines; they are not necessarily on the solid lines.
There are some unusual things about the graph. One is that the recurrence risk--on the vertical axis--is expressed as a decimal fraction instead of the percentages we usually see. So, if page 1 of the report said your risk of recurrence was 17%, it would appear as 0.17 on the vertical axis on this graph. A recurrence risk of 40% would be 0.4.
Another thing that makes this graph interesting is that the horizontal axis shows Oncotype Recurrence Scores as a continuous variable, instead of grouped into the 3 categories of low, medium, and high. The researchers knew that all the scores within a category did not carry the same risk. Scores of 18 and 30 are both in the "intermediate risk" category, but the actual recurrence risks for those scores are quite different: 18 is an 11% risk; 30 is a 20% risk. So, plotting the scores on a continuous scale is more helpful.
The bottom line with this graph is, the closer together the red and blue lines are, the less benefit there is likely to be from chemo. When the solid lines overlap, there is no benefit. The confidence intervals show how much uncertainty there is in these measurements... and how much more we need to know.
This next pair of graphs, below, is from the same article. The top graph ("A") is not in the Oncotype report. It shows the relative benefit of chemo, for women whose scores are in the 3 categories. The relative benefit is another way of expressing a change in the risk of recurrence. This time, the researchers are displaying recurrence risk on the horizontal axis as a relative value. I'm pretty sure--but not positive--that the value is a ratio of the recurrence risk with chemo, divided by the recurrence risk without chemo. So, if the recurrence risk with chemo was 15% and the recurrence risk without chemo was 20%, the relative benefit of chemo in this graph would be 15/20 or 0.75. If the risk with chemo was 10% and the risk without chemo was 30%, the relative benefit of chemo would be 10/30 = 0.33. The value "1.0" means there was no difference with chemo. A value > 1.0 means the recurrence risk was actually greater with chemo than without chemo. Look at the huge error bars, though--there is enormous variation in the results for the low and intermediate categories.
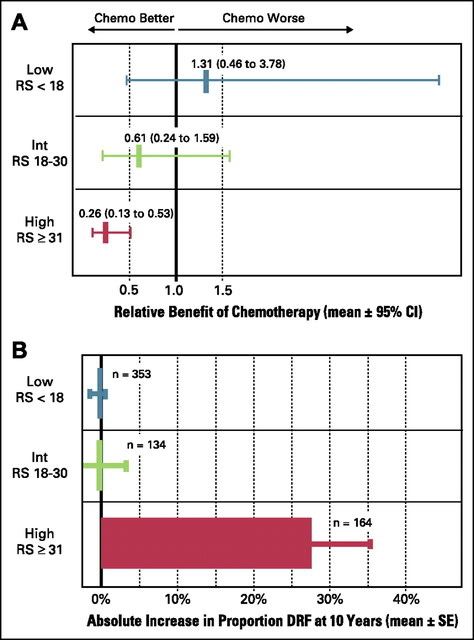
The bottom graph ("B") is the right-hand graph on page 2 of the Oncotype report. It shows the effect chemo has on the absolute risk of recurrence. On the horizontal axis, "DRF" = distant recurrence-free. The horizontal axis is the additional percentage of women who were free of distant recurrence after 10 years--that is, the difference between the percentage that were recurrence-free after chemo and tamoxifen and the percentage that were recurrence-free after only tamoxifen.
As mbradford said, only women in the "high risk" category showed a dramatic improvement in absolute risk of recurrence, with chemo (i.e., benefit from chemo). Women in the "low risk" category showed no improvement at all in their risk. It looks like women in the "intermediate risk" group also had no benefit from chemo, but we know that the benefit in that group varies, depending on whether the Oncotype score is at the low or high end of that range. (See the large error bars.) Also, as mbradford said, the TAILORx trial will hopefully clarify the benefit of chemo in that group.
I am sorry this is so long and wordy. Please post or PM if you are still confused.
otter
-
Thank you Otter for all the time you spent on this. We appreciate you! Welcome back and OBTW...."CLEAN SCAN". Yipee!
Artsee
-
Hi Otter, welcome back, and thanks for that very detailed and instructive look at those graphs. You are indeed right in assuming that the first graph, and graph B, are the ones on p. 2 of the Oncotype report.
The second one is modified slightly, in that it is rotated to a vertical view and the decimals are expressed as percentages, but it is otherwise the same.
I think the point that mbradford is getting at is not that the graphs are misleading, but that they can be interpreted in a misleading way that makes the improvement seem greater than it is. Take for example the first graph. Someone with a score of 30 has a recurrence risk of 20%. Tamoxifen (on the average) reduces this to a 15% rate of recurrence. One might say that in relative terms Tam has reduced the risk by 25%, whereas absolute terms it has only reduced the rate by 5%.
Chemo, according to the first chart, drops the rate of recurrence down to 7%, so one might say in relative terms that chemo has reduced the risk by another 40%, whereas in absolute terms it has only reduced the rate by an additional 8%. However, a 13% overall absolute reduction in risk is pretty good. It just doesn't sound as good as a risk reduction of 65%.
If your oncotype score is thirty you should definitely do chemo according to this graph. The confusion of relative and absolute risk becomes more critial for lower scores.
A score of 22, for example, has a recurrence risk of 12%. Tam reduces this to 10% for an absolute gain of 2%. However, since 2 is 17% of 12, one could say thatTam had reduced the risk by 17%. Chemo further reduces the rate of recurrence to 7%, for an absolute gain of 3%. However, in relative terms one could say that chemo has reduced the risk an additional 25%. This sounds a lot better than a total absolute gain of 5%, which has to be weighed against the risks of side effects.
The Australian article I referenced takes an extreme view, but it does make a point about understanding the difference betweeen relative and absolute benefit.
-
You can add me to the roll call....jst got back from Oncologist and my Ocncotype is 26! Ugh!! He is recomending 4 doses of Cytoxan/Taxotere....3 weeks apart. He said the choice was mine.....
I asked him what would her recommend if I was his daughter.....he said he would tell her to do the chemo.....
Any thoughts you ll have would be welcome. I'm a little new to this stuff and it all seems like greek and you all seem to be very learned on it all...help!
-
Alo123, my Oncotype score was also 26, and I had 4 rounds of Taxotere/Cytoxan (3 wks apart). I finished last June. It's bad--after all, it's CHEMO ... but it wasn't as bad as I feared it would be.
Seabee, thanks for the added discussion of absolute vs. relative benefit. Sometimes it's very difficult to tell which is being used when the results of a study are discussed, especially if it's in a news article. All the headlines and shouting about a "40% improvement" can end up looking pretty pale when you see the actual data and realize they're talking about a relative benefit.
Fortunately, my onco was pretty clear. She said with an Oncotype score of 26, I had a 17% chance of a distant recurrence even after tamoxifen. (The recurrence risks reported by Genomic Health for their Oncotype scores are for women who've had 5 years of tamoxifen.) She told me chemo would decrease that risk by about one-third, bringing it down to around 12%. Later I rechecked that "one-third" figure, and found it was pretty close to the chemo benefit calculated for me by the Adjuvant!Online calculator.
otter
-
Al0123 - I have my Oncologist meeting tomorrow. My score is 23 and I am pretty sure my oncologist is going to NOT recommend chemo. I am basing this on my tape of our conversation before we got the oncotype score back.
I hate having to make this decision. I feel like chosing chemo so that at least I feel like I did all I could at this point, however if it is a slim margin of improvement, is it worth it? Did your oncologist give you recurrence % (such as 17% recurrence just tamoxifen and 11% recurrence with chemo and tamoxifen). I am trying to figure that out.
Good luck with your decision - sorry I can't be more help!
Susan
-
My oncotype was 19, with a 12% chance of recurrence with 5 years of tamoxifen. Both of the oncologists I consulted said that adding chemo would probably only bring it down to 10% at best. They recommended against chemo, saying that if you only are going to get a 2% benefit, your chances of having some kind of serious problems from the chemo are close to 2%, and in their eyes that suggests that it isn't worth doing.
-
Kamico3 - I kind of had it in my head that if my score came back under 20, I would not do chemo, so I know my oncologist would agree with you and your doctor. As a 23 my numbers are a bit higher, but I'm not sure how much higher. My onc. also quoted the low benefit with serious SE at 2% as well. SIGH
I guess I'll see what she says tomorrow. Does age factor into this? I am 44 and my kids are 9 and 11.
-
I think I will do the chemo! As much as I know I willnot enjoy it.....I'm not up for the gamble. If I can reduce my risk by any percent....isn't it worth a few months of hell?! I don't know, but I'm gonna do it.
Otter, it seems from reading your posts that you are very well informed. Thanks for your input....
-
This is making my brain hurt...I still have dain bramage from chemo that my not have done me any good.....
-
Kamico3! I am exactly what you are. 19Oncotype with 5 years of tamoxifen, chemo would be of no benefit, as far as my oncologist sees it. I had a mastectomy with an expander in Sept. and I will have my exchange on the 20th!!Yeah! My oncologist feels that my cancer will not reoccur, of course there are no' garuntees 'in life. Thanks for your input it nice to have reinforcement,for my decision! God Luck! Dawn
-
Alo123, welcome to the roll call, I got you added. Sorry it took me so long, I didnt see your post till right now. Thanks for sharing your info with us and for participating in the roll call!
Otter and Seabee, because of the two of you and your way of explaining things, I think I FINALLY got it!!! LOL I am so glad you guys are here as you have been sooooo helpful!!!! BUT I still need a bit more clarification (sorry).
Here are the stats written on my paper:
Bi-lat mastectomy only : 75% no recur, 25% of recur
Mast + Tamox (5 yrs): reduces 25% to 15% risk of recur (I thought this meant going from 75/25 to 85/15
Mast + Chemo: reduces 25% to 16.1% risk of recur ( I thought this meant going from 75/25 to 84/16)
Mast + Combined therapy: reduces 25% to 9% risk of recur (thought this meant going from 75/25 to 91/9
All of the above + Herceptin: reduces 25% to 4.5% (but I wrote down 96/4)
And Mast + chemo + Herceptin (no Tamox): gave me 92/8 - which is what I chose
So which way is this?
Edited b/c when I got home tonight, I looked at my paper again, & I didnt post the above correctly the first time. "Bold" will indicate the "revised". LOL
-
It is always nice to hear of someone who is in the same or a very similar situation and who got the same advice! I guess the bottom line is that different doctors have different takes on things and we all also have to examine what risks we feel we face and which risks we can tolerate better than others. I was absolutely paralyzed in terms of making a decision re chemo or no chemo, so the fact that my doctors at Dana Farber were so definite in recommending against it was a relief to me, as it gave me something to use as my decision point, so to speak. That doesn't mean, though, that I don't read these posts and freak out when I see that other people in my situation went ahead and had the chemo. I second guess myself every day, actually. If my cancer recurs, will I kick myself for not having had the chemo? You betcha! Will I then end up being able to rationalize my decision by saying , well, I probably would have had a recurrence even if I had had the chemo? Probably! Am I sure I made the right decision? No, not really. I hope so.
-
Moody, thanks for the compliments, but I don't think I can help much with deciphering your numbers. I don't know where your onco (surgeon?) got them, and I've been unable to replicate them with any of the on-line risk calculators.
The Adjuvant!Online website calculates risk of recurrence, but it doesn't take HER2 status or Herceptin into account and the chemo and hormonal therapy formulas are out-of-date. The only other detailed risk calculator I'm aware of is the Cancermath.net site, and it doesn't calculate recurrence risk--it figures lifespan and calculates additional years of life "rescued" by various treatments.
So, neither of those will provide the numbers you've been given.
I'm wondering if your onco didn't just estimate some of those numbers. Maybe you can ask where they came from? From what you've been told, the benefits of chemo, tamoxifen, and combined tamox+chemo seem very, very good. If you add Herceptin to that mix, you have a recurrence risk that's extraordinarily low (4%).
I just don't understand why tamoxifen alone (no chemo, no Herceptin) can lower your risk from 25% down to 15%--which is a 10% absolute benefit and a 40% relative benefit (correct, Seabee?), but according to the numbers you've been given, when added to chemo and Herceptin, the absolute benefit of Tamoxifen is just 4%. The 40% relative benefit from tamoxifen alone is what the Adjuvant!Online calculator says there would be. I know the benefits of all those treatments are not additive--I wish they were--but I don't understand why the benefit of tamoxifen drops that much when you add it to chemo + Herceptin.
Or (this is otter, thinking out loud), maybe another way to look at it is that, for a HER2+ tumor, chemo and Herceptin play a much greater role than estrogen blockade? HER2+ tumors are typically more aggressive, so, as with high-Oncotype tumors, maybe Tamoxifen has less of an effect despite the ER+ status?
I do have a concern that all these numbers have huge statistical errors associated with them. Much of this stuff, especially the newer chemo regimens, the Herceptin benefits, and the complex combinations, haven't been studied long enough to have reliable data on recurrence risk and survival. Add to that the fact that ER+ HER2+ tumors aren't all that common, and I think the "database" on which the calculations are based may be flimsy.
That's just IMHO, though. At some point, we just have to decide whom to trust and we make a decision.
Hugs...
otter
-
Kamico3!Don't second guess yourself, you made the right decision based on the facts that you had at the time. I am a nurse and have had some experience with chemo, and I have seen reoccrrance even with chemo. Once you are a member of this club it never leaves you, unfortunately. I used to work at BI that is afilliated with The Farber, and it is a wonderful place,if your MDs are steering against chemo,I'd follow their advice. My MDs are from Dartmouth-Hitchcock,and are suggesting the same thing, so based on their opions we both have made the right decision. I like you was unsure,but after seeing first hand and figuring %, I opted to have no chemo as the oncologist advised.Did you have a mastectomy or lumpectomy? Which ever way you went was right too! this is so daunting, that you cn't eat yourself up all of the time,I find these decisions have been the hardest ones I've ever made. Keep the Faith! Dawn
-
Thanks for your kind words, Dawn! I had a lumpectomy... that was hard to choose, too, but that also went along with the advice I was being given. It's funny... I always used to say that if I ever got breast cancer (not that I ever thought I was going to!) I would just get a mastectomy automatically, but once it had actually happened, I found that I felt differently about it and wanted to preserve my breast if it made sense to do so.
-
Moody--like Otter I can't tell where some of those figures come from, but if you'll look at the first graph that Otter reproduced for us, you'll see that your survival/risk split may be correct. Your DX score of 36 indicates a 25% risk of recurrence with surgery only According to the graph, Tam reduces this to about 18%, for an absolute gain of 7. Tamox plus chemo further reduces the risk to 8%, for an absolute gain of 10. This would give you the 92/8 split you note for "combined therapy," and your oncologist seems to be suggesting that chemo plus Herceptin will work as well as Tamox plus chemo, thus giving you the same favorable odds. This is probably based on some of the research on Herceptin, which I'm not very familiar with since I'm HER2-
I can't do anything with the percentages of "benefit," but your odds of recurrence-free survival seem excellent.
-
I had my big meeting to discuss my oncotype 23 and chemo and the Oncologist recommended chemo, so I started CMF today. So far,I feel fine!
It gives me peace of mind and did make statistical sense after all!
I have learned so much from this thread (and this board). Thank you to all!
Susan
-
otter wrote:
Moody, thanks for the compliments, but I don't think I can help much with deciphering your numbers. I don't know where your onco (surgeon?) got them, and I've been unable to replicate them with any of the on-line risk calculators.
Seabee wrote:
Moody--like Otter I can't tell where some of those figures come from, but if you'll look at the first graph that Otter reproduced for us, you'll see that your survival/risk split may be correct.
LMBO otter and seabee as that makes three of us!
But what I can tell you is how my onc explained the way Herceptin changed the %. Basically, Hercep reduces the recur risk % by an additional 50%. In other words, if chemo reduced my 25% risk recur down to a 16% risk recur, then Herceptin would reduce the 16% down to 8% risk of recurrence. And if chemo + tamox reduced the 25% down to 8%, then Herceptin would reduce 8% down to 4% chance of recurrence. Does that make sense? It made sense to me, but THAT doesnt mean anything!

-
There IS a problem with the way we're interpreting the scores.
The "recurrence risk" represented by an Oncotype score is the rate of distant recurrence (metastasis) at 10 years in women who have had surgery (with or without rads) plus 5 years of tamoxifen. There is nothing in the Oncotype report that mentions recurrence risk after surgery alone (no tamoxifen and no chemo). That's because the data used for validating the Oncotype DX test included only women who had been on tamoxifen for 5 years.
So, Moody, this means the Oncotype scores and % recurrence values you posted at the top of this thread refer to the risk after surgery and 5 years of tamoxifen. Those recurrence risks are not for women with no treatment except surgery.
Recurrence data and tumor blocks from the NSABP-B14 clinical trial were used in the original validation testing. The NSABP-B14 trial studied the benefit of tamoxifen versus no tamoxifen in women with BC, but only the data and samples from the tamoxifen-treated women were used by Genomic Health in the Oncotype validation.
Data and samples from a different clinical trial, the NSABP-B20 trial, were used to test the relationship between Oncotype score and benefit from chemo. The NSABP-B20 trial compared the benefit of tamoxifen alone to the benefit of tamoxifen plus chemo. So, all the data from the NSABP-B20 trial were from women who had been treated with tamoxifen.
The graph I posted that has the blue and red lines is not a standard curve--it shouldn't be used to relate Oncotype scores to recurrence risks. It was a statistically generated plot to show trends, I think. So, I don't think we're supposed to use it to calculate our actual recurrence risk before and after chemo.
As Seabee has observed, the recurrence risk associated with an Oncotype score of 36 is approximately 18% (after tamoxifen) if taken from the red line on that graph. However, according to the graph on page 1 of the Oncotype report (on my copy and on the Genomic Health website), an Oncotype score of 36 actually represents a 10-year risk of distant recurrence of 25%, and that is after 5 years of tamoxifen. The risk with surgery alone--no tamoxifen--is considerably greater.
So, something is amiss with the numbers Moody was given. They just aren't right, according to the data from Genomic Health. Moody, have you seen your original Oncotype report--the one FAXed to your doc by Genomic Health?
otter
-
Well see otter all of this seems to be my onco's fault! He gave me ONE sheet of paper with a graph on it (sure does look EXACTLY like the AdjuvantOnline-graph) BUT he WROTE on the paper "Oncotype DX Assay" SO, I, not knowing about any of these things 11 months ago, thought that this piece of paper was my Oncotype DX..........
How the heck was I suppose to know, when I never studied up on cancer testing before.....duh....
SOOOOOO I am thinking he , ehm, may have NOT actually sent off for the Oncotype DX?!?!?!? But I can tell you this, When I go back Tuesday, I will ----ehm, tell him how I want him to give me the Oncotype DX 4 page report that he would have gotten from them..........and see what he says......

-
I was away for the holidays and just saw this roll roll...
my oncotype DX score was 19 (April 2005) - I had a lumpectomy, declined chemo, total hysterectomy, full breast rads and am taking Arimidex.
Doreen
-
Hi DoreenF I am glad you found us. Thanks for joining the roll call, I got you added. So since 2005 no recurrence? Awesome!
-
Moody- I think it is great you have this posting!
What to do after this oncotype test filled my mind with so many questions. I am sure everyone goes through all these ????????
Up so this point I had put so much confidence into just doing what the doctors said was best for me. It was the first time I had to make a decision that would determine by future. It was huge for me.
After reading all the material - and there is so much out there, and so much yet to be determined especially in what I call the gray area >10 and < 25- I hope I made the right decision not to do chemo. I like many of you had talked to lots of people who said just wanted to treat knowing I had done all I can. (example full masectomy to know that I had gotten it all.) (and the same thing with oncotype test to be sure I had left nothing undone in my treatment)
Yet with todays validation studies and what they know know. I was told also that with the size of my tumor my doctor said "my survival rate was the same" with lupectomy as full masectomy. And the doctors said the choice was mine after oncotype score of 14, but very little if ANY benefit from chemo for me.
My tumor size was 1.8cm, Stage 1C, oncotype score 14, recurrence percentage 9%
This decision though is still heavy on my mind- so I value reading each story of how you all also struggled with this choice.
Thanks also for the Bible verse Moody- That is powerful. I too have grown closer to God each trial of the way. For me the song Amazing Grace has touched me powerfully. I listen to it all the time on my I Pod waiting at all my appointments and find strength.











Categories
- All Categories
- 679 Advocacy and Fund-Raising
- 289 Advocacy
- 68 I've Donated to Breastcancer.org in honor of....
- Test
- 322 Walks, Runs and Fundraising Events for Breastcancer.org
- 5.6K Community Connections
- 282 Middle Age 40-60(ish) Years Old With Breast Cancer
- 53 Australians and New Zealanders Affected by Breast Cancer
- 208 Black Women or Men With Breast Cancer
- 684 Canadians Affected by Breast Cancer
- 1.5K Caring for Someone with Breast cancer
- 455 Caring for Someone with Stage IV or Mets
- 260 High Risk of Recurrence or Second Breast Cancer
- 22 International, Non-English Speakers With Breast Cancer
- 16 Latinas/Hispanics With Breast Cancer
- 189 LGBTQA+ With Breast Cancer
- 152 May Their Memory Live On
- 85 Member Matchup & Virtual Support Meetups
- 375 Members by Location
- 291 Older Than 60 Years Old With Breast Cancer
- 177 Singles With Breast Cancer
- 869 Young With Breast Cancer
- 50.4K Connecting With Others Who Have a Similar Diagnosis
- 204 Breast Cancer with Another Diagnosis or Comorbidity
- 4K DCIS (Ductal Carcinoma In Situ)
- 79 DCIS plus HER2-positive Microinvasion
- 529 Genetic Testing
- 2.2K HER2+ (Positive) Breast Cancer
- 1.5K IBC (Inflammatory Breast Cancer)
- 3.4K IDC (Invasive Ductal Carcinoma)
- 1.5K ILC (Invasive Lobular Carcinoma)
- 999 Just Diagnosed With a Recurrence or Metastasis
- 652 LCIS (Lobular Carcinoma In Situ)
- 193 Less Common Types of Breast Cancer
- 252 Male Breast Cancer
- 86 Mixed Type Breast Cancer
- 3.1K Not Diagnosed With a Recurrence or Metastases but Concerned
- 189 Palliative Therapy/Hospice Care
- 488 Second or Third Breast Cancer
- 1.2K Stage I Breast Cancer
- 313 Stage II Breast Cancer
- 3.8K Stage III Breast Cancer
- 2.5K Triple-Negative Breast Cancer
- 13.1K Day-to-Day Matters
- 132 All things COVID-19 or coronavirus
- 87 BCO Free-Cycle: Give or Trade Items Related to Breast Cancer
- 5.9K Clinical Trials, Research News, Podcasts, and Study Results
- 86 Coping with Holidays, Special Days and Anniversaries
- 828 Employment, Insurance, and Other Financial Issues
- 101 Family and Family Planning Matters
- Family Issues for Those Who Have Breast Cancer
- 26 Furry friends
- 1.8K Humor and Games
- 1.6K Mental Health: Because Cancer Doesn't Just Affect Your Breasts
- 706 Recipe Swap for Healthy Living
- 704 Recommend Your Resources
- 171 Sex & Relationship Matters
- 9 The Political Corner
- 874 Working on Your Fitness
- 4.5K Moving On & Finding Inspiration After Breast Cancer
- 394 Bonded by Breast Cancer
- 3.1K Life After Breast Cancer
- 806 Prayers and Spiritual Support
- 285 Who or What Inspires You?
- 28.7K Not Diagnosed But Concerned
- 1K Benign Breast Conditions
- 2.3K High Risk for Breast Cancer
- 18K Not Diagnosed But Worried
- 7.4K Waiting for Test Results
- 603 Site News and Announcements
- 560 Comments, Suggestions, Feature Requests
- 39 Mod Announcements, Breastcancer.org News, Blog Entries, Podcasts
- 4 Survey, Interview and Participant Requests: Need your Help!
- 61.9K Tests, Treatments & Side Effects
- 586 Alternative Medicine
- 255 Bone Health and Bone Loss
- 11.4K Breast Reconstruction
- 7.9K Chemotherapy - Before, During, and After
- 2.7K Complementary and Holistic Medicine and Treatment
- 775 Diagnosed and Waiting for Test Results
- 7.8K Hormonal Therapy - Before, During, and After
- 50 Immunotherapy - Before, During, and After
- 7.4K Just Diagnosed
- 1.4K Living Without Reconstruction After a Mastectomy
- 5.2K Lymphedema
- 3.6K Managing Side Effects of Breast Cancer and Its Treatment
- 591 Pain
- 3.9K Radiation Therapy - Before, During, and After
- 8.4K Surgery - Before, During, and After
- 109 Welcome to Breastcancer.org
- 98 Acknowledging and honoring our Community
- 11 Info & Resources for New Patients & Members From the Team